What you need to know about research dissemination
Last updated
5 March 2024
Reviewed by
In this article, we'll tell you what you need to know about research dissemination.
- Understanding research dissemination
Research that never gets shared has limited benefits. Research dissemination involves sharing research findings with the relevant audiences so the research’s impact and utility can reach its full potential.
When done effectively, dissemination gets the research into the hands of those it can most positively impact. This may include:
Politicians
Industry professionals
The general public
What it takes to effectively disseminate research will depend greatly on the audience the research is intended for. When planning for research dissemination, it pays to understand some guiding principles and best practices so the right audience can be targeted in the most effective way.
- Core principles of effective dissemination
Effective dissemination of research findings requires careful planning. Before planning can begin, researchers must think about the core principles of research dissemination and how their research and its goals fit into those constructs.
Research dissemination principles can best be described using the 3 Ps of research dissemination.
This pillar of research dissemination is about clarifying the objective. What is the goal of disseminating the information? Is the research meant to:
Persuade policymakers?
Influence public opinion?
Support strategic business decisions?
Contribute to academic discourse?
Knowing the purpose of sharing the information makes it easy to accurately target it and align the language used with the target audience.
The process includes the methods that will be used and the steps taken when it comes time to disseminate the findings. This includes the channels by which the information will be shared, the format it will be shared in, and the timing of the dissemination.
By planning out the process and taking the time to understand the process, researchers will be better prepared and more flexible should changes arise.
The target audience is whom the research is aimed at. Because different audiences require different approaches and language styles, identifying the correct audience is a huge factor in the successful dissemination of findings.
By tailoring the research dissemination to the needs and preferences of a specific audience, researchers increase the chances of the information being received, understood, and used.
- Types of research dissemination
There are many options for researchers to get their findings out to the world. The type of desired dissemination plays a big role in choosing the medium and the tone to take when sharing the information.
Some common types include:
Academic dissemination: Sharing research findings in academic journals, which typically involves a peer-review process.
Policy-oriented dissemination: Creating documents that summarize research findings in a way that's understandable to policymakers.
Public dissemination: Using television and other media outlets to communicate research findings to the public.
Educational dissemination: Developing curricula for education settings that incorporate research findings.
Digital and online dissemination: Using digital platforms to present research findings to a global audience.
Strategic business presentation: Creating a presentation for a business group to use research insights to shape business strategy
- Major components of information dissemination
While the three Ps provide a convenient overview of what needs to be considered when planning research dissemination, they are not a complete picture.
Here’s a more comprehensive list of what goes into the dissemination of research results:
Audience analysis : Identifying the target audience and researching their needs, preferences, and knowledge level so content can be tailored to them.
Content development: Creating the content in a way that accurately reflects the findings and presents them in a way that is relevant to the target audience.
Channel selection: Choosing the channel or channels through which the research will be disseminated and ensuring they align with the preferences and needs of the target audience.
Timing and scheduling: Evaluating factors such as current events, publication schedules, and project milestones to develop a timeline for the dissemination of the findings.
Resource allocation: With the basics mapped out, financial, human, and technological resources can be set aside for the project to facilitate the dissemination process.
Impact assessment and feedback: During the dissemination, methods should be in place to measure how successful the strategy has been in disseminating the information.
Ethical considerations and compliance: Research findings often include sensitive or confidential information. Any legal and ethical guidelines should be followed.
- Crafting a dissemination blueprint
With the three Ps providing a foundation and the components outlined above giving structure to the dissemination, researchers can then dive deeper into the important steps in crafting an impactful and informative presentation.
Let’s take a look at the core steps.

1. Identify your audience
To identify the right audience for research dissemination, researchers must gather as much detail as possible about the different target audience segments.
By gathering detailed information about the preferences, personalities, and information-consumption habits of the target audience, researchers can craft messages that resonate effectively.
As a simple example, academic findings might be highly detailed for scholarly journals and simplified for the general public. Further refinements can be made based on the cultural, educational, and professional background of the target audience.
2. Create the content
Creating compelling content is at the heart of effective research dissemination. Researchers must distill complex findings into a format that's engaging and easy to understand. In addition to the format of the presentation and the language used, content includes the visual or interactive elements that will make up the supporting materials.
Depending on the target audience, this may include complex technical jargon and charts or a more narrative approach with approachable infographics. For non-specialist audiences, the challenge is to provide the required information in a way that's engaging for the layperson.
3. Take a strategic approach to dissemination
There's no single best solution for all research dissemination needs. What’s more, technology and how target audiences interact with it is constantly changing. Developing a strategic approach to sharing research findings requires exploring the various methods and channels that align with the audience's preferences.
Each channel has a unique reach and impact, and a particular set of best practices to get the most out of it. Researchers looking to have the biggest impact should carefully weigh up the strengths and weaknesses of the channels they've decided upon and craft a strategy that best uses that knowledge.
4. Manage the timeline and resources
Time constraints are an inevitable part of research dissemination. Deadlines for publications can be months apart, conferences may only happen once a year, etc. Any avenue used to disseminate the research must be carefully planned around to avoid missed opportunities.
In addition to properly planning and allocating time, there are other resources to consider. The appropriate number of people must be assigned to work on the project, and they must be given adequate financial and technological resources. To best manage these resources, regular reviews and adjustments should be made.
- Tailoring communication of research findings
We’ve already mentioned the importance of tailoring a message to a specific audience. Here are some examples of how to reach some of the most common target audiences of research dissemination.
Making formal presentations
Content should always be professional, well-structured, and supported by data and visuals when making formal presentations. The depth of information provided should match the expertise of the audience, explaining key findings and implications in a way they'll understand. To be persuasive, a clear narrative and confident delivery are required.
Communication with stakeholders
Stakeholders often don't have the same level of expertise that more direct peers do. The content should strike a balance between providing technical accuracy and being accessible enough for everyone. Time should be taken to understand the interests and concerns of the stakeholders and align the message accordingly.
Engaging with the public
Members of the public will have the lowest level of expertise. Not everyone in the public will have a technical enough background to understand the finer points of your message. Try to minimize confusion by using relatable examples and avoiding any jargon. Visual aids are important, as they can help the audience to better understand a topic.
- 10 commandments for impactful research dissemination
In addition to the details above, there are a few tips that researchers can keep in mind to boost the effectiveness of dissemination:
Master the three Ps to ensure clarity, focus, and coherence in your presentation.
Establish and maintain a public profile for all the researchers involved.
When possible, encourage active participation and feedback from the audience.
Use real-time platforms to enable communication and feedback from viewers.
Leverage open-access platforms to reach as many people as possible.
Make use of visual aids and infographics to share information effectively.
Take into account the cultural diversity of your audience.
Rather than considering only one dissemination medium, consider the best tool for a particular job, given the audience and research to be delivered.
Continually assess and refine your dissemination strategies as you gain more experience.
Should you be using a customer insights hub?
Do you want to discover previous research faster?
Do you share your research findings with others?
Do you analyze research data?
Start for free today, add your research, and get to key insights faster
Editor’s picks
Last updated: 18 April 2023
Last updated: 27 February 2023
Last updated: 6 February 2023
Last updated: 6 October 2023
Last updated: 5 February 2023
Last updated: 16 April 2023
Last updated: 9 March 2023
Last updated: 12 December 2023
Last updated: 11 March 2024
Last updated: 4 July 2024
Last updated: 6 March 2024
Last updated: 5 March 2024
Last updated: 13 May 2024
Latest articles
Related topics, .css-je19u9{-webkit-align-items:flex-end;-webkit-box-align:flex-end;-ms-flex-align:flex-end;align-items:flex-end;display:-webkit-box;display:-webkit-flex;display:-ms-flexbox;display:flex;-webkit-flex-direction:row;-ms-flex-direction:row;flex-direction:row;-webkit-box-flex-wrap:wrap;-webkit-flex-wrap:wrap;-ms-flex-wrap:wrap;flex-wrap:wrap;-webkit-box-pack:center;-ms-flex-pack:center;-webkit-justify-content:center;justify-content:center;row-gap:0;text-align:center;max-width:671px;}@media (max-width: 1079px){.css-je19u9{max-width:400px;}.css-je19u9>span{white-space:pre;}}@media (max-width: 799px){.css-je19u9{max-width:400px;}.css-je19u9>span{white-space:pre;}} decide what to .css-1kiodld{max-height:56px;display:-webkit-box;display:-webkit-flex;display:-ms-flexbox;display:flex;-webkit-align-items:center;-webkit-box-align:center;-ms-flex-align:center;align-items:center;}@media (max-width: 1079px){.css-1kiodld{display:none;}} build next, decide what to build next.

Users report unexpectedly high data usage, especially during streaming sessions.

Users find it hard to navigate from the home page to relevant playlists in the app.

It would be great to have a sleep timer feature, especially for bedtime listening.

I need better filters to find the songs or artists I’m looking for.
Log in or sign up
Get started for free

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- BMC Health Serv Res
Sustainability in Health care by Allocating Resources Effectively (SHARE) 10: operationalising disinvestment in a conceptual framework for resource allocation
Claire harris.
1 School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria Australia
2 Centre for Clinical Effectiveness, Monash Health, Melbourne, Victoria Australia
Sally Green
Adam g. elshaug.
3 Menzies Centre for Health Policy, Sydney School of Public Health, University of Sydney, Sydney, Australia
4 Lown Institute, Brookline, Massachusetts USA
Associated Data
Many of the datasets supporting the conclusions of the articles in the SHARE series are included within the articles and/or the accompanying additional files. Some datasets provide information for more than one article and are only provided once; where they are not included within an article and/or the accompanying additional file, the relevant citations to the articles in which they are provided are included. Datasets have not been made available where it is impossible to de-identify individuals due to the nature of survey or interview responses or where the data is published in confidential internal reports.
This is the tenth in a series of papers reporting a program of Sustainability in Health care by Allocating Resources Effectively (SHARE) in a local healthcare setting. After more than a decade of research, there is little published evidence of active and successful disinvestment. The paucity of frameworks, methods and tools is reported to be a factor in the lack of success. However there are clear and consistent messages in the literature that can be used to inform development of a framework for operationalising disinvestment. This paper, along with the conceptual review of disinvestment in Paper 9 of this series, aims to integrate the findings of the SHARE Program with the existing disinvestment literature to address the lack of information regarding systematic organisation-wide approaches to disinvestment at the local health service level.
A framework for disinvestment in a local healthcare setting is proposed. Definitions for essential terms and key concepts underpinning the framework have been made explicit to address the lack of consistent terminology. Given the negative connotations of the word ‘disinvestment’ and the problems inherent in considering disinvestment in isolation, the basis for the proposed framework is ‘resource allocation’ to address the spectrum of decision-making from investment to disinvestment. The focus is positive: optimising healthcare, improving health outcomes, using resources effectively.
The framework is based on three components: a program for decision-making, projects to implement decisions and evaluate outcomes, and research to understand and improve the program and project activities. The program consists of principles for decision-making and settings that provide opportunities to introduce systematic prompts and triggers to initiate disinvestment. The projects follow the steps in the disinvestment process. Potential methods and tools are presented, however the framework does not stipulate project design or conduct; allowing application of any theories, methods or tools at each step. Barriers are discussed and examples illustrating constituent elements are provided.
Conclusions
The framework can be employed at network, institutional, departmental, ward or committee level. It is proposed as an organisation-wide application, embedded within existing systems and processes, which can be responsive to needs and priorities at the level of implementation. It can be used in policy, management or clinical contexts.
Electronic supplementary material
The online version of this article (doi:10.1186/s12913-017-2506-7) contains supplementary material, which is available to authorized users.
About share
This is the tenth in a series of papers reporting Sustainability in Health care by Allocating Resources Effectively (SHARE). The SHARE Program is an investigation of concepts, opportunities, methods and implications for evidence-based investment and disinvestment in health technologies and clinical practices in a local healthcare setting. The papers in this series are targeted at clinicians, managers, policy makers, health service researchers and implementation scientists working in this context. This paper proposes a framework for operationalising disinvestment in the context of resource allocation in the local healthcare setting.
Although there is no clear single definition, disinvestment is generally understood to be removal, reduction or restriction of technologies and clinical practices (TCPs) that are unsafe or of little benefit, in order to improve patient outcomes and use available resources more efficiently [ 1 ]. Three main areas of opportunity for disinvestment have been identified: 1) TCPs in current use that were not evaluated rigorously prior to their introduction and have subsequently been identified as harmful, ineffective or not cost-effective for all patients or certain subgroups, 2) existing TCPs that are safe, effective and cost-effective but which have alternatives offering greater benefit, and 3) TCPs that are overused or misused [ 1 ].
Following successful implementation of a systematic, integrated, transparent, evidence-based program to assess new TCPs prior to their introduction within the health service [ 2 ], Monash Health, a large health service network in Melbourne Australia, sought to develop a similar program for disinvestment. The ‘Sustainability in Health care by Allocating Resources Effectively’ (SHARE) Program was established to investigate this. An overview of the program and a guide to the SHARE publications are provided in the first paper in this series [ 3 ] and a summary of the findings are in the final paper [ 4 ].
It is common for healthcare networks and individual facilities to make decisions within organisation-wide frameworks; for example introduction of new TCPs and models of care, delivery of programs and services, development and authorisation of policies and procedures, capital expenditure and clinical purchasing. Although disinvestment can be considered in all these contexts, it is frequently reported in individual standalone projects, isolated from other decision-making settings. Monash Health chose to explore disinvestment in the context of organisation-wide systems and processes for all resource allocation decisions.
There was little published information available to guide development of a systematic organisation-wide local approach to disinvestment at Monash Health. In the absence of guidance from the literature, a two-phased process was proposed to identify and then evaluate potential opportunities for disinvestment (Fig. (Fig.1). 1 ). The aim of Phase One was to understand concepts and practices related to disinvestment and the implications for a local health service and, based on this information, to identify potential settings and methods for decision-making. The aim of Phase Two was to develop, implement and evaluate the proposed settings and methods to determine which were sustainable, effective and appropriate at Monash Health.

Overview of SHARE Program
The outcomes of Phase One provide information regarding decision-making settings, decision-makers, scope and type of decisions, strengths and weaknesses in current processes, barriers and enablers, and criteria used for allocating resources within a local health service which, to our knowledge, has not previously been documented to this level of detail in this context [ 5 – 8 ]. While the program had limited success in achieving the aims of Phase Two, the investigation provides in-depth insight into the experience of disinvestment in one local health service and reports the process of disinvestment from identification, through prioritisation and decision-making, to implementation and evaluation, and finally explication of the processes and outcomes [ 9 – 11 ]. These detailed findings enabled development of several frameworks and models for a range of purposes related to disinvestment and resource allocation in the local healthcare setting.
At the completion of these activities, a third phase was undertaken to review the current literature from the perspective of a local health service, and combine it with the published findings from the SHARE Program to address some of the gaps in information about disinvestment in this setting. This review focuses on the practical and operational aspects of disinvestment at the local level. It is a companion to the ninth paper of the SHARE series which provides a conceptual description; disinvestment is introduced and discussed in relation to terminology and concepts, motivation and purpose, relationships with other health improvement paradigms, challenges, and implications for policy, practice and research [ 1 ]. The methods of the literature review are included in Paper 9 and the contents of both reviews are summarised in Table Table1 1 .
Contents of the literature reviews
| SHARE Paper 9. Conceptual perspective |
| ▪ Terminology and concepts – Health technologies – Disinvestment – Resource allocation – Optimising health care – Reinvestment ▪ Motivation and purpose – Impetus for disinvestment – Rationale for disinvestment ▪ Relationships with other healthcare improvement paradigms – Evidence based health care – Quality improvement – System redesign – Health economic approaches ▪ Challenges ▪ New approach to disinvestment |
| SHARE Paper 10. Operational perspective |
| ▪ Existing theories, frameworks and models ▪ New framework ▪ Program – Principles of decision-making – Settings and opportunities – Prompts and triggers – Steps in the disinvestment process ▪ Projects ▪ Research ▪ Methods and tools – Identification of opportunities – Prioritisation and Decision-making – Development of a proposal – Implementation – Monitoring, Evaluation and Reporting – Reinvestment – Dissemination and Diffusion – Maintenance ▪ Barriers and enablers |
Although research and debate has broadened considerably over the past decade, there remains a lack of information to guide healthcare networks or individual facilities in how they might take a systematic, integrated, organisation-wide approach to disinvestment in the context of all resource allocation decisions [ 1 ]. Despite the paucity of evidence in this context, there are clear and consistent messages regarding principles for decision-making, settings and opportunities to identify disinvestment targets, steps in the disinvestment process, barriers and enablers to successful implementation, and some frameworks and models for elements of the disinvestment process. This practical information can be used to develop an organisation-wide framework for operationalising disinvestment in the local healthcare setting.
The aims of this paper are to discuss the current literature on disinvestment from an operational perspective, combine it with the experiences of the SHARE Program, and propose a framework for disinvestment in the context of resource allocation in the local healthcare setting.
Existing theories, frameworks and models
Theories are based on concepts or ideas that characterise a particular phenomenon and propositions or relationships that link the concepts [ 12 ]. No specific theories of disinvestment have been proposed, however resource allocation theory, prioritisation theories, and decision-making theories have been applied in disinvestment projects; examples are listed in Table Table2 2 [ 13 – 18 ].
Examples of theories proposed or applied in disinvestment-related projects
| Theory | Purpose | Context |
|---|---|---|
| Decision-making theory | To guide resource allocation decisions | Health service delivery organisations [ ] |
| Deliberative democratic theory Deliberation theory | To capture stakeholder perspectives | Assisted Reproductive Technologies [ , ] Pathology testing for vitamin B12 and folate [ ] |
| To underpin patient involvement | Priority setting healthcare improvement [ ] | |
| Social constructionist theory | To inform data analysis | Pathology testing for vitamin B12 and folate [ ] |
| Resource allocation theory | To refine arguments in funding debate | Assisted Reproductive Technologies [ ] |
| Prioritisation and quality improvement theories | To develop a proposal for rationalisation, prioritisation and rationing | Assisted Reproductive Technologies [ ] |
Perhaps the most relevant to disinvestment is the theory of discontinuance, defined by Rogers in his discussion of the theory of diffusion as “a decision to reject an innovation after having previously adopted it” [ 19 ]. In their review of diffusion of innovations in health care, Greenhalgh et al. note the importance of research into discontinuance and the lack of studies in this area [ 20 ]. Hollingworth et al. propose a schema of health technology adoption and withdrawal which includes both discontinuance and disinvestment [ 21 ] and Niven et al. use the definition of discontinuance for the term ‘de-adoption’ in their review of low-value clinical practices [ 22 ].
Frameworks use concepts and relationships to provide a frame of reference, organise and focus thinking and assist interpretation. Frameworks are descriptive, tend to be high-level and can apply to a wide variety of situations [ 12 , 23 ]. No frameworks for systematic, integrated, organisation-wide approaches to disinvestment were identified, however there are several frameworks for specific aspects of the disinvestment process. These are summarised by setting, aims, method of development and components in Table Table3. 3 . Those applicable to the local healthcare setting are discussed in more detail under the relevant steps in the disinvestment process below.
Examples of frameworks and models related to disinvestment
| Framework/Model | Setting | Aims | Method of development | Components |
|---|---|---|---|---|
| PROJECTS TO IDENTIFY AND DISINVEST INDIVIDUAL TCPS | ||||
| Framework of potential settings and methods for disinvestment [ ] | Organisation-wide program in local health service network | To identify potential settings and methods for disinvestment decision-making within local health service systems and processes | Literature review; survey of external experts, interviews and workshops with local stakeholders | Three organisational contexts that provide potential opportunities to introduce disinvestment decisions into health service systems and processes are presented in order of complexity, time to achieve outcomes and resources required: 1. Explicit consideration of potential disinvestment in routine decision-making for purchasing and procurement and development of guidelines and protocols, 2. Proactive decision-making about disinvestment driven by available evidence from published research and local data, 3. Specific exercises in priority setting and system redesign. |
| Algorithm for selecting a disinvestment project from a catalogue of potential opportunities [ ] | Organisation-wide program in local health service network | To facilitate decision-making for identification of potential and selection of actual disinvestment projects | Literature reviews; surveys, interviews and workshops with local stakeholders; document analysis; consultation with experts; taxonomy development | Five steps in selection process: 1. Assess highest risk, 2. Assess importance and potential, 3. Assess quality and strength of evidence, 4. Assess extent of problem, 5. Assess implications of change. Three key decision-making steps between Steps 2 and 3, 3 and 4, and after 5. After selection: Notify decision; Implement; Evaluate; Report Each step includes the activities, who will undertake them, and the decision options |
| Model for an Evidence Dissemination Service [ ] | Organisation-wide program in local health service network | To facilitate use of recently published synthesised evidence in organisational decision-making | Literature reviews; surveys, interviews and workshops with local stakeholders; document analysis; consultation with experts; taxonomy development | Methods and tools to identify sources of high quality synthesised evidence; automate methods of capture; classify, collate and store materials in useful categories; prioritise based on user and health service needs; repackage into suitable formats based on user needs; identify relevant individuals or groups to receive information; disseminate to the appropriate target groups, and report use of evidence |
| Guideline for Not Funding Health Technologies (GuNFT) [ ] | Two versions are provided, one for application at national and regional level and the other at local level. | To facilitate establishment of a transparent, systematic and explicit process for assessing the potential for disinvestment in certain health technologies or in some of their indications | Literature review; face-to-face meeting, teleconference and emails using Nominal Group Technique with 10 experts representing health care delivery, administration, technology assessment and consumers to draft the guideline; validation by two external experts in HTA; wide circulation for comment and approval | Seven phases: 1. Identification through applications; 2. Validation of applications; 3. Prioritisation (if necessary); 4. Assessment; 5. Decision making; 6. Development of an action plan; 7. Diffusion of the decision, the reasons why it has been taken and the action plan. Applications are submitted by health care professionals; validation, prioritisation and assessment of the applications are undertaken by a HTA agency or the health service Technology Assessment Committee; and the decision, development of the action plan and diffusion is undertaken by the health service or regional health authority management team or other multidisciplinary body. Tools are available. |
| Disinvestment framework to guide resource allocation decisions in health service delivery [ ] | Health service delivery organisations | To aid disinvestment activity in the local setting. | Thematic analysis of systematic review and a scoping review of the public sector and business literatures. Draft framework critiqued by Decision Maker Advisory Committee (Chief Financial Officers from Canadian health services) and External Reference Group (international academics) before being finalised. | Seven steps: 1. Determine objectives and scope; 2. Identify strategic priorities; 3. Identify options and risk; 4. Rank options; 5. Develop implementation plan; 6. Conduct disinvestment; 7. Assess outcomes and processes. Oversight Committee (senior managers and clinical leaders) is responsible for the majority of the process components including making final decisions; independent Assessment Committee (managers, clinicians, other staff and public representatives) defines the criteria, weights and scale used to assess disinvestment options, Support Committee (researchers and financial personnel) assists in the assessment of disinvestment options in the form of evidence, financial analysis and evaluative measures. |
| PROGRAMS FOR SECTOR-WIDE INVESTMENT AND DISINVESTMENT | ||||
| Framework of components in the resource allocation process [ ] | Organisation-wide program in local health service network | To represent components in the process of resource allocation and the relationships between them | Interviews and workshops with stakeholders, thematic analysis of responses, document analysis, use of existing frameworks to synthesise findings | Eight components: Governance, Administration, Stakeholder engagement, Resources Decision Making, Implementation, Evaluation, and, when appropriate, Reinvestment. Details of elements of structure and practice within each component is provided. Structure is described as ‘who’ and ‘what’ and includes people, systems, policies, requirements, relationships and coordination. Practice addresses ‘how’ through processes, procedures, rules, methods, criteria and customs. |
| Model for Sustainability in Health care by Allocating Resources Effectively (SHARE) [ ] | Organisation-wide program in local health service network | To develop, implement and evaluate organisation-wide systematic, transparent, accountable and evidence-based decision-making systems and processes | Three literature reviews; online survey, interviews and structured workshops with stakeholders; consultation with experts in disinvestment, health economics and health program evaluation; drafted in consultation with staff, consumers and external experts; assessed against framework for success and sustainability | Four components, each with multiple elements: 1. Systems and processes; 2. Disinvestment projects; 3. Support services; 4. Program evaluation and research. The model outlines each component and the relationships between them, their aims and activities as well as the underlying principles and the preconditions required for success and sustainability. There is also detailed discussion of the antecedents, barriers and enablers. |
| New Zealand National Health Committee Workplan [ ] | National government decision-making | To provide the Minister of Health with recommendations for use and funding of health technologies | Not documented | The program addresses which technologies should be publicly funded, to what level and where technology should be provided and how new technology should be introduced and old technology removed. Six phases: 1. Identification, 2. Prioritisation, 3. Analyse and Assess, 4. Recommend, 5. Implement, 6. Evaluate. |
| Health technology reassessment and decommissioning framework/model [ ] | National or provincial government decision-making | To create a model for assessing the health technology life cycle to identify and delist obsolete technologies | Focused narrative literature review and input from experts. | Two components: 1. Health technology life cycle and reassessment, 2. Reassessment and Decommissioning Model, with Oversight Committee, Triggers, and Possible Outcomes. Second component includes triggers and processes, structure (oversight committee), decisions and outcomes |
| PROGRAM EVALUATION | ||||
| Framework for evaluation of priority setting [ ] | National, regional and individual healthcare facilities | To develop a framework for the evaluation of priority setting practice at macro and meso levels | Literature review and thematic analysis | Two evaluation domains: 1. Consequentialist outcomes: Efficiency, Equity, Stakeholder satisfaction, Stakeholder understanding, Shifted (reallocation of resources), Implementation of decisions, 2. Proceduralist conditions: Stakeholder engagement, Empowerment, Transparency, Revisions, Use of evidence, Enforcement, Community values |
| SHARE Program Evaluation Framework and Plan [ ] | Organisation-wide program in local health service network | To assess the effectiveness of the SHARE program, implementation fidelity and factors for successful change | Drafts prepared by project team in consultation with Consultant in Health Program Evaluation to meet the information needs of key stakeholders and the internal capacity of staff conducting the project; revised and finalised in consultation with key stakeholders | Seven evaluation domains: 1. Improved patient care, 2. Improved resource allocation for health technologies and clinical practices, 3. Improved decision-making, 4. Improved staff capacity in use of evidence and data in decision-making and implementation of practice change, 5. Barriers and enablers, 6. Implementation fidelity, 7. Sustainability and spread. Includes an outcomes hierarchy based on the SHARE program components and a research program based on a theoretical framework for implementation of an evidence-based innovation. |
| Framework for evaluation and explication of the processes and outcomes of a disinvestment project [ ] | Organisation-wide program in local health service network | To adapt a framework and taxonomy for evaluation of evidence-based innovations to enable evaluation and explication of disinvestment projects | Literature review, surveys and interviews with stakeholders | Three components: 1. Determinants of effectiveness (characteristics of external environment, organisation, proposal for change, rationale and motivation, potential adopters, potential patients, identification process, prioritisation and decision-making process, implementation plan, implementation resources); 2. Process of change (delivery of implementation strategy and stages of change); 3. Outcomes (process and impact for patient, practitioner, systems, economic, reinvestment, sustainability and spread). Taxonomy containing details within each component is provided. |
| Integrative framework for measuring overuse [ ] | Relevant settings within health care systems | To assess the impact of efforts to reduce low-value care. | Not documented | Provides list of measurement tools linked to specific project/program goals and discusses advantages and disadvantages of each approach |
| STAKEHOLDER ENGAGEMENT | ||||
| SHARE model for incorporating consumer views into decisions for resource allocation [ ] | Organisation-wide program in local health service network | To involve consumers in organisation-wide decision-making, capture their perspectives and incorporate them into decisions for resource allocation. | Literature review, individual and group interviews with Consumer Working Group and health service staff, workshop with Community Advisory Committee, drafting and revision with consumer participation. | Four components: 1. Principles, 2. Scope, 3. Preconditions, 4. Activities Activities include Consumer engagement (communication, consultation and participation) and use of Consumer evidence (consumer perspectives found in publications and data sources). Details of activities are reported in the context of the components of the resource allocation process noted above |
| New Zealand National Health Committee Workplan [ ] | National government decision-making | To seek advice and engage with the health sector | Not documented | Tiered approach to engage with and seek advice from clinicians via colleges and specialty societies; providers such as District Health Boards, NGOs and private facilities via Health Sector Forum; international Health Technology Assessment agencies; Universities and Research Institutes, international and domestic manufacturers. |
Polisena and colleagues [ 24 ] identified three frameworks in their review of disinvestment projects: Health Technology Assessment (HTA) [ 25 ], Accountability for Reasonableness (A4R) [ 26 ] and Program Budgeting and Marginal Analysis (PBMA) [ 27 ]. To distinguish between evaluation of new TCPs and those in current practice, the term Health Technology Reassessment (HTR) has been introduced for methods aiming to identify potential targets for disinvestment [ 28 , 29 ]. HTA and A4R are frameworks by definition and are valuable tools for decision-making; however, although their use may lead to disinvestment, they are not frameworks specifically for disinvestment. Like A4R and HTA, PBMA and other priority setting frameworks [ 30 – 32 ] can play a key role in certain approaches to disinvestment, but do not address all potential aspects of the disinvestment process or all opportunities to drive change. However they would all integrate readily into a wider framework for disinvestment, as aspired to with the trialing of the Australian Medicare Benefits Schedule Review initiative [ 33 ]. Recently Elshaug et al. provided a comprehensive inventory of disinvestment policy and practice levers that could flow from HTA/HTR and other priority setting processes [ 34 ].
Sources of synthesised evidence such as HTAs, systematic reviews and evidence-based guidelines, can underpin disinvestment decisions in two ways. Firstly, the process of evidence synthesis can be undertaken reactively to address policy, management or clinical questions as they arise and inform the resultant decisions. Secondly, dissemination of the findings of published HTAs, systematic reviews or guidelines can be a proactive method of initiating decision-making to ensure policy and practice is consistent with the best available evidence.
The ‘Disinvestment framework to guide resource allocation decisions in health service delivery’ [ 16 ] and the ‘Guideline for Not Funding Health Technologies’ (GuNFT) [ 35 ] are examples of frameworks to identify and disinvest individual TCPs. They are very similar to the process outlined in the Workflow Diagram of the New Zealand National Health Committee for introduction of new and removal of old technologies [ 36 ]. All three are systematic, transparent and based on a series of steps to identify suitable TCPs, engage relevant stakeholders, make the appropriate decisions, implement and evaluate change.
The New Zealand National Health Committee also includes a framework for wider stakeholder engagement in their Business Plan [ 36 ].
Joshi and colleagues use both framework and model when referring to the outcome of their narrative review ‘Reassessment of Health Technologies: Obsolescence and Waste’ [ 37 ]. Based on the definitions used herein, it is classified as a framework. It includes the role of reassessment in the life cycle of a health technology and triggers, structures and outcomes for health technology reassessment and decommissioning.
Bhatia et al. present an ‘Integrative framework for measuring overuse’ as an evaluation tool to be implemented within initiatives that aim to reduce ‘low value care’ [ 38 ] and Barasa and colleagues propose a framework for evaluation of priority setting processes which considers both procedure aspects and outcomes in a range of contexts [ 39 ].
Conceptual frameworks developed in the SHARE Program for a range of purposes within the disinvestment process include potential settings and methods to integrate disinvestment into health service systems and processes [ 5 ], components in the resource allocation process [ 6 ], an evaluation framework and plan for the overall SHARE program [ 40 ] and an algorithm to facilitate decision-making for selecting projects from an evidence-based catalogue of potential opportunities for disinvestment [ 9 ]. An existing framework for evaluation and explication of implementation of an evidence-based innovation was adapted for use in disinvestment projects [ 9 ] and health information products and services [ 11 ].
Models are more precise and more prescriptive than frameworks. They are narrower in scope, the concepts are well defined and the relationships between them are specific. Models are representations of the real thing [ 12 , 23 ].
The SHARE Program produced three models: integrating consumer values and preferences into decision-making for resource allocation in a local healthcare setting [ 7 ], exploring Sustainability in Health care by Allocating Resources Effectively in this context [ 8 ] and facilitating use of recently published synthesised evidence in organisational decision-making through an Evidence Dissemination Service [ 11 ]. These are summarised in Table Table3. 3 . No other models for disinvestment were identified in the literature.
New Framework
Information pertaining to the practical and operational aspects of disinvestment in the local healthcare setting is presented and discussed in the context of a new framework (Fig. (Fig.2). 2 ). The framework proposes a systematic approach that is integrated within organisational infrastructure. It brings together the definitions, concepts, principles, decision-making settings, potential prompts and triggers to consider disinvestment, and steps in the disinvestment process identified from the literature. It also seeks to remove barriers when it is possible to do so through establishment of new or adjustment of existing operational mechanisms. The details of each of the framework components are clearly articulated in the literature; many are derived from extensive work with stakeholder groups including decision-makers, policy-makers, health service staff, patients and members of the public.

Framework for an organisation-wide approach to disinvestment in the local healthcare setting
The proposed framework builds on the work of others. While incorporating all the messages from the literature, it draws heavily on the three noted frameworks which identify steps in the disinvestment process [ 16 , 35 , 36 ]; the SHARE frameworks and models [ 5 – 9 ]; and other frameworks for introduction of new TCPs [ 2 ] and evidence-based change [ 41 ].
The framework is aimed at health service decision-makers considering disinvestment and resource allocation, and health service researchers and implementation scientists working in this context.
The setting for this initiative was Monash Health, a large health service network in Melbourne Australia operating within a state-allocated fixed-budget model of financing. We anticipate results of this work and elements of the framework to have broader applicability and transferability, including to fee-for-service environments.
Application
Decision-making in healthcare is described at three levels: macro (national, state/provincial and regional), meso (institutional) and micro (individuals) [ 42 , 43 ].
The proposed framework was developed for use in policy, management and/or clinical decision-making at the meso level. It was designed to be embedded within existing systems and processes where it can be responsive to local needs and priorities at the level of implementation; for example health service networks, individual facilities, departments, wards or committees.
Definitions
The lack of standardised terminology is a barrier to development of systematic approaches to operationalise disinvestment [ 1 ]. To address this, definitions and key concepts underpinning the framework are made explicit. The proposed framework provides a common language for researchers and decision-makers within and between programs, institutions and health systems making it easier to build and share a body of knowledge.
There are multiple definitions for disinvestment in the literature based on a range of different concepts [ 1 , 44 ]. Numerous alternative terms conveying the same concepts are also in common use. Disinvestment is focused on the use of ‘health technologies’ but there is also a range of definitions for this term. To compound the difficulties arising from multiple definitions, the terms ‘disinvestment’ and ‘health technologies’ are frequently used in one way by researchers and in another by health service decision-makers [ 1 ]. Definitions relevant to the local healthcare setting are provided in Table Table4 4 .
| Health technologies | Health products, devices and equipment used to deliver health care (eg prostheses, implantable devices, vaccines, pharmaceuticals, surgical instruments, telehealth, interactive IT and diagnostic tools). This is a narrow definition which reflects the common use by decision-makers and consumers in the local health care setting. Clinical practices, support systems, or organisational and managerial systems are NOT considered to be health technologies in this context. |
| Health technologies and clinical practices (TCPs) | Therapeutic, preventative and diagnostic procedures (eg use of products, devices and equipment PLUS medical, surgical, nursing, allied health and population health interventions). This is a pragmatic term to reflect the scope of most resource allocation decisions in the local healthcare setting. |
| Health programs and services | Agencies, facilities, institutions and the components within them that deliver health care, rehabilitation or population health practices such as health promotion and education. |
| Disinvestment | Removal, reduction or restriction of any aspect of the health system for any reason. Removal indicates complete cessation, reduction is a decrease in current volume or delivery sites, and restriction is narrowing of current indications or eligible populations. This is a broad definition, in essence the conceptual opposite of investment. This could apply equally to products, devices and equipment; clinical practices and procedures; health services and programs; information technology and corporate systems. |
| Principles | Fundamental qualities or elements that represent what is desirable or essential in a system. |
| Criteria | Standards against which alternatives can be judged in decision-making. |
| Routine decisions | Decisions made on a recurring basis or scheduled via a timetable eg annual budget setting processes, six-monthly practice audits, monthly Therapeutics Committee meetings, reviews of protocols at specified intervals after their introduction, etc. |
| Reactive decisions | Decisions made in response to situations as they arise eg new legislation, product alerts and recalls, applications for new drugs to be included in the formulary, critical incidents, emerging problems, etc. |
| Proactive decisions | Decisions driven by information that was actively sought for the purpose of healthcare improvement eg accessing newly published synthesised research evidence such as Cochrane reviews or Health Technology Assessments to compare against current practice, interrogating routinely-collected datasets to ascertain practices with high costs or high rates of adverse events, etc. |
| Prompt | An informal reminder or encouragement for thought or action. |
| Trigger | A formal mechanism that initiates or activates a reaction, process or chain of events. |
| Diffusion | Passive processes by which an innovation is communicated over time among members of a social system; usually unplanned, informal, untargeted, uncontrolled, decentralised, and largely horizontal or mediated by peers. |
| Dissemination | Active processes to spread knowledge or research eg publications, presentations and other deliberate strategies; planned, formal, often targeted, controlled or centralised, and likely to occur more through vertical hierarchies. |
| Maintenance | Active processes to sustain recently implemented change after project support is removed; to integrate the change into organisational systems, processes and practices; and to attain long-term viability of the change. |
| Methods and tools | Approaches, instruments or other resources that identify ‘what’ tasks are needed at each step and/or ‘how’ to undertake them. This is a pragmatic inclusive definition developed for use in this review to assist health service staff in disinvestment. This broad definition allows frameworks and models to be included if they meet these criteria. |
We use the term disinvestment in the broadest sense, ‘removal, reduction or restriction of any aspect of the health system for any reason’. This can be applied to products, devices and equipment; clinical practices and procedures; health services and programs; information technology and corporate systems. Unlike most of the research definitions for disinvestment, this version is not constrained by a specified purpose (eg withdrawing practices of low value), defined criteria (eg effectiveness or cost-effectiveness) or anticipated outcome (eg reallocation of resources) which do not address cessation or limitation of TCPs for other purposes, based on other criteria, for different outcomes, which are likely to arise in local health services [ 1 ].
In contrast, we define health technologies in the narrowest sense; as products, devices and equipment used to deliver health care (eg prostheses, implantable devices, vaccines, pharmaceuticals, surgical instruments, telehealth, interactive IT and diagnostic tools) which reflects common use by health service decision-makers and consumers [ 1 ]. Clinical practices, health programs and services, information technologies, support systems, and organisational and managerial systems are not included in this definition. Although contained in many research definitions, they are not included in general references to health technologies in the local healthcare setting [ 1 ].
The terms ‘principles’ and ‘criteria’ are often used interchangeably; definitions for use in this review are included in Table Table4 4 .
The proposed framework is underpinned by several key concepts (Table (Table5). 5 ). While disinvestment is the aim, it is not considered in isolation but in the context of resource allocation, addressing the spectrum of decision-making covering investment in new, continuation of existing, and disinvestment from current activities. The focus of the framework is positive: optimising healthcare, improving health outcomes, using resources effectively and efficiently. The components of the framework are integrated within current systems and processes and within existing health improvement paradigms such as evidence-based practice (EBP), quality improvement (QI) and system redesign.
| Concept | Implication for framework |
|---|---|
| Use of the term disinvestment as a driver or justification for change is associated with negative connotations such as focusing on cost cutting, engendering suspicion and distrust, and getting stakeholders offside. | Do not use ‘disinvestment’ as the basis for the framework or the aim of change initiatives |
| Conducting disinvestment activities independently of existing systems and processes does not represent the reality of health service decision-making. It may be counterproductive: lacking incentives for change and introducing disincentives. Disinvestment should not be considered as an isolated activity, but integrated within existing systems and processes in the context of all resource allocation decisions, covering the spectrum from investment to disinvestment. | Implement disinvestment activities in the context of ‘resource allocation’ |
| Removal or restriction of practices that are harmful or of little or no value; replacement of inferior practices with more effective or cost-effective alternatives; and reduction of organisational waste, systematic error and inappropriate use of TCPs all arise from good policy, management and clinical decisions. If these are based on evidence from research, local data and/or stakeholder views there are sound positive drivers for action. There is no need for the concept of disinvestment to be introduced as a reason for change. | Focus on the positive reasons driving removal, reduction or restriction of current practices Use existing systems, processes, expertise, methods and tools whenever possible |
| It has been proposed that disinvestment activities are more likely to be successful if decisions are transparent, integrated into everyday decision-making and central to local planning rather than ad hoc decisions, individuals ‘championing’ causes or standalone projects | |
| Disinvestment driven from a positive perspective focusing on optimisation of health care through allocation or reallocation of finite resources for maximum effectiveness and efficiency is more likely to be successful. | |
| Existing healthcare improvement paradigms such as Knowledge Translation, Evidence Based Practice, Quality Improvement, System Redesign and Health Economics offer theories, frameworks, methods and tools for decision-making, implementation and evaluation that can be applied to disinvestment. |
Level of detail
Many of the elements within the proposed framework should be self-evident and be applied routinely as good practice, making it unnecessary to stipulate their requirement. However strong and consistent messages in the literature confirm that they are not standard practice and authors felt the need to state that they should be made explicit. Incorporating them all into a detailed framework achieves this.
Another reason for including all the elements in detail is to address potential ethical dilemmas [ 1 ]. In some circumstances it may be difficult to accommodate the principles of beneficence and utilitarian justice; clinicians advocate for the best interests of individual patients but resource allocation aims for the greatest benefit for the most people [ 45 – 47 ]. Similarly, arguments for equity may conflict with those for efficiency when the most efficient outcome is not the most equitable [ 48 – 50 ]. A systematic, transparent approach acknowledging these issues may facilitate difficult discussions and create potential for some efficiency to be traded away for equity maintenance or gain.
Some elements may be more important than others in individual situations. However, because they are all defined in the framework, the decision to exclude or reduce the role of some elements in extenuating circumstances becomes explicit. This strengthens the process and empowers those who have previously participated in suboptimal decision-making due to lack of resources, hidden agendas or organisational politics [ 6 , 51 – 57 ].
The proposed framework is composed of three interconnected and interdependent components: 1) a program for organisation-wide decision-making, 2) projects to implement decisions and evaluate outcomes, and 3) research to understand and improve the program and project activities. Each component has a number of elements which are outlined in detail below.
Characteristics
The framework is primarily descriptive to enable application in a local healthcare service and allow adaptation, replication and testing. It was developed using both deductive and inductive methods. Although not based on a specific theory, it has potential to facilitate future theory development and/or testing. Specific characteristics of the framework and potential for its use are summarised in Table Table6 6 using domains and criteria developed to assess the robustness and utility of proposed models and frameworks [ 12 ]. This assessment enables potential users to identify whether the framework will meet their aims and be applicable to their situation.
Characteristics of a framework for organisation-wide approach to disinvestment in the local setting
| Domain | SHARE features |
|---|---|
| Purpose ▪ descriptive, explanatory or predictive | The framework is primarily descriptive to enable application and allow replication and testing. There are also some explanatory elements addressed in the relationships between components, for example ethical principles underpin all activities, decision-making settings sit within the scaffold of all eight principles, projects follow on from decisions, research is conducted in all aspects. |
| Development ▪ deductive or inductive ▪ supporting evidence | Methods used in development were both deductive and inductive. Evidence from research literature and other publications was the primary source. Many of these findings were based on extensive work with stakeholder groups. This was supplemented with experience from the SHARE program. |
| Theoretical underpinning ▪ explicit or implicit | No specific theory was used to underpin the framework. |
| Conceptual clarity ▪ well-described, coherent language for identification of elements ▪ strengths and weaknesses of theories ▪ potential to stimulate new theoretical developments | Three components are outlined in the framework: Program, Projects and Research. The Program is based on eight principles and nine settings for decision-making. The Projects are outlined in eight main steps. The relationships between them are captured in a diagram. Details of each component and the elements within them are provided in the text and in tables. No specific theories were used so no comparisons are made. There is potential for new theoretical developments if: ▪ specific theories are tested in development and implementation of the components ▪ components are removed or the relationships changed ▪ principles or pre-conditions are varied ▪ the framework is applied for purposes other than resource allocation ▪ the framework is applied in a range of contexts |
| Level ▪ individual, team, unit, organisation, policy | The framework was developed for implementation at meso level within the health system eg local network, institution, department, ward or committee. |
| Situation ▪ hypothetical, real | The framework represents actual settings and contexts in health service decision-making and implementation of change. However it could also be used for teaching or capacity building through hypothetical classroom discussions or simulation exercises. |
| Users ▪ nursing, medical, allied health, policy makers, multidisciplinary | The framework can be used by any decision-makers within the health system. While use of the framework could be initiated by any group, engagement and involvement of all relevant stakeholders is an underlying principle of application. The framework could be used in policy, management or clinical contexts. |
| Function ▪ barrier analysis ▪ intervention development ▪ selection of outcome measures ▪ process evaluation | The main function is to establish and maintain systems and processes to make, implement and evaluate decisions regarding resource allocation and research the components involved. The principle of evidence-based implementation requires assessment of barriers and enablers but the framework itself does not specifically facilitate this process other than to prompt users. Details of barriers identified from the literature are contained in the text and tables. The steps within the Project component will facilitate development of an intervention for systematic evidence-based decision-making and implementation of change. Evaluation of process and outcomes is a key element; however selection of variables and outcome measures is not facilitated by the framework per se, other than to prompt users to take an evidence-based approach. Examples of measures proposed by others are included in the text. |
| Testable ▪ hypothesis generation ▪ supported by empirical data ▪ suitable for different methodologies | The framework describes principles to underpin robust decision-making, settings and opportunities, implementation of change and evaluation of process and outcomes. A range of hypotheses could be developed for each of these elements and the relationships between them which could be tested in a number of ways using various methodologies. The framework could also be tested beyond the local healthcare level, at national or state/provincial level; or outside the health context in education, community development, social services, etc |
Principles for decision-making
Forty-two principles were identified from the existing literature and the SHARE publications and grouped into eight categories that emerged from these findings: Boundaries, Ethics, Governance, Structures, Processes, Stakeholder involvement, Resources and Preconditions. These are presented in the framework as two groups (Fig. (Fig.2 2 ).
The first group have a hierarchical relationship depicted as a series of nested boxes. The whole program is defined by explicit boundaries, ethical principles underpin good governance, governance directs and controls structure, and structure enables and accommodates process. The decision-making settings, prompts and triggers all sit within the scaffold of these five categories.
The second group, represented as three vertical bars, are required across all of the other elements. For example, stakeholders need to be involved in defining the boundaries and establishing the ethical parameters and methods of governance; they should be included in the structures and processes and participate in the projects and research. Adequate and appropriate resources and the noted preconditions will be required to establish, maintain and improve all aspects of the framework.
The intersection of the two groups of principles also demonstrates that ethics, governance, structures and processes also apply to stakeholder engagement, resources and preconditions. For example, stakeholder engagement should be systematic and integrated, funding should be sourced ethically and influence should be transparent.
These principles and their relationships also apply to the project and research components.
Further details of the categories, full descriptions of individual principles, and related citations are outlined in Additional file 1 .
Nine settings for decision-making are described in three categories: Decision-making infrastructure, Specific initiatives and Individual decision-makers.
While the framework is proposed for organisation-wide application, any of the nine settings could be considered individually. A framework for a single setting would be underpinned by the same principles, decisions would lead to projects with the same steps and research could be conducted on all elements.
Decision-making infrastructure
Each sector of the health system has an organisational infrastructure of decision-making settings where committees, designated panels or individuals with delegated authority make decisions on behalf of the jurisdiction or individual facility. A classification system and descriptors for decision-making settings, decision-makers, scope and type of decisions in the local health service setting was developed in the SHARE Program [ 6 ].
Decisions can be categorised as routine, reactive and proactive [ 6 , 58 ]. Routine decisions are made on a regular basis; reactive decisions are made in response to situations as they arise; and proactive decisions are driven by information that was actively sought for the purpose of healthcare improvement. Examples are included in Table Table4 4 .
A range of potential decision-making activities are outlined in Table Table7 7 [ 1 , 5 , 6 , 8 , 59 – 61 ]. Most of these occur in more than one of the three categories of decision-making and can be used for more than one aspect of the disinvestment process. Development or revision of guidance documents is a good example. Guideline and protocol development can occur routinely, particularly when existing documents are updated at regular intervals; in reactive situations such as a critical incident which highlights lack of guidance in a specific area; or when proactive use of research identifies that current documents do not reflect the best available evidence. Disinvestment opportunities can be identified if the systematic review process undertaken when initiating or revising a guidance document determines that a TCP, service or program should be removed or replaced [ 5 , 17 , 60 – 63 ]. Guidance documents can also be used to implement disinvestment decisions and audit of guideline adherence can measure the results [ 59 , 60 , 64 – 66 ]. Manuals for guideline or protocol production could include prompts to note and follow up opportunities for disinvestment as part of the document development process [ 5 ].
Examples of activities and settings for disinvestment within decision-making infrastructure
| Activity | Example | Routine | Reactive | Proactive | Priority Setting |
|---|---|---|---|---|---|
| Meeting external requirements | ▪ Addressing legislative, regulatory and accreditation requirements, national and professional standards, etc | ✓ | ✓ | ||
| ▪ Responding to product alerts and recalls | ✓ | ||||
| Setting budgets | ▪ Determining sources of income and items of expenditure | ✓ | ✓ | ||
| Spending money | ▪ Introducing new items to funding lists. Examples include, but are not limited to, national health schemes, insurance benefits schedules, institutional lists of permitted TCPs, formularies. | ✓ | ✓ | ✓ | ✓ |
| ▪ Commissioning health services and programs | ✓ | ✓ | ✓ | ✓ | |
| ▪ Procuring capital works, plant and equipment | ✓ | ✓ | ✓ | ✓ | |
| ▪ Purchasing clinical consumables | ✓ | ✓ | ✓ | ✓ | |
| ▪ Assessing grant and funding applications | ✓ | ✓ | |||
| Allocating non-monetary resources | ▪ Allocating people, time, access to facilities, etc | ✓ | ✓ | ✓ | ✓ |
| ▪ Developing guidance documents, promotional information or educational materials that indirectly allocate resources. Examples include, but are not limited to, peak body recommendations, clinical guidelines, protocols, standard operating procedures, decision support systems, posters, presentations. | ✓ | ✓ | ✓ | ✓ | |
| Making strategic and operational decisions | ▪ Developing goals and strategies for Strategic Plans | ✓ | ✓ | ||
| ▪ Developing outcomes measures and targets for Business Plans | ✓ | ✓ | |||
| Using evidence to initiate and/or inform decisions | ▪ Updating existing evidence, undertaking Health Technology Reassessment, etc. | ✓ | ✓ | ✓ | |
| ▪ Accessing and utilising research evidence, population health data, local health service data, consumer and staff feedback | ✓ | ✓ | ✓ | ✓ | |
| Evaluating outcomes of previous decisions and projects | ▪ Monitoring, evaluating and reporting of all newly introduced TCPs to see if they perform as expected, post marketing surveillance | ✓ | |||
| ▪ Monitoring, evaluating and reporting of purposive or random samples of decisions | ✓ | ✓ | ✓ | ||
| ▪ Monitoring, evaluating and reporting of purposive or random samples of projects | ✓ | ✓ | ✓ |
Formal priority setting exercises may also be built into the decision-making infrastructure. These determine which TCPs, programs or services to introduce, maintain or remove based on a pre-determined set of criteria. An example might be annual capital expenditure decisions. In this situation, priority setting could be classified as ‘routine’, however it is noted separately in the framework as it also commonly arises in the context of individual initiatives described below.
Specific initiatives
In addition to the decision-making settings outlined, specific initiatives to improve practice are undertaken by health services, many of which involve disinvestment. These may be instigated by government, management or health practitioners, and although there is considerable diversity, most are related to EBP, QI, system redesign or economic approaches to priority setting such as PBMA [ 1 , 6 , 34 ]. Some projects may set out to disinvest, others may have quite different initial aims but the need for disinvestment becomes apparent during the project.
An EBP approach might be to remove or reduce use of inferior practices identified from systematic reviews, HTAs, evidence-based guidelines or ‘low value’ lists, or reduce their use to levels deemed clinically appropriate [ 9 ]. Clinical audit, QI and system redesign methods may be used to tackle inappropriate use of TCPs or organisational waste. Priority setting exercises like PBMA consider the costs and benefits of relevant alternatives in an aspect of healthcare delivery to determine the maximum outcome from the available resources.
There are several examples of disinvestment-related initiatives with relevance at the local health service level. Therapeutic equivalence or drug substitution programs involving replacement of expensive drugs with equally effective but lower cost alternatives from the same drug family has demonstrated considerable cost saving in macro and meso programs [ 67 , 68 ]. Generic prescribing, substituting brand name drugs with generic alternatives, has been addressed at international, national, institutional and individual levels with mixed outcomes [ 69 – 72 ]. Benchmarking the results from individual interventions or programs across different health providers aims to ascertain best practice which others can aspire to and which can be applied at all levels; but by simultaneously identifying inferior practices it can also be used as “ a tool to start a disinvestment dialogue ” [ 21 , 73 , 74 ].
Individual decision-makers
At the micro level, the term ‘disinvestment’ is not generally applied to changes initiated by individuals; however the principle is the same. Individuals cease or restrict practices when they become aware of new evidence or to address local needs and priorities.
Much of the literature on decision-making focuses on how money is spent, however there are considerable opportunities for disinvestment in allocation of non-monetary resources. Although clinical encounters do not usually involve funding decisions, they offer opportunities to consider disinvestment in use of other resources such as ordering tests, referring to other practitioners, using drugs and other therapies, or undertaking procedures. An example is the Choosing Wisely program being replicated in national campaigns across the world which highlights potentially ‘low value’ treatments and tests so that clinicians and consumers can consider the relative benefits in their specific situations [ 75 ].
Prompts and triggers
Prompts and triggers are proposed to initiate and facilitate identification of disinvestment opportunities. Prompts are informal reminders or encouragement for thought or action and triggers are formal mechanisms that initiate or activate a reaction, process or chain of events (Table (Table4). 4 ). The settings above provide opportunities to introduce systematic prompts and triggers to use evidence from research, data and stakeholder feedback to drive decision-making.
Prompts, triggers and potentially even mandatory requirements to consider disinvestment could be built into existing decision-making infrastructure [ 5 , 37 ]. Using expenditure decisions as an example, prompts and triggers could be incorporated into meeting agendas of finance committees, budgeting processes, application forms, algorithms, protocols or checklists. Mandatory requirements to consider disinvestment could be implemented as specific directions within purchase orders, explicit decision-making criteria for committees, or steps in application processes that require authorisation. Additional examples of prompts and triggers at the organisational level are outlined in Table Table8 8 .
Examples of systematic prompts and triggers to initiate disinvestment decisions
| ▪ Approve introduction or continuation of TCPs for limited time only and require review of desired outcomes, costs, etc. before re-approval is granted at end of time period |
| ▪ Approve new guidelines and protocols for limited time only and require review of evidence, costs, etc. and appropriate revision before re-approval is granted at end of time period |
| ▪ Include steps that consider disinvestment of existing practices in manuals for guideline and protocol development |
| ▪ Include steps that consider disinvestment of existing practices in checklists for a range of organisational decisions |
| ▪ Add consideration of disinvestment to templates for meeting agendas where appropriate |
| ▪ Mandate consideration of disinvestment in procurement processes: include in requistion documents and require sign off by relevant body overseeing disinvestment at appropriate level |
| ▪ Systematically ascertain evidence from research, data or stakeholder feedback, send directly to decision-makers and seek and/or require response |
| ▪ Incorporate flags and/or question use of low value TCPs in clinical decision support systems |
| ▪ Build questions about potential disinvestment into business case templates and application forms for grants, changes to formulary, introduction of new TCPs, etc. |
| ▪ Introduce requirements for consideration of disinvestment into documents governing scope of decisions such as position descriptions and committee Terms of Reference |
| ▪ Add prompts to consider disinvestment to data reports, scorecards, dashboards, etc. |
| ▪ Add prompts to consider disinvestment in project management templates and training programs for project management, change management, quality improvement processes, etc. |
| ▪ Build disinvestment into strategic planning processes |
| ▪ Build disinvestment KPIs into business plans or performance plans |
| ▪ Consider ‘one for one’ swaps where a new TCP can only be introduced if an old one is removed |
In specific initiatives to implement health service improvements, prompts and triggers to consider disinvestment could be introduced into project management templates or training programs for project management, change management, quality improvement processes, etc.
Prompts, triggers and mandatory requirements could also be used to guide the decisions of individual practitioners in clinical encounters; these could be included in local guidelines and protocols to steer practice away from unsafe, ineffective or inefficient use of TCPs.
Steps in the disinvestment process
The disinvestment process begins when opportunities for disinvestment are identified from the activities in the settings above. Eight steps in the disinvestment process were ascertained from existing frameworks [ 6 , 16 , 35 , 36 ]: Identification of opportunities; Prioritisation (if required) and Decision-making; Development of a proposal; Implementation; Monitoring, Evaluation and Reporting; Reinvestment (if required); Dissemination and Diffusion; and Maintenance. Two additional elements are included: some projects may require development of local criteria for prioritisation and decision-making and projects that aim to reinvest will need to measure the resources released as part of the evaluation process.
The first two steps are part of the decision-making program, the following six are undertaken in projects arising from the decisions.
Once a decision has been made, a project to implement it can be initiated. While individual projects will have specific characteristics and requirements such as aims, objectives, timelines, budgets, deliverables, roles and responsibilities, the principles outlined in the framework apply to all project activities.
Examples of methods and tools for disinvestment are discussed below; however the proposed framework does not stipulate project design or conduct, allowing application of any theories, methods or tools at each step.
Research is required to understand and improve the program and project activities. It is overlaid across all elements in the diagram to represent the potential for research in each aspect of the framework.
Methods and tools
There are many definitions for the terms theory, framework, model, method, tool, strategy and related concepts. Some definitions note specific features that make the terms mutually exclusive, others allow the terms to be used interchangeably, and some overlap. In this review, the label ‘methods and tools’ is used pragmatically to assist health service staff in disinvestment and includes approaches, instruments or other resources that identify ‘what’ tasks are needed at each step and/or ‘how’ to undertake them. This broad definition allows frameworks and models to be included if they meet these criteria.
Appropriate, valid and reliable methods and tools are required for effective decision-making, implementation and evaluation. The resources identified are described briefly but no evaluation was undertaken due to lack of relevant data; some have been piloted and refined, but most have no published reports of their effectiveness or impact. The availability of validated materials is noted where appropriate. Hence users will need to consider the validity and applicability of these resources in their individual contexts.
There are many sources of generic advice for ascertaining and utilising evidence, undertaking and applying health economic analyses, making decisions, implementing change and evaluating outcomes including, but not limited to, The Cochrane Library, Canadian National Coordinating Centre for Methods and Tools, UK National Institute for Health and Care Excellence (NICE), US Institute for Healthcare Improvement, US Centers for Disease Control and Prevention, and US Agency for Healthcare Research and Quality.
There are also many methods and tools from other areas of health research and practice that are relevant to disinvestment which could be employed within this framework; knowledge translation, EBP, QI, system redesign and other improvement methodologies all have well-developed validated processes that are familiar to health service staff [ 1 ]. While there are few published examples of successful initiatives labelled as ‘disinvestment’ within local health services, there are many examples in the EBP and quality and safety literature of disinvestment-type activities where TCPs that are unsafe or ineffective have been discontinued. A review of ‘de-adoption’ summarises 39 such interventions that provide information on several steps in the disinvestment process [ 22 ].
Two publications provide advice in a range of areas relevant to disinvestment. A book on rationing, priority setting and resource allocation in health care discusses multiple generic and specific methods and tools suitable for disinvestment including stakeholder participation, leadership, economic evaluation and several of the steps in the disinvestment process [ 76 ]. A toolkit for decommissioning and disinvestment, defined as withdrawal of funding from the provider organisation, provides high-level guidance on governance and administrative matters for removal of health services, not individual TCPs, and some tools for assessing service performance against UK data [ 77 ].
The GuNFT guideline provides guidance on establishment of a decision-making program and recommendations, templates and other tools for several steps in the disinvestment process [ 78 ]
Several products from the SHARE Program also address a range of principles and steps in the disinvestment process.
- Summaries of issues to consider in development of an organisational program for disinvestment [ 5 ] and implications for disinvestment in the local setting [ 8 ] were compiled.
- An investigation of the resource allocation process in a local health service generated a framework of eight components, the relationships between them, and features of structure and practice for each component [ 6 ]. Structure is described as ‘who’ and ‘what’ and includes people, systems, policies, requirements, relationships and coordination. Practice addresses ‘how’ through processes, procedures, rules, methods, criteria and customs.
- A classification of decision-making settings, decision-makers, and scope and type of decisions was developed and strengths, weaknesses, barriers and enablers to resource allocation in a local health service were ascertained [ 6 ].
- A model for exploring Sustainability in Health care by Allocating Resources Effectively (SHARE) in the local healthcare setting brings together systems and processes for decision-making; identifying and undertaking disinvestment projects; support services to facilitate making, implementing and evaluating decisions; evaluation and research to measure and understand the processes and outcomes of these disinvestment-related activities; and principles and preconditions for success and sustainability [ 8 ].
Methods and tools for the principles are presented in Additional file 1 .
1. Identification of opportunities
Potential disinvestment opportunities can be derived from all of the decision-making settings discussed above, either incidentally or systematically from prompts or triggers embedded in local systems and processes. However, at the health service level, it is more common for disinvestment opportunities to be identified through ad hoc proposals based on individual’s observations or local knowledge than through a systematic evidence-based approach [ 9 , 21 , 79 , 80 ].
The sources of information noted in the literature that could be used in these settings to identify disinvestment opportunities include research, health service data, expert opinion and stakeholder consultation. While any one of these sources could identify a potential target for disinvestment, ideally information from all four would be combined in confirming the appropriateness of the choice [ 5 ]. Evidence from research would be considered in light of local data. For example, if a systematic review or HTA identified a more cost-effective intervention to one in current use, decision-makers could use local data to assess whether the burden of disease, volume of use, likely impact and potential cost of change warrant the required disinvestment activities. Similarly, evidence from local data would be enhanced by using the literature to identify best practice. For example, if an audit of prescribing rates of a high cost drug finds variation between departments, a review of the appropriate research would confirm whether the higher rate is overuse and should be reduced or the lower rate is underuse and should be increased. Expert opinion and stakeholder consultation add clarification and important perspectives to these decisions and may also reveal examples of inappropriate use of TCPs not identified by other methods. The SHARE Program used the SEAchange model [ 41 ], a formal evidence-based approach to change, to ensure that evidence from research and local data, experience and expertise of health service staff, and values and perspectives of consumers were considered at each step (Fig. (Fig.1) 1 ) [ 3 ].
1.1 Research
Reactive decisions can be informed by synthesised evidence and relevant primary studies; the type of research design and level of evidence required depends on the context of the decision and the nature of the question being addressed. Rigorous evaluation of new TCPs prior to inclusion in nationally funded health schemes has been standard practice for the past two decades and high quality HTAs, systematic reviews, evidence based guidelines and clinical effectiveness research reports have been developed to determine other national health policies. There is also a long history of locally-developed HTAs for use in decisions about introduction of new TCPs at health service level [ 2 , 81 ]. Health technology reassessment of existing TCPs with view to identifying potential targets for disinvestment has been undertaken at both national and local level [ 28 , 29 , 82 , 83 ].
Systematic use of research in routine decisions is evident in reassessment of new TCPs at specified time periods after their introduction at national [ 72 , 84 ] and local level [ 2 ]. At the other end of the TCP lifespan, “obsolescence forecasting” has also been proposed as a systematic approach to initiate HTR when it is anticipated that “a new, more functional product or technology supersedes the old or when the cost of maintenance or repair of old technology outpaces the benefits of a new piece of technology” [ 37 ].
Examples of proactive use of research for disinvestment at national level include a review of all listed drugs conducted in France resulting in removal of 525 drugs considered to have “insufficient medical value” [ 72 ] and commissioning of a complete review of the Australian Medicare Benefits Schedule (fee-for-service) to ensure that all funded items are safe, effective and cost-effective [ 33 ]. There are other examples of systematic and ad hoc use of research to drive disinvestment at national level [ 60 , 72 , 85 ].
Similar approaches have been used at local level where organisations have reassessed all of the TCPs related to a specific clinical issue or area, or reassessed one particular TCP at a time [ 83 ]. The SHARE Program implemented an Evidence Dissemination Service to proactively retrieve, appraise, summarise and categorise synthesised evidence from high-quality sources soon after publication and deliver it directly to the relevant designated groups and individuals responsible for organisational decision-making related to resource allocation [ 11 ]. The SHARE Program also proposed a framework for consumer involvement that included proactive use of sources of published consumer evidence [ 7 ].
Lessons from these national and local examples may be useful to those undertaking local disinvestment initiatives.
High quality sources of research evidence are available and readily accessible through online resources, however there are some challenges to their use in the local health service setting.
Health service staff report lack of time, knowledge, skills and resources as barriers to searching for, accessing and appraising research; and that evidence is not used systematically or proactively to inform decisions [ 6 , 10 , 86 – 96 ]. Reports of HTAs undertaken by local health services [ 81 , 97 ] and decision-making for use of TCPs [ 2 , 98 – 100 ] note limitations in local processes, resources and expertise resulting in decision-making with varying degrees of rigour, structure and transparency. In addition to expertise, training and support, systematic prompts and triggers to use research evidence in all three types of decision-making are needed at the local level and could also be used to identify relevant TCPs for disinvestment or initiate discussions on potential disinvestment topics.
There are also limitations in coverage and applicability of currently available synthesised evidence to address all the needs of local decision-makers. The topics reviewed by national agencies are most frequently medical interventions, pharmaceuticals and diagnostic tests that have a high profile and are expensive as individual items. While these are obviously important in local health services, lower profile areas such as nursing and allied health practices, service delivery options, models of care and clinical consumable items, all of which have potential for considerable improvement in patient outcomes and reduction in costs and resource utilisation, are less commonly addressed in these formats, leading to locally-conducted HTA/HTR with the shortcomings noted above.
These limitations have additional implications for local health services given the lack of standardised methods for HTR [ 37 , 82 , 83 ]. Further research in this area has been proposed to develop consistent methods which will increase rigour, enable replication, enable comparison with others, facilitate application in equivalent situations to reduce duplication, engender familiarity and understanding to increase uptake and use of content, and build on existing work [ 28 , 29 , 83 ].
1.2 Health service data
Routine, reactive or proactive investigation of available data can identify potential opportunities for disinvestment. There are many generic tools like dashboards, statistical process control or balanced scorecards available to analyse health service data, however none were identified in this review of the disinvestment literature. These tools, plus simple data interrogation methods, can identify factors associated with TCPs that might be worthy of further exploration as candidates for disinvestment; for example high volume, high cost, long length of stay and high rates of mortality, adverse events, readmission or reoperation, and geographic variation [ 5 ].
Searching routinely-collected datasets for known ‘low value’ practices is a direct and potentially productive method of identifying disinvestment opportunities [ 38 , 101 , 102 ]. With initiatives such as Choosing Wisely proliferating, it is now less a case of list-making as list-taking and prioritising. An algorithm developed in the SHARE Program for selection and prioritisation of disinvestment projects from a catalogue of potential targets derived from the research literature using locally-developed criteria could be adapted for use with a collection of potential targets identified from investigation of local data [ 9 ].
There is a large body of literature on examination of practice variation [ 103 ]. Reporting on variations in healthcare practice has been done at national and regional levels and atlases of healthcare variation have been produced [ 104 – 108 ]. Similar processes could be undertaken at local level. Comparisons can be made between regions, facilities, departments and individual practitioners, or over time; but should only be done when the population demographics, socio-economic factors and particularly patient acuity are similar [ 5 , 21 , 73 , 105 , 109 , 110 ].
Recent studies have investigated practice variation specifically to identify ineffective practices; they note the potential to do so within local health services or for health services to benchmark against their counterparts [ 21 , 105 , 110 ]. Examination of health service utilisation and patient outcomes data, as well as differences in rates of prescribing, ordering diagnostic tests or use of specific interventions, could indicate inappropriate or suboptimal practices suitable for disinvestment. Procedures with high variability are often not on the ‘low value’ lists, indicating additional possibilities to identify disinvestment opportunities from this approach [ 21 ].
Use of local data clearly has potential but problems with data validity, reliability, comprehensiveness and degree of sensitivity to disinvestment requirements remain significant barriers [ 21 , 24 , 46 , 48 , 58 , 60 ].
There are many methods for analysis, synthesis and interpretation of data however, like research evidence, there is a lack of systematic prompts or triggers to use them [ 5 , 21 ]. While not specifically directed at disinvestment or resource allocation, a conceptual framework and logic model developed by Nutley and colleagues for improving data use in health system decision-making could facilitate a more proactive, systematic approach [ 111 , 112 ].
The aims of the SHARE Data Service were 1) to interrogate routinely-collected data to identify potential disinvestment opportunities and communicate this information to appropriate decision-makers and 2) to respond to requests from decision-makers to assess local data related to potential disinvestment opportunities that had been identified from the research literature [ 10 ]. Although the Data Service was not implemented due to unanticipated local factors, the decisions underpinning the design and the models proposed may be helpful to local health services wishing to establish similar resources to support use of data in the disinvestment process.
1.3 Stakeholder nominations
Stakeholder engagement is noted as a fundamental principle of the decision-making process and involvement of stakeholders and local ownership of decisions and projects are noted as facilitators of change in general [ 113 – 115 ] and in relation to disinvestment [ 21 , 58 , 72 , 82 ].
The Ontario Reassessment Framework gives priority to potential candidates for disinvestment if nominated by a clinical expert [ 85 ] and four frameworks for disinvestment employ applications from stakeholders in the identification process [ 9 , 16 , 35 , 36 ].
Participants in the SHARE Program noted that, while formal prompts and triggers could be built into existing decision-making infrastructure, there are also informal yet systematic approaches that could be integrated into other systems and processes to facilitate identification of opportunities for disinvestment by health service staff [ 9 ]. Examples are included in Table Table9 9 .
Additional systematic methods to facilitate identification of disinvestment opportunities in a local health service
| ▪ Discuss principles of disinvestment and examples of successful projects at department/unit meetings, educational events, etc. |
| ▪ Assign a group member to look for disinvestment opportunities in committee/working party decisions |
| ▪ Add a disinvestment question to the ‘Leadership Walkround’ protocol |
| ▪ Identify clinical champions interested in disinvestment in each program/department/unit who would look out for opportunities |
| ▪ Support staff who have undertaken a disinvestment project to look for more opportunities |
| ▪ Have disinvestment as a high priority in medication safety reviews |
| ▪ Encourage or require projects that are introducing something new to have a component of disinvestment |
| ▪ Review projects that are being conducted for other reasons and identify and focus on any disinvestment elements |
Stakeholder nomination can be a powerful contribution to the process, providing the nominated items are objectively scrutinised against additional identification and prioritisation criteria [ 109 ], however there are some considerations in the actual implementation.
Although evaluation of the applications in these frameworks is rigorous, based on explicit local criteria and health technology assessment, the process of how the topic was raised initially is not systematic or transparent. Applications can be received from any stakeholder for any reason. In this context they are likely to be driven by non-systematic factors such as clinician’s interests, information obtained from conferences or journal articles, or awareness of practice elsewhere [ 2 , 6 ]. “Understanding how the technology got on the agenda, where it came from and who was pushing for it” and the potential for “gaming by industry” are concerns reported by senior health decision-makers [ 116 ], but are often unclear in a stakeholder application process.
When invited to nominate candidates for disinvestment, clinicians have been found to be more likely to identify the practices of other professional groups than their own, practices that do not affect their revenue-generating services and practices of low impact [ 9 , 21 , 117 ].
Clarity of aims and objectives at the start of a project and clear rationale for change were in the top 10 considerations for successful disinvestment and one of three best practice recommendations arising from a Delphi study of international experts [ 52 ]. However lack of clarity and rationale have been noted as problems in identifying disinvestment opportunities [ 63 ], particularly from stakeholder applications [ 9 , 10 ].
These issues may create systematic biases in the choice of investment targets and miss some key opportunities. Unnecessary duplication of effort may also result, with individual facilities or regions undertaking extensive evaluations of the same topics.
1.4 ‘Low value’ lists
‘Low value’ lists are compilations of practices that have been demonstrated to have little or no benefit or potential to cause harm. They have been developed by governments and health agencies [ 118 – 120 ], commissioners of health services [ 121 ], professional bodies [ 65 , 122 , 123 ] and researchers [ 124 – 126 ]. Some of these lists are derived from research evidence, some are based on expert opinion and others from a combination of the two.
Duckett and colleagues separate them into ‘top down’ and ‘bottom up’ approaches, noting that each has benefits and drawbacks [ 73 ]. The ‘top down’ approaches, such as the UK National Institute for Health and Clinical Excellence ‘Do Not Do’ Recommendations [ 54 ], are described as providing the most consistent, objective, transparent and relevant evaluations. The ‘bottom up’ approaches, such as the Choosing Wisely program [ 74 ], highlight potentially ‘low value’ treatments and tests that should be carefully considered at the point of care.
Removing, reducing or restricting practices of little or no value clearly has merit, and ‘low value’ lists are likely to be very useful to health service decision-makers if they are based on sound evidence backed by expert consensus. However the definition of ‘low value’ is not always explicit and the validity and appropriateness of some of the lists and the ethics of their application have been questioned [ 117 , 125 , 127 – 130 ]. Potential users of ‘low value’ lists may wish to confirm the basis for claims made, in particular the definition being used and the use of systematic review evidence in the inclusion process [ 9 ].
The SHARE algorithm described earlier could also be applied to ‘low value’ lists to assess local applicability and facilitate prioritisation [ 9 ].
1.5 Economic approaches to priority setting
These priority setting approaches combine evidence from local data, expert opinion and stakeholder consultation [ 27 , 32 ].
PBMA applies the economic principles of opportunity cost and marginal analysis to determine priorities for health program budgets in the context of limited resources [ 131 ]. This method approaches disinvestment from the relative perspective, with decision-makers weighing up options for investment and disinvestment and reaching their preferred balance using locally-relevant criteria established by the stakeholders. The process is well-tested and guidance is available [ 27 ]. Although decision-makers acknowledge the usefulness of PBMA, it remains quite difficult to achieve in practice [ 24 , 48 , 131 ]. Another criticism is that it fragments the health sector into ‘program budget silos’ resulting in allocation and re-allocation of resources within, rather than between, programs which fails to identify more cost-effective options outside the program area [ 31 , 48 , 131 , 132 ].
In contrast to PBMA, the Health-sector Wide model is designed to shift the focus of priority setting away from program budgets towards well-defined target populations with particular health problems [ 31 ]. The condition-specific silos created here may be an improvement on program budget silos, but the model is more difficult to apply in local health services where funding decisions are not based on condition-specific populations.
The major limitations for all priority setting approaches include idiosyncrasies in cost-accounting, lack of sufficient high quality data to inform decision-making, and lack of time and appropriate skills of decision-makers to undertake the process and implement the decisions [ 24 , 27 , 46 , 48 , 55 , 131 ]. Lack of in-house expertise in health economics is a particular barrier at the local level [ 9 ].
2. Prioritisation and decision-making
Priority setting exercises clearly include a prioritisation process, however initiatives that identify their disinvestment targets by other means may need a specific prioritisation process to choose between the options available. Methods and tools for systematic, transparent and equitable decision-making may be used if prioritisation is not required or to complement the prioritisation process.
Prioritisation tools primarily focus on characteristics intrinsic to the TCP; however additional criteria may influence the decision to proceed with a disinvestment project in the local healthcare setting [ 9 ]. These might be pragmatic features that enhance initiatives chosen specifically as pilot or demonstration projects, such as opportunities for ‘quick wins’, or factors that affect the outcome of a project, such as likelihood of success and sustainability or potential usefulness of the evaluation.
There is a huge range of potentially relevant criteria for resource allocation decisions. Most authors emphasise that a list of criteria should be developed with input from all stakeholders to meet the objectives of individual situations. The commonly cited basic requirements include clinical parameters such as safety and effectiveness, economic measures such as cost-effectiveness and affordability, and social factors such as local values and priorities. Additional criteria will depend on the setting and context. Methods and tools to assist in assessment of safety and effectiveness [ 133 – 136 ] and use of economic measures [ 137 – 139 ] are available. Similar resources for consumer and community engagement are addressed in Additional file 1 .
Deciding between several alternatives is a complex process requiring consideration of multiple factors. Health service decision-makers are often not good at this, relying on heuristic or intuitive approaches which ignore potentially important information [ 140 ]. Methods such as burden of disease analyses, cost-effectiveness analyses and equity analyses focus on some but not all of the available information [ 140 ]. Multi-criteria decision analysis (MCDA) allows consideration of all factors simultaneously, and although used widely in other scientific disciplines, it has only been used in health care relatively recently [ 76 , 140 ].
The Star model, a “ socio-technical allocation of resources ” based on MCDA and health economic theory, has been piloted successfully in two settings, revised and developed into a toolkit [ 141 – 143 ]. MCDA is also the foundation of the Evidence and Value: Impact on DEcision Making (EVIDEM) framework, which is being investigated further through research conducted by the international EVIDEM Collaboration [ 144 ].
While the components of the A4R framework are included within several principles in the new framework, policy makers, managers and clinicians may also wish to use the A4R terminology specifically in their decision-making processes.
A4R is also the basis for the Systematic Tool for Evaluating Pharmaceutical Products for Public Funding Decisions (6-STEPPPs) [ 145 ] and A4R and MCDA have been combined in other decision-making applications [ 146 , 147 ].
Lists of criteria for consideration in prioritisation and decision-making have been published for disinvestment [ 78 , 82 , 85 , 109 , 148 ], including many who have applied or adapted the criteria framework proposed by Elshaug et al. [ 72 ]; resource allocation [ 6 , 149 – 151 ]; and general decision-making [ 42 ]. A tool to analyse gaps in priority setting has also been developed [ 152 ].
Many health service decision-makers use a prioritisation matrix, but most of these are developed locally and based on simple spreadsheets or business case templates [ 9 , 48 , 55 , 153 ]. This variety of tools makes it difficult to compare costs and outcomes more broadly and there is some scepticism amongst decision-makers about the lack of rigour, transparency and skills involved in their local programs [ 21 , 48 ].
There are also software applications to facilitate PBMA and generic prioritisation processes [ 27 , 154 , 155 ].
3. Development of a proposal
Once a decision has been made that there is a need for change, a proposal to meet that need and implement the decision is developed. When the proposal is drafted, the time and other resources required to implement and evaluate it can be assessed to determine if the benefits outweigh the costs of the exercise and to inform planning.
The range of potential disinvestment activities is broad and disparate. A proposal to remove a drug from a hospital formulary is likely to be very different to a proposal to close down an inpatient facility. No specific methods and tools were identified for developing disinvestment proposals, but generic materials for developing the program theory or rationale and defining the program logic would be useful [ 156 – 164 ], as would business case proformas and communication templates.
Proposals are more likely to be successful if they have certain favourable characteristics and new initiatives are more likely to be sustainable if there is appropriate availability and adequate provision of critical factors to achieve and maintain the proposed components and activities [ 20 , 165 – 167 ]. A checklist of the factors influencing likelihood of success and sustainability is available [ 8 ].
4. Implementation
Some successes with national approaches to disinvestment have been reported and may have elements that are generalisable to local circumstances [ 72 , 85 , 102 ]. However in some circumstances national approaches are not applicable at state/provincial, regional or institutional levels; for example removing or refining indications for reimbursement for ‘low value’ TCPs in national fee-for-service schemes for doctors in private practice may not apply to doctors working in state funded hospitals.
As noted above, there are also many examples in the EBP and quality and safety literature of successful projects at local level to remove unsafe or ineffective TCPs which are not labelled as disinvestment.
Many articles about disinvestment do not address implementation at all and some note that there are difficulties related to implementation but offer no solutions. Of those that do consider implementation, many of the comments are principles, captured in the section above, or barriers and enablers, captured below.
One recommendation for successful implementation is that “ we could create conditions that make it easy for people to avoid using low-value health care services ” [ 128 ]. Environmental changes such as closing services, physically removing products from storerooms and work areas, and eliminating items from formularies and purchasing catalogues should achieve this aim and result in complete cessation. In addition, if providers or recipients of a TCP, program or service receive financial reimbursement, removal of funding is likely to reduce use considerably, although not necessarily completely [ 64 , 72 , 117 , 168 , 169 ]. But not all disinvestment decisions can be managed with structural changes.
The need for an implementation strategy for each disinvestment activity is widely acknowledged. One disinvestment guideline details eight generic steps in their Action Plan [ 35 ], the SHARE Program used the SEAchange model for evidence-based change [ 41 ] to implement disinvestment pilot projects and support services [ 9 , 10 ], and a model for ‘de-adoption’ utilises the ‘Knowledge to Action’ framework [ 22 , 170 ].
A range of approaches to facilitate implementation of disinvestment decisions has been proposed. These include communication and educational materials [ 58 , 72 , 78 , 117 , 121 , 171 ]; financial incentives and pay-for-performance [ 59 , 64 , 72 , 117 , 168 ]; reinvestment of resources saved [ 29 , 78 , 80 , 172 ]; clinical champions [ 48 , 80 ]; clinical pharmacists to monitor and advise prescribers [ 68 ]; quality standards [ 59 , 117 ]; professional standards, maintenance-of-certification activities and practice audit [ 117 ]; prompts through guidelines, protocols, clinical pathways and decision support systems [ 5 , 58 – 60 , 72 , 82 , 168 , 171 ]; requirements to report variations from mandatory guidelines [ 59 , 72 ]; monitoring and reporting of outcomes [ 72 , 78 , 168 ]; public reporting of provider performance [ 59 , 117 , 168 ]; training and re-organisation of staffing and equipment [ 10 , 78 ]; and “ picking low hanging fruit ” before tackling more difficult projects [ 80 ]. These proposals have arisen from qualitative work with stakeholders or been derived from an understanding of implementation science; the papers offering these suggestions for implementation do not report application or evaluation of these strategies in the disinvestment context.
Several authors note that implementation is more likely to be successful if decisions are made at the local level, integrated into everyday decision-making and central to local planning [ 55 , 59 , 60 , 80 ]. A well-resourced and well-designed formal priority setting entity is reported to improve implementation of decisions [ 27 , 37 , 55 , 173 ]. It provides a recognised vehicle to consider information such as new evidence or local performance concerns, one which has transparent processes and appropriate authority for decision-making and action, where local expertise can be built up and local knowledge utilised. It is thought to “ make contentious decisions more palatable and defensible ” [ 55 ].
The SHARE Program used the Technology/Clinical Practice Committee (TCPC) as a formal decision-making structure [ 2 ]. After piloting several approaches, the Evidence Dissemination Service mentioned above as a method of identification, was finally implemented within a governance model to ensure maximum adherence [ 11 ]. Recently-published, high-quality synthesised evidence was identified and publications reporting evidence of harm, lack of effect or findings of a more cost-effective alternative to current practice were prioritised for dissemination. An Evidence Bulletin summarising an individual publication was provided to the TCPC, which then forwarded it to the department head or committee chair responsible for practice in the specific topic area. A response was required to confirm whether current practice was consistent with the evidence, and if not, what measures were being taken to address this or an explanation of why change was not required. When there was evidence of harm, responses to the TCPC were required within 1 month and the responses, or lack thereof, were reported to the Chief Executive the following month. Responses to other Evidence Bulletins were required in three or 6 months. A total of 175 publications were disseminated, 55 of the Evidence Bulletins required responses. Of the 43 responses received during the evaluation period, 32 reported that local practice was consistent with the evidence, six reported that the evidence was not applicable at Monash Health, three noted that local practice was not consistent with the evidence but provided a justifiable reason, and two reported that remedial action was planned to bring local practice into line with the evidence [ 11 ].
Although there are some particular challenges to asking people to stop doing things they believe in [ 1 ], the general principles of implementation should apply to disinvestment as they do for any practice change. These are summarised in the SEAchange model and the Knowledge to Action framework: engaging all stakeholders, identifying what is already known about practice change in the topic area from the literature and local knowledge, undertaking an analysis of local barriers and enablers, developing an implementation plan including strategies to minimise barriers and build on enablers, piloting and revising as required, and finally implementing in full [ 41 , 170 ].
5. Monitoring, evaluation and reporting
The Schmidt ‘Framework for disinvestment’ notes that both process and outcome evaluations should be undertaken but provides no details [ 16 ]. In their framework for evaluation of priority setting processes, Barasa and colleagues propose measures for both procedure aspects and outcomes [ 39 ] and a systematic review summarises a range of performance measures to assess use of ‘low value’ TCPs [ 174 ]. The ‘Integrative framework for measuring overuse’ lists measurement tools linked to specific project/program goals and discusses advantages and disadvantages of each approach [ 38 ].
The SHARE Evaluation Framework and Plan was created for an organisation-wide program of disinvestment in a local health service network [ 40 ]. It was developed in consultation with stakeholders and included evaluation domains, audience, scope, evaluation questions, sources of data, methods of collection and analysis, reporting and timelines. A theoretical framework and taxonomy adapted for evaluation and explication of disinvestment projects was also used to understand the process of disinvestment in the SHARE Program [ 9 ].
The deficiencies in available economic and usage data and lack of methods for quantifying savings are considered to be significant limitations to evaluation [ 46 , 60 , 82 , 175 , 176 ].
There are many generic guidance documents for monitoring and evaluation of health programs and projects in a range of settings. Like implementation, the principles, methods and tools for evaluation should be as appropriate for disinvestment as they are for any healthcare improvement project.
Findings from monitoring and evaluation activities should be reported on a regular and/or scheduled basis to the appropriate stakeholders in accordance with project terms of reference, governance protocols and other local requirements.
6. Reinvestment
This step will only apply in certain projects when it is anticipated that firstly resources will be released and secondly that they will be available for use elsewhere. Although there is considerable discussion about the potential for reinvestment or reallocation, there is little information about how to do it [ 1 ]. Resource release and reallocation are built into prioritisation processes for budget-setting but are not integral to other methods of disinvestment. One proposal for a “ sensible, well-managed reinvestment program” describes “a cost-accounting process to capture, and a financial strategy and analysis to return, a pre-agreed portion of real savings ” [ 172 ]. However the comments by other authors regarding inconsistencies in accounting practices, insufficient valid and reliable data, lack of methods and tools and absence of reported examples suggest that this may not be currently achievable [ 1 , 21 , 48 , 60 , 83 , 175 – 177 ].
7. Dissemination and diffusion
These terms have been used with specific, but inconsistent, meanings in the disinvestment literature. For example, diffusion has been used to refer to uptake of ‘new’ technologies where disinvestment is used for removal of ‘old’ technologies [ 178 ]. In contrast, diffusion and discontinuation have been used to represent ‘spontaneous’ uptake and removal of technologies where dissemination and disinvestment are their counterparts for ‘managed’ uptake and removal [ 21 ]. The former links disinvestment with diffusion, the latter with dissemination.
Since the focus of this framework is on implementation of change, and does not differentiate between implementation of investment or disinvestment decisions, the definitions of dissemination and diffusion are taken from the knowledge translation literature (Table (Table4) 4 ) [ 20 , 170 , 179 ]. Dissemination involves planned, active processes to share and spread information; diffusion is unplanned and passive.
Outcomes of disinvestment projects should be disseminated to others working in this area to fill gaps in knowledge, avoid duplication, build on successes and learn from mistakes and misfortune. However no guidance for systematic dissemination or facilitation of diffusion of successful disinvestment initiatives at the local health service level was identified. Guidance from the knowledge translation, EBP, QI and implementation science literature for dissemination and diffusion of new TCPs may be a useful starting point, however the specific challenges of disinvestment may influence the generalisability of these methods [ 1 , 180 ].
8. Maintenance
Maintenance is the final step in the change process. It involves strategies to sustain recently implemented change after project support is removed; to integrate the change into organisational systems, processes and practices; and to attain long-term viability of the change (Table (Table4). 4 ). Several terms are used in the broader health literature to capture this concept; examples include adoption, assimilation, sustainability and institutionalisation. Sustainability has been used in the context of disinvestment [ 3 , 8 , 22 , 169 , 181 ]. Maintenance is used in this framework to avoid confusion with use of the term ‘sustainability’ in a different context in the title of the SHARE Program. Maintenance is also used in the evaluation literature to assess “the extent to which a program becomes institutionalized or part of the routine organizational practices and policies” and can be applied to both the population targeted for behaviour change and the organisation that enacted or adopted the policy [ 182 ].
Montini and Graham propose that the disciplines of “Science and technology studies, the History and philosophy of science, the Sociology of health and illness, and Medical Anthropology” be explored to understand the factors relating to sustaining change related to ‘de-implementation’ [ 169 ]. Niven and colleagues recommend that ‘de-adoption’ interventions include a sustainability plan to prevent healthcare providers knowingly or unknowingly reverting to old practices [ 22 ].
The SHARE Program applied, adapted and developed methods and tools to facilitate sustainability of disinvestment-related initiatives at both the program and project level.
- SHARE projects were assessed against a framework for sustainability based on five categories: structure, skills, resources, commitment and leadership [ 8 ].
- The SEAchange model for sustainable, effective, appropriate evidence-based change in health services applied in SHARE projects includes formal assessment of sustainability at each step in the change process [ 41 ].
- The determinants of effectiveness outlined in a framework and taxonomy adapted for evaluation and explication of SHARE disinvestment projects could be considered in developing strategies for sustainability of new disinvestment interventions [ 9 ].
- The preconditions and underlying principles derived from the literature and local research in development of the SHARE model for exploring sustainability in health care by allocating resources effectively in the local health service setting were identified as factors related to success and sustainability of the whole SHARE Program [ 8 ].
Barriers and enablers
The terms barrier and enabler are commonly used to describe factors influencing the success of change initiatives in health care, but interestingly they are less frequent in the disinvestment literature. Most authors refer to the ‘challenges’ related to disinvestment, few refer to specific ‘barriers’. ‘Enablers’ or existing factors that could facilitate desired change are rarely mentioned, however many authors describe favourable conditions that represent the absence of specific negative factors or strategies that seek to remove them. The challenges and negative factors identified are interpreted as barriers and summarised in Table Table10 10 .
Examples of potential barriers to disinvestment
| Common to all aspects of disinvestment ▪ Lack of common terminology, theories, tested frameworks and models, proven methods and tools ▪ The word ‘disinvestment’ generates negativity and mistrust ▪ Divergent understanding of the concept of disinvestment between researchers and health service decision-makers ▪ Lack of guidance and/or successful examples to follow ▪ Lack of resources particularly time, funds and skills ▪ Lack of any of the elements of the framework ▪ Resistance to change |
| Establishment and delivery of program ▪ Lack of communication between agencies ▪ Autonomy of agencies resulting in multiple different systems ▪ Wastage of resources by duplication of effort, particularly in HTA ▪ Lack of resources to support policy mechanisms ▪ Lack of appropriate data collection systems ▪ Cost of appropriate data collection systems ▪ Lack of political, clinical, or administrative will to achieve change ▪ Difficulty establishing systems and processes to assess choices and reallocate resources across and between programs. Easier when done within programs but this has limited effectiveness. ▪ Difficulty establishing systems and processes between competing sectors or paradigms eg cure versus prevention, acute versus community care, drug therapy versus counselling ▪ Lack of coordination and integration of systems and processes ▪ Short-termism in government policy ▪ Conflicting priorities – at individual levels, and/or between levels ▪ System inertia ▪ Longstanding structures, institutional practices and organisational relationships ▪ Poor understanding of organisational practices and relationships ▪ Lack of established triggers to initiate disinvestment discussions ▪ Scarcity of strategic plans that include disinvestment ▪ Lack of incentives, presence of disincentives ▪ Fee for service models reward quantity not quality |
| Stakeholder engagement ▪ Lack of stakeholder commitment ▪ Stakeholder inertia ▪ Difficulty identifying and engaging multiple diverse stakeholders ▪ Resistance to, or lack of understanding of consumer participation |
| Identification of disinvestment opportunities ▪ Health Technology Reassessment (HTR) not conducted routinely ▪ Public and private funding focused on HTA rather than HTR ▪ Insufficient ‘unequivocal’ evidence to disinvest ▪ Lack of mechanisms to identify disinvestment targets ▪ Difficulties in producing, accessing & interpreting economic data ▪ Willingness to use lower quality evidence to maintain status quo |
| Prioritisation and decision-making ▪ Lack of knowledge of available tools ▪ Unfamiliarity with economic evaluations ▪ Disagreement with assumptions in economic evaluations ▪ Difficulties estimating marginal costs ▪ Reluctance to disinvest if there are sunk costs in existing technology and supporting capital infrastructure ▪ Reluctance to expend effort in disinvestment if benefits not clear ▪ Gains from disinvestment are less readily measured and may not happen but losses from disinvestment are immediate ▪ Strength of vested interests and lobby groups ▪ Lack of negotiating skills making it difficult to resist opposition ▪ Conflicting priorities between decision-makers ▪ Conflicting priorities between local, regional and national levels ▪ Reluctance to disinvest due to heterogeneity of outcomes and/or if there is potential for benefit in some subgroups or individuals ▪ Controversy associated with removal of an effective TCP in favour of a more cost-effective alternative and/or where there is lack of evidence of effect but general perception that it works ▪ Sensitivity of disinvestment target eg children, cancer, end of life ▪ Lack of decision-making processes ▪ Lack of integration with other decision-making processes ▪ Requirement for prospective data collection or further research to provide enough information for decision ▪ Difficulty making choices and reallocating resources across and between programs. Easier when done within programs but this has limited effectiveness. ▪ Difficulty making choices between competing sectors or paradigms eg cure versus prevention, acute versus community care, drug therapy versus counselling ▪ Decision-makers not held in sufficiently high regard for decisions to be respected and enforced ▪ Perceived influence of power imbalances and hidden agendas ▪ Political challenges |
| Implementation ▪ Inadequate project timelines ▪ Lack of funding for implementation ▪ Lack of skills in project management ▪ Lack of skills in change management ▪ Loss of patient choice ▪ Loss of perceived entitlement to treatment ▪ Loss of clinical autonomy ▪ Clinician reluctance to remove practices they perceive as integral to their professional practice and identity ▪ Loss of perceived benefit of intervention being removed ▪ Perceived criticism of practice and/or practitioners ▪ Perception that management priority is only to save money ▪ Lack of incentives, presence of disincentives ▪ Lack of data to substantiate need ▪ Gains from disinvestment less readily measured and may not happen, but losses from disinvestment are immediate ▪ Complexity of practice change if disinvestment limited to certain groups or for certain indications ▪ Lack of coordination between projects resulting in gaps and duplication ▪ Stakeholder fatigue and disillusionment with constant change |
| Monitoring and evaluation ▪ Routinely-collected data not valid or reliable, often out-of-date ▪ Routinely-collected data not precise or specific enough ▪ Cost of obtaining appropriate data ▪ Lack of post-market surveillance ▪ Lack of methods to quantify savings ▪ Distrust of reasons for monitoring and evaluation |
| Reinvestment ▪ Lack of methods for reallocating resources released ▪ Lack of examples of successful reinvestment ▪ Some cost savings may not be realised eg length of stay reduced but beds immediately filled with other patients of greater acuity |
| Research ▪ Assumptions that current practice is effective ▪ Ethical objections to randomising patients to control groups ▪ Resistance to enrolling patients in trials due to belief in intervention ▪ Difficulty getting funding to research existing practices |
Some barriers impact on all aspects of disinvestment across each level of influence [ 15 , 16 , 21 , 24 , 29 , 48 , 58 , 78 – 80 , 83 , 116 , 120 , 129 , 175 , 178 , 183 – 187 ]. Barriers to establishment and delivery of a program for decision-making are noted [ 8 , 9 , 24 , 31 , 55 , 58 , 64 , 79 , 82 , 120 , 131 , 132 , 153 , 175 , 183 ] and other barriers are categorised using the steps of the disinvestment process: stakeholder engagement [ 2 , 58 , 78 – 80 , 82 , 120 , 153 ], identification of disinvestment targets [ 8 , 9 , 16 , 21 , 24 , 46 , 48 , 58 , 60 , 63 , 72 , 79 , 82 , 120 , 129 , 175 , 183 , 188 – 190 ], prioritisation and decision-making [ 2 , 21 , 24 , 31 , 46 , 48 , 55 , 58 , 60 , 63 , 64 , 72 , 79 , 82 , 120 , 129 , 132 , 175 , 183 , 188 , 190 , 191 ], implementation [ 2 , 8 , 21 , 46 , 58 , 64 , 79 , 82 , 120 , 132 , 153 , 169 ], monitoring and evaluation [ 8 , 46 , 48 , 60 , 82 , 175 ], reinvestment [ 55 , 64 , 153 , 175 , 176 ] and research [ 58 , 183 , 189 ]. There is some overlap where the same barriers affect more than one aspect of the process.
This summary only captures barriers to disinvestment activities. Barriers and enablers to investment in new TCPs and strategies to address them are summarised elsewhere [ 2 ]. Programs for disinvestment may require system reform, so the barriers inherent in large-scale change will also be applicable. The body of literature on barriers and enablers to using evidence in decision-making and implementing practice change will also be relevant to disinvestment activities.
In addition to the list summarised here and the wider literature, an analysis of local barriers and enablers should be undertaken for every project to identify crucial contextual factors.
Limitations
Although a rigorous systematic approach was taken, it is impossible to be comprehensive in ascertaining all the relevant literature on disinvestment; the reasons are outlined in the conceptual review [ 1 ]. As a result, some relevant publications may not have been identified and some information may not have been published. Despite these limitations, the messages about operationalising disinvestment are generally clear and consistent and provide strong underpinnings for the framework.
The literature has been reviewed from the perspective of a local health service, however the authors’ experience is based in the Australian health system; hence differences with other health systems may not have been recognised and additional decision-making settings or methods and tools may have been missed.
The specific details of the ‘where, who and how’ of decision-making is likely to differ between organisations but the underlying premises should be the same: individuals and groups make decisions under certain conditions. The classifications of decisions and decision-makers might be useful starting points to elucidate local particulars.
The proposed framework is conceptual and untested. Naming of categories, determination of their constituent elements and the relationships between components has not been piloted or refined with stakeholder input. It is large, complex and all-encompassing and may prove too daunting or complicated to be achieved in this format. Testing and research may establish if it is feasible in the current overarching format or if it should be renamed, redefined or reformulated for implementation in smaller sections.
The framework is proposed at the ‘big picture’ level and requires supplementation with detail for all the components. There are some existing frameworks, models, methods and tools that can be applied in several areas but not for all elements within the framework.
There are many barriers that cannot be addressed by generic system changes and must be tackled when implementing the framework in individual situations. Many of these may be successfully overcome with local strategies; however some aspects of the framework involve potentially insurmountable barriers in the current environment. The main example is lack of valid, reliable, timely, appropriate and sufficiently specific data to identify disinvestment targets and monitor and evaluate disinvestment initiatives.
Implications for policy and practice
As the focus of this review is operationalisation of disinvestment, the implications for policy and practice have been integrated throughout the paper.
Implications for research
The implications for research in operationalising disinvestment are enormous. Placing the research component of the proposed framework across all the constituent elements illustrates that there is a need for research in each of them. Some topics stand out as priorities.
Many authors report a lack of frameworks, models, methods or tools for disinvestment. However there are some frameworks and models for disinvestment, although not tested; and plenty of methods and tools, many of which are tested, frequently from other research disciplines but which are relevant for disinvestment projects. Perhaps a more important factor is the lack of proactive mechanisms, prompts and triggers [ 9 , 11 , 16 , 21 , 24 , 27 , 192 ]. There are rigorous methods for HTA and analysis of health service data but no systematic methods to initiate these processes or draw the results to the attention of health service decision-makers. It is also not clear who is, or should be, responsible for instigating and making decisions and taking action. Research in these areas is a priority.
Investigation of data requirements, data collection methods and skills of decision-makers to use data for disinvestment is another priority [ 21 , 24 , 27 , 46 , 48 , 55 , 58 , 60 , 131 ]. Support for data collection after a TCP has been introduced is low and research into methods and resources required for post-market surveillance and “ coverage with evidence development ” is required [ 24 , 132 ].
Some authors have highlighted other aspects of disinvestment for research such as exploring disinvestment at local health service and individual practitioner level [ 16 , 55 , 56 , 80 , 188 , 193 ], taking a longitudinal approach from inception through implementation to outcomes that cross organisational boundaries [ 80 , 188 ], identifying determinants for disinvestment [ 15 , 80 , 129 ], implementing change management [ 56 , 58 ], and drafting and refining frameworks, methods and tools [ 15 , 24 , 29 , 58 , 129 , 175 , 184 , 185 ]. Mechanisms to develop, implement and evaluate disinvestment activities can be built on existing theoretical frameworks from other research paradigms such as HTA, knowledge translation and implementation science [ 28 , 83 ]. Measures of impact, potential unintended consequences and factors contributing to success or failure also need to be captured [ 24 , 83 , 193 ]. The SHARE Program provides some early work to build on by reporting disinvestment projects from inception to implementation [ 9 ]; identifying determinants for disinvestment, potential unintended consequences and factors contributing to success or failure [ 9 ]; and developing frameworks, models and algorithms [ 5 – 9 , 11 ] and evaluation frameworks and plans [ 10 , 11 , 40 ]. These outputs of the SHARE Program are summarised in Paper 1 [ 3 ].
Research could also include testing the proposed framework in different contexts.
There is no agreed definition or common understanding of disinvestment, yet the concept is widely discussed and disinvestment initiatives and research are called for. Although there are only a few, largely untested, frameworks and models and little practical guidance in the literature, there are clear and consistent messages regarding principles for decision-making, settings and opportunities to identify disinvestment targets, steps in the disinvestment process, methods and tools, and barriers and enablers. This information has been drawn together into a framework for operationalising disinvestment in a systematic, integrated, organisation-wide approach in the local healthcare setting.
Definitions for essential terms are proposed and key concepts underpinning the framework have been made explicit. The term disinvestment is used in the broadest sense, ‘removal, reduction or restriction of any aspect of the health system for any reason’, and can be applied to products, devices and equipment; clinical practices and procedures; health services and programs; information technology and corporate systems. Given the negative connotations of the word and the problems inherent in considering disinvestment in isolation, the basis for the framework is ‘resource allocation’ addressing the spectrum of decision-making from investment to disinvestment.
The framework is based on three components: the program consists of principles for decision-making and settings that provide opportunities to introduce systematic prompts and triggers to initiate consideration of disinvestment; projects follow the steps of the disinvestment process; and research is needed across all aspects of the framework.
The proposed framework can be employed at network, institutional, departmental, ward or committee level. It is proposed as an organisation-wide application, embedded within existing systems and processes, which can be responsive to needs and priorities at the level of implementation. It can be used in policy, management or clinical contexts, for resource allocation and potentially other decision-making processes.
There are many theories, frameworks, models, methods and tools from other areas of health research and practice that are relevant to disinvestment which could be employed within this framework.
Multiple barriers to establishing a decision-making framework and implementing disinvestment initiatives were identified. Some of these relate to the lack of elements that form individual principles and are addressed in the framework, however many involve local factors that can only be tackled when implementing the framework in particular contexts.
The framework captures all the identified information from the literature about operationalisation of disinvestment in the context of resource allocation. This could be a strength, if all the elements are required for a robust effective program of decision-making and action, or a weakness, if it is too complex to be achieved in practice.
Acknowledgements
The authors would like to thank Violet Marion and Kelly Allen for assistance in development and revision of the framework, Tari Turner for critical comments on the manuscript, and Richard King for co-supervision of CH’s PhD.
The SHARE Program was funded by Monash Health and the Victorian Department of Human Services. No conditions related to the project or subsequent publications were imposed. This review was undertaken as part of an unfunded PhD.
Availability of data and materials
Abbreviations.
| A4R | Accountability for Reasonableness |
| EBP | Evidence Based Practice |
| EVIDEM | Evidence and Value: Impact on DEcision Making |
| HsW | Health Sector Wide |
| HTA | Health Technology Assessment |
| HTR | Health Technology Reassessment |
| MCDA | Multi-criteria decision analysis |
| NICE | National Institute of Health and Clinical Excellence |
| PBMA | Program Budgeting and Marginal Analysis |
| QI | Quality Improvement |
| SHARE | Sustainability in Health care by Allocating Resources Effectively |
| STEPPP | Systematic Tool for Evaluating Pharmaceutical Products for Public Funding Decisions |
| TCPC | Technology/Clinical Practice Committee |
| TCPs | Technologies and Clinical Practices |
Additional file
Principles for resource allocation. (PDF 697 kb)
Authors’ contributions
CH and SG developed the conceptual approach. CH undertook the literature review and drafted the framework and initial manuscript. SG provided critical revisions to both. AGE provided critical revisions and proposed refinements and changes to scope. All authors read and approved the final manuscript.
Authors’ information
CH was the Director of the Centre for Clinical Effectiveness and the SHARE Program Director. CH undertook this review and completed the SHARE publications as part of an unfunded PhD. SG is Professorial Fellow in the Monash University School of Public Health and Preventive Medicine and co-supervisor of CH’s PhD. AGE is Professor of Health Policy, HCF Research Foundation Professorial Research Fellow, and Co-Director of the Menzies Centre for Health Policy at The University of Sydney and Senior Fellow with the Lown Institute in the USA.
Ethics approval and consent to participate
The Monash Health Human Research and Ethics Committee (HREC) approved the SHARE program as a Quality Assurance activity. Further ethical review was not required as the program met the following criteria [ 194 ]:
▪ “The data being collected and analysed is coincidental to standard operating procedures with standard equipment and/or protocols;
▪ The data is being collected and analysed expressly for the purpose of maintaining standards or identifying areas for improvement in the environment from which the data was obtained;
▪ The data being collected and analysed is not linked to individuals; and
▪ None of the triggers for consideration of ethical review are present.” [ 194 ]
Participation was based on the ‘opt-out approach’ [ 194 ]. “The opt-out approach is a method used in the recruitment of participants into an activity where information is provided to the potential participant regarding the activity and their involvement and where their participation is presumed unless they take action to decline to participate.” [ 194 ] Consent to participate was approved by the HREC based on the following criteria:
▪ Health care providers, managers, consumer representatives, and officers within government health departments will be informed about the project and the processes and invited to participate.
▪ Participation in interviews, workshops and/or surveys will be considered to be implied consent.
These conditions were met.
Consent for publication
Not applicable
Competing interests
AGE receives salary support as the HCF Research Foundation Professorial Research Fellow, and holds research grants from The Commonwealth Fund and Australia’s National Health and Medical Research Council (ID 1109626 and 1,104,136). AGE receives consulting/sitting fees from Cancer Australia, the Capital Markets Cooperative Research Centre-Health Quality Program, NPS MedicineWise (facilitator of Choosing Wisely Australia), The Royal Australasian College of Physicians (facilitator of the EVOLVE program) and the Australian Commission on Safety and Quality in Health Care, and as a member of the Australian Government Department of Health’s Medicare Benefits Schedule Review Taskforce.
CH and SG declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Claire Harris, Email: [email protected] .
Sally Green, Email: [email protected] .
Adam G. Elshaug, Email: ua.ude.yendys@guahsle .
Research Voyage
Research Tips and Infromation
8 Effective Strategies for Managing Research Time

1. Set Specific Goals
2. prioritize tasks, 3. break tasks into smaller pieces, 4. create a schedule, 5. take breaks, 6. use technology to your advantage, 7. stay organized, 8. outsourcing certain tasks, introduction.
Effective time management is crucial for successful research projects. When you are conducting research, you need to balance a variety of tasks, such as collecting data, analyzing results, and writing up your findings. Without proper time management, it can be easy to get overwhelmed and fall behind schedule.
Time management refers to the process of planning and organizing how much time to allocate to different tasks and activities to make the most of the available time. Time management involves breaking down complex projects into smaller, more manageable tasks, prioritizing those tasks, creating a schedule, taking breaks, and using technology and outsourcing to streamline the research process.
In this post, we’ll explore these strategies in detail and offer tips on how to apply them to your own research projects. Whether you’re a seasoned researcher or just starting out, this post will help you to maximize your productivity and achieve your research goals with ease.”
In this post, we will explore several strategies for managing research time, including:
- Setting specific goals: By defining clear goals for your research project, you can prioritize your tasks and stay on track.
- Prioritizing tasks: You can use techniques such as the Eisenhower matrix to prioritize your research tasks and maximize your productivity.
- Breaking tasks into smaller pieces: By breaking larger tasks into smaller, more manageable pieces, you can work more efficiently and stay focused.
- Creating a schedule: A schedule can help you allocate your time effectively and ensure that you are making progress towards your goals.
- Taking breaks: Taking regular breaks can help you stay focused and productive, and prevent burnout.
- Using technology to your advantage: You can leverage tools such as citation managers, project management software, and communication apps to streamline your research process.
- Staying organized: Staying organized throughout your research project can help you avoid distractions and ensure that you are making progress towards your goals.
By using these strategies, you can manage your research time more effectively and achieve better results. Let’s see these strategies in detail in the next sections.
Setting specific goals is essential for managing research time effectively. Without clear goals, it can be difficult to stay focused and on track. Specific goals allow you to break down your research project into smaller, achievable tasks, making it easier to manage your time and measure progress.
Here are some tips on how to set specific goals for your research project in the computer science domain:
- Identify your research question: Start by identifying the main question or problem that you want to investigate. For example, if you are researching machine learning algorithms, your question might be, “What is the most effective algorithm for predicting user behaviour based on website activity?”
- Break down your research question into smaller tasks: Once you have identified your research question, break it down into smaller, more specific tasks. For example, you might need to review the existing literature on machine learning algorithms, collect data on website activity, test different machine learning algorithms, and analyze your results.
- Create a timeline for each task: After breaking down your research question into smaller tasks, create a timeline for each task. Assign specific deadlines to each task, and make sure that you allocate enough time to complete each task thoroughly.
- Measure progress: As you work on your research project, measure your progress towards your goals. This can help you stay motivated and adjust your timeline if necessary. For example, if you find that you are falling behind schedule on a specific task, you may need to adjust your timeline or allocate more time to that task.
By setting specific goals and breaking down your research project into smaller, manageable tasks, you can effectively manage your research time and stay on track towards achieving your research objectives.
Prioritizing tasks is crucial for effective time management in research projects. With so many tasks to complete, it is essential to focus on the most important tasks first, to make sure that you are making progress towards your research goals.
Here are some tips on how to prioritize tasks for your research project in the computer science domain:
- Use the Eisenhower matrix: The Eisenhower matrix is a popular time management tool that can help you prioritize your tasks based on their importance and urgency. To use this tool, divide your tasks into four categories: urgent and important, important but not urgent, urgent but not important, and neither urgent nor important. Then, prioritize your tasks accordingly.
- Consider the potential impact of each task: Some tasks may have a greater impact on your research project than others. For example, analyzing the data you have collected may be more critical to your project’s success than organizing your notes. By considering the potential impact of each task, you can prioritize your tasks more effectively.
- Identify dependencies: Some tasks may depend on others being completed first. For example, you may need to finish collecting data before you can start analyzing it. By identifying dependencies between tasks, you can prioritize tasks more effectively and make sure that you are not wasting time on tasks that cannot be completed yet.
- Focus on your research goals: Ultimately, your research goals should guide your task prioritization. Make sure that you are focusing on tasks that will help you achieve your research objectives. For example, if your research goal is to develop a new algorithm for analyzing website data, you should prioritize tasks related to algorithm development over administrative tasks like organizing your notes.
By prioritizing tasks effectively, you can make sure that you are making progress towards your research goals and using your time most efficiently.
Breaking tasks into smaller, more manageable pieces is helpful for managing research time because it allows you to focus on one task at a time and avoid feeling overwhelmed. It also makes it easier to measure progress and adjust your timeline if necessary.
Here are some examples of how to break a large research project into smaller, more manageable tasks in the computer science domain:
- Literature review: If your research project involves reviewing existing literature, you can break this task into smaller pieces by focusing on specific subtopics or keywords. For example, you can start by searching for literature related to the specific machine learning algorithm you are investigating, and then narrow your search to include only recent publications or publications from top-tier conferences. I have written an articles on “ How to write a better Survey Paper in 06 easy steps? “. and Top 10 Rules to Identify Keywords for your Research Paper . Thsese articles will be helpful for literature review process.
- Data collection: If your research project involves collecting data, you can break this task into smaller pieces by focusing on specific sources or types of data. For example, you can start by collecting data from a small sample of websites or users, and then gradually increase your sample size as you become more proficient at data collection.
- Algorithm development: If your research project involves developing a new algorithm, you can break this task into smaller pieces by focusing on specific components or features of the algorithm. For example, you can start by developing a prototype of the algorithm and testing it on a small dataset, and then gradually refine the algorithm and test it on larger datasets. You can refer my article on How to Write the Method Section of your Research Paper in 03 Simple Steps? . This article will help you in developing the algorithm.
- Results analysis: If your research project involves analyzing results, you can break this task into smaller pieces by focusing on specific metrics or aspects of the data. For example, you can start by analyzing the accuracy of your algorithm on a small dataset, and then gradually expand your analysis to include other metrics such as precision and recall. Refer my article on How to write Results Section of your Research Paper . This article will take you through the detailed result analysis process.
By breaking large research projects into smaller, more manageable tasks, you can stay focused, measure progress, and adjust your timeline if necessary. It can also help you avoid feeling overwhelmed and make it easier to manage your time effectively.
Creating a schedule is essential for managing research time because it helps you stay organized and accountable. A schedule can help you plan your time effectively and ensure that you are making progress towards your research goals.
Here are some tips on how to create a schedule that works for you in the computer science domain:
- Identify your most productive times: Some people are more productive in the morning, while others work best in the afternoon or evening. Identify your most productive times and schedule your most challenging tasks during those times.
- Block off time for specific tasks: Once you have identified your most productive times, block off time in your schedule for specific tasks. For example, you can schedule time for a literature review in the morning, data collection in the afternoon, and algorithm development in the evening.
- Use a project management tool: There are many project management tools available that can help you create a schedule and track your progress. For example, you can use Trello or Asana to create a project board and add tasks and deadlines.
- Be realistic: When creating a schedule, be realistic about how long each task will take. Consider factors like the complexity of the task and any potential roadblocks. This will help you avoid overloading your schedule and feeling overwhelmed.
- Leave room for unexpected tasks: Research projects often involve unexpected tasks that can throw off your schedule. Leave some buffer time in your schedule to account for these tasks.
By creating a schedule that works for you, you can make sure that you are using your time most efficiently and making progress towards your research goals. It can also help you avoid feeling overwhelmed and ensure that you are staying on track with your project timeline.
Taking breaks is essential for managing research time because it helps prevent burnout, improves productivity, and boosts creativity. When you take breaks, you give your brain a chance to recharge and reset, which can help you stay focused and engaged in your research project.
Here are some tips on how to take effective breaks that will help you recharge and stay productive:
- Schedule breaks into your day: Plan for breaks in your daily schedule and take them regularly. Taking short breaks every hour or so can help you stay focused and avoid burnout.
- Get up and move: Sitting in front of a computer for long periods can be tiring and bad for your health. Get up and move around during your breaks. Take a walk outside, do some stretching, or try some simple exercises to get your blood flowing.
- Do something different: Engage in activities that are different from your research work during your breaks. For example, you could listen to music, read a book, or do a crossword puzzle. Doing something different can help you shift your focus and recharge your brain.
- Disconnect from technology: It’s essential to disconnect from technology during your breaks, especially if you spend a lot of time in front of a computer. Turn off your phone, log out of your email, and take a break from social media.
- Take longer breaks when needed: Sometimes, you may need longer breaks to recharge fully. For example, you could take a weekend off or plan a vacation. Taking longer breaks can help you come back to your research project with renewed energy and focus.
By taking effective breaks, you can manage your research time better, improve your productivity, and avoid burnout. Incorporate these tips into your daily routine to stay focused, engaged, and productive throughout your research project.
Technology can be a valuable tool for managing research time and streamlining the research process. Here are some ways in which technology can be used to your advantage:
- Use project management tools: There are several project management tools available that can help you keep track of your research tasks, deadlines, and progress. Some popular project management tools used in the computer science domain include Trello, Asana, and Jira .
- Use reference management software: Reference management software can help you organize and manage your research sources, citations, and bibliographies. Some popular reference management software tools include Zotero , Mendeley , and EndNote .
- Use collaboration tools: Collaborating with other researchers or team members is a crucial part of research. Using collaboration tools like Slack , Microsoft Teams , or Google Docs can help you communicate and work with others more efficiently.
- Use data analysis tools: If your research involves data analysis, there are several software tools available to help you analyze and visualize your data. Some popular data analysis tools include R , Python , and MATLAB .
- Use automation tools: Automation tools can help you save time by automating repetitive tasks, such as data entry or formatting. For example, you can use tools like Zapier or IFTTT to automate tasks across different software applications.
I have written articles on
- How Mendeley Reference Management Software makes Researcher’s Life Easy? and
- EndNote: The key to streamlining your research and writing process .
These articles will teach you the effective usage of Mendeley and EndNote software.
By using technology to your advantage, you can streamline your research process, save time, and stay organized. Incorporate these tools and resources into your research workflow to help manage your research time more effectively.
Staying organized is crucial for managing research time effectively. Here are some tips on how to stay organized throughout the research process:
- Use a file organization system: Use a consistent file organization system for your research files and documents. Create folders for each project or subproject, and use descriptive file names that make it easy to locate files quickly. I have written an article on How to Effectively Organize your Research Articles on your System . This article will help you to organize your files and folders effectively and optimally.
- Keep track of your references: Keep a record of all your research sources, including articles, books, and websites. Use reference management software to organize your references and citations. Visit my article on How to Write References for your Research Paper in IEEE Format Easily and Quickly .
- Use version control: Use version control software to keep track of different versions of your research documents and code. This can help you avoid confusion and save time when working on collaborative projects.
- Keep a research journal: Use a research journal to document your progress, ideas, and insights throughout the research process. This can help you stay focused and motivated, and can also serve as a valuable reference when writing your final report or paper.
- Use task lists and calendars: Use task lists and calendars to keep track of deadlines, meetings, and important tasks. This can help you prioritize your work and avoid procrastination.
By staying organized, you can minimize the time spent on searching for files or documents and avoid duplication of work, which will help you manage your research time more effectively. Incorporate these tips into your research workflow to help stay organized throughout the research process.
Outsourcing certain tasks can be beneficial for managing research time effectively, whether you’re in academia or part of the industry. Here are some tips on how to outsource certain tasks, including outsourcing tasks to your students in an academic setting or using internships to outsource tasks within the industry:
Benefits of outsourcing: Outsourcing can help you focus on the more important aspects of your research project, while still ensuring that all necessary tasks are completed. This holds true not only in the academic sphere but also within the industry. It can save time and money, especially for tasks that require specialized skills or equipment.
Examples of tasks that can be outsourced: In addition to tasks like data entry, transcription, software development, and data analysis, there are other avenues for outsourcing. If you’re an academic, you can involve your students by assigning them tasks that align with their skills and can contribute to their learning experience. In an industry setting, you can consider outsourcing tasks to interns who are eager to learn and gain practical experience in exchange for their contributions.
Outsourcing to students in academia: In an academic environment, you can leverage the skills and enthusiasm of your students to outsource certain tasks. This not only benefits you by reducing your workload but also provides students with hands-on experience and exposure to real-world research tasks. You can delegate tasks such as literature reviews, preliminary data collection, and even basic coding to your students, allowing them to actively contribute to the research process.
Outsourcing tasks as internships in the industry: If you’re part of the industry, internships can serve as a valuable outsourcing method. By offering internships to students or entry-level professionals, you can delegate tasks like market research, content creation, or prototype testing. Interns can gain practical exposure to the industry while assisting you with tasks that might be time-consuming but necessary for your projects.
Finding a reputable outsourcing partner or intern: Regardless of whether you’re working with students or interns, it’s essential to find individuals who are reliable and enthusiastic about contributing to your research or projects. In academia, you can collaborate with students who demonstrate a keen interest in the subject matter. In the industry, you can recruit interns through university partnerships or industry-specific platforms.
Working with an outsourcing partner or intern: To ensure successful collaboration, clear communication is key. Provide detailed instructions, set expectations, and establish deadlines. Regular check-ins and updates will help you monitor progress and address any concerns. For both students and interns, offering guidance and mentorship can enhance their learning experience and the quality of their contributions.
By outsourcing tasks to students in academia or using internships in the industry, you can free up valuable time to focus on critical aspects of your research or projects. Simultaneously, you empower the next generation of researchers or professionals by providing them with practical opportunities to learn and grow. This collaborative approach benefits everyone involved and contributes to the overall success of the research or industry endeavours.
Managing research time is crucial for the success of any research project. Here are the main points discussed in this post:
- Setting specific goals is important for managing research time effectively.
- Prioritizing tasks can help you stay on track and make the most of your time.
- Breaking tasks into smaller pieces can make them more manageable and less daunting.
- Creating a schedule can help you stay organized and ensure that you are making progress on your project.
- Taking breaks is important for recharging and maintaining productivity.
- Technology can be a powerful tool for streamlining the research process.
- Staying organized is crucial for managing research time effectively.
- Outsourcing certain tasks can save time and resources.
We encourage readers to try out these strategies to manage their research time more effectively. By setting specific goals, prioritizing tasks, breaking tasks into smaller pieces, creating a schedule, taking breaks, using technology, staying organized, and outsourcing certain tasks, researchers can maximize their productivity and achieve their research goals.
Remember, managing research time is an ongoing process, and it is important to regularly assess and adjust your strategies to ensure that you are making the most of your time. We hope that these tips will be helpful in managing your research time effectively.
Upcoming Events
- Visit the Upcoming International Conferences at Exotic Travel Destinations with Travel Plan
- Visit for Research Internships Worldwide

Recent Posts
- 05 Quick Review, High Impact, Best Research Journals for Submissions for July 2024
- Top Mistakes to Avoid When Writing a Research Paper
- Average Stipend for Research/Academic Internships
- These Institutes Offer Remote Research/Academic Internships
- How to Include Your Journal in the UGC-CARE List? A Guide for Publishers
- All Blog Posts
- Research Career
- Research Conference
- Research Internship
- Research Journal
- Research Tools
- Uncategorized
- Research Conferences
- Research Journals
- Research Grants
- Internships
- Research Internships
- Email Templates
- Conferences
- Blog Partners
- Privacy Policy
Copyright © 2024 Research Voyage
Design by ThemesDNA.com

- Contact sales
Start free trial
What Is Resource Allocation? How to Allocate Resources for Projects
Projects require many resources. Everything from the people you’re working with and the equipment they’re using, to the materials and other supplies you need to even the site where you’re working falls under the umbrella of project resource allocation. Let’s explore what resource allocation is, why it’s so important for project management and what tools you can use to better allocate your project resources.
What Is Resource Allocation?
Resource allocation is the process of scheduling resources such as labor, materials or equipment to complete tasks. Organizations need resources to carry out the processes they operate normally and to execute operational and strategic projects to achieve specific goals.
This means the resource allocation process is integral in project management and strategic planning. Here’s a quick overview of the importance of resource allocation in these two areas.
Resource Allocation in Project Management
Resource allocation is a step in the larger project resource management process that involves estimating resources, procuring resources, allocating resources and tracking resources until the project is completed. The main objective of the project resource allocation stage is to ensure that resources are spent as efficiently as possible to minimize costs and avoid delays.
If a project team overspends resources on a task, the whole project schedule and budget might be affected as these resources need to be acquired again, generating additional costs and possibly extending the project timeline.
Once you’ve acquired your project resources, you should use project management software to plan how they’ll be allocated. That way you can coordinate them with your project schedule and distribute them across your team. In ProjectManager , for instance, you can manage your project schedule, team and non-human resources in one place. Build your schedule on a Gantt and track your resource distribution, progress and labor costs in one software. Try it free today!

Resource Allocation in Strategic Management
Resource allocation plays an important role when an organization is planning its business strategy for the future. This is described in a document known as the strategic plan, which outlines the key goals and objectives of the organization for a period from three to five years.
These goals and objectives are accompanied by an action plan detailing the actions, projects and strategic initiatives the organization will take to achieve them. All of these require resources , which need to be acquired, allocated and monitored.
Why Is Resource Allocation Important?
As difficult as it might be to allocate resources correctly over the life cycle of a project, it’s an essential part of any thorough project management plan and should be done in the planning stage of a project. This keeps costs down, maximizes productivity and helps with team morale. It also facilitates client satisfaction by achieving the best outcome and successfully delivering the project.
What Is a Resource Allocation Plan?
A resource allocation plan describes in detail what resources will be utilized for each project task, noting quantities, specifications and due dates for their utilization. There’s no standard way of making a resource allocation plan, it might include a variety of resource management charts such as a resource allocation graph, project calendar, Gantt chart or any other diagram that can be used to visualize how resources are allocated over a project timeline or a project task list.
In most cases, the resource allocation plan is part of the resource management plan , a document that guides all the project team’s resource management efforts.
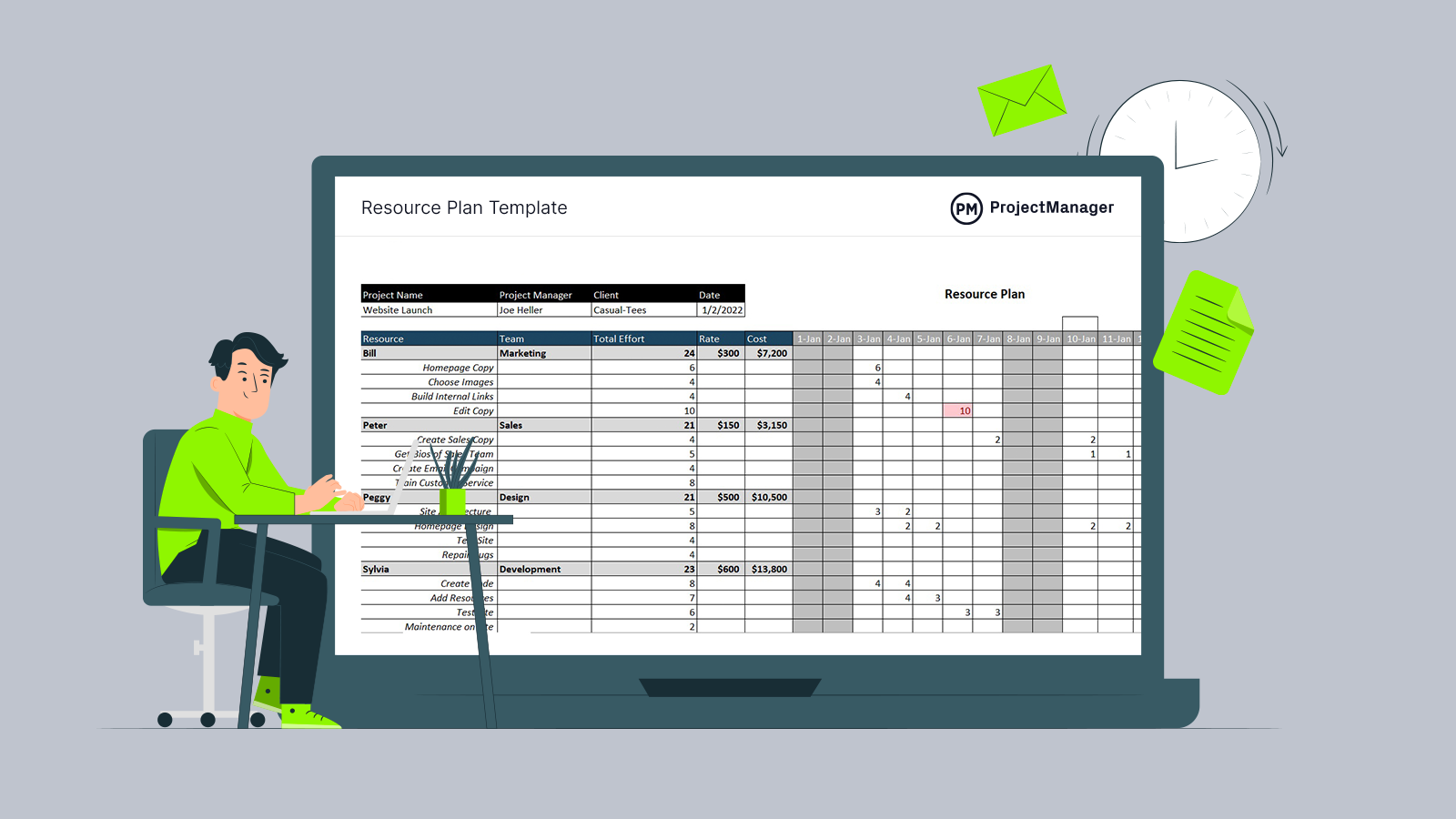
Get your free
Resource Planning Template
Use this free Resource Planning Template for Excel to manage your projects better.
What Does a Resource Allocator Do?
A resource allocator can take many different names, but essentially this is a role that acts as a liaison between the project management office and HR, finance, accounting or any other business departments throughout the organization to ensure that project resources are acquired and allocated effectively.
Resource Allocation Software
Resource allocation software is equipped with resource management tools that help organizations allocate resources for the completion of projects or operational activities and processes. For example, ProjectManager is a robust project management software with advanced resource allocation features such as Gantt charts, workload management charts, timesheets, real-time dashboards and much more. These tools will help make a resource schedule , reallocate resources, track resource availability and utilization rate and much more.
Resource Allocation Methods
The specific resource allocation method your organization implements depends on your industry and the nature of how resources are managed. For example, manufacturing companies might focus on raw materials and equipment while a professional services company might focus on team utilization and financial resources.
Regardless, it’s important to balance resource allocation with involved stakeholders . This could include teams, departments, customers, shareholders and other stakeholders. We’ve outlined some commonly utilized resource allocation methods for you to consider.
- Critical Path Method: In project management, the longest chain of dependent tasks is referred to as the critical path . By outlining a straightforward priority for task completion before the project starts, the CPM helps use resources as efficiently as possible. However, one criticism is that this method doesn’t allow for multitasking.
- Resource Leveling: To implement resource leveling , start by looking at the capacity of your team to determine how much work they can handle. Compare this with demand. If resources aren’t aligned with demand, reschedule tasks accordingly.
- Resource Smoothing: Resource smoothing aims to reduce demand while executing the project within the ideal timeframe. During this method, the project manager makes adjustments to resource scheduling and allocation. For example, if you’re under a time crunch, you might bring on a more seasoned person who can complete the work faster.
Resource Allocation Tools
Now that we’ve explained some popular resource allocation methods, let’s examine some of the tools project managers can use along the way.
Gantt Charts
Gantt charts provide an easy way to map the required project tasks and note dependencies. You’ll be able to see and allocate your resources across a project timeline, so you know exactly when you’ll need each resource. Once you’ve identified your tasks, you can assign them on the Gantt chart and see how long each team member has spent working on each task.

Workload Charts
These project management charts visually represent your resource allocation for your project team, department or entire company. You can see how many hours each person has been assigned and make adjustments to ensure your team is working at capacity. Use it to quickly determine how your human resource management aligns with your planned resource allocation.

Resource Allocation Matrix
A resource allocation matrix is an overview of the needed project resources. It helps identify any potential bottlenecks or imbalances ahead of time. Typically, the matrix includes the names and roles of each team member, their availability and their skills and tasks on the project. It acts as a visual representation of your resources mapped against project tasks and activities.
Resource Breakdown Structure
This resource allocation tool is a hierarchical chart of the resources needed to execute your project and it includes everything from the people needed for the project to what you’ll be spending your money on. An RBS can include materials, equipment, people, project management tools and more.
Resource Allocation Templates
Resources allocation requires accurate and timely data to avoid bottlenecks that can slow down your project. Project management software is the most efficient way to manage your resources, but if you don’t have an online resource management tool some templates can help. ProjectManager has free project management templates for every phase of your project, including ones to help with resource allocation. Here are a few.
Requirement Gathering Template
Before you can allocate resources, you need to understand what’s required. The free requirement gathering template for Word acts as a means of communication between the stakeholders and the project team. This ensures quality deliverables that meet specifications.

RACI Matrix Template
You’ll also need to organize your resources before you can properly allocate them. Our free RACI matrix template for Excel is a place where you can define the roles and responsibilities of the team members. RACI stands for responsible, accountable, consulted and informed, and the free template helps you place everyone involved in the project within one of those quadrants.

Our free resource planning template for Excel lists all the resources you’ll need for the project, how much each will cost and a monthly, weekly or daily chart of when you’ll need them.

Capacity Planning Template
Leverage this free capacity planning template for Excel to ensure you’re able to meet customer demand. It helps you understand your organization’s resource capacity by outlining the utilization, time and effort for each team member to complete tasks.

Workload Analysis Template
Use this workload analysis template to allocate work hours to employees and calculate their utilization rate and labor costs.

Project Dashboard Template
This free project dashboard template for Excel shows the project progress, costs and workload distribution in various charts and tables.

Resource Allocation Process: How to Allocate Project Resources
Resource allocation is a plan that you develop to make the most of the available resources at your disposal in a project, which makes it a critical resource planning activity. This is mostly a short-term plan set in place to achieve goals in the future.
This sounds challenging, but don’t worry, we’re here to help. The following are some general tips to help you with your resource allocation when managing a project.
1. Define Your Project Scope
Before you can allocate your resources or manage them, you have to determine the scope of the project you’re working on. To do so, you need to break down the project into every individual task and deliverable that will be completed. Once you’ve done so, you can make the right decision on what resources you’ll need and how many of them are necessary to complete the project.
The clearer the project scope is, the better you’ll be able to figure out how to allocate your resources. Take the time to get the full picture of the project using a work breakdown structure or other project planning tools to visualize all your project tasks before estimating your resources.

2. Estimate What Project Resources Will Be Needed
Once you’ve defined your project scope, you can move to the resource planning phase which is when you’ll have to estimate what resources will be needed including people, equipment, materials and anything else you’re going to need to complete your project tasks. Your organization will have some of these resources already, while others will need to be purchased or rented.
Before you can allocate resources, you have to have them. So, make a list using the criteria above and make sure it fits within the project budget .

3. Assess Your Current Resource Utilization & Resource Availability
Now that you’ve determined what resources are required for your project, you should also identify which of those resources are available within your organization. However, some existing resources might be being used for other projects, so it’s important that you not only identify which resources your organization has but also which of those are being utilized.
4. Create a Resource Allocation Plan
Take the information that you’ve gained from the above steps to put together a resource allocation plan. Outline the list of resources you’ll need for your project as well as the cost and quantity of each. When you’re finished, circle back to your project scope to make sure your plan aligns with it.
5. Keep Track of Your Project Resources
It’s a problem when you’re so focused on the process that you neglect to lift your head from the resource allocation plan to note what’s happening. This isn’t merely tracking your estimates against actual progress in the project, though that’s important, too.
You should always be aware of the state of your resources. For example, what’s the schedule for your team, are any taking vacation time, are they sick, etc.? Also, what’s the duration of the lease for the site or equipment? These are important questions to ask when scheduling resources.
Don’t let these details get past you because of tunnel vision. Look at the whole project, not just the various pieces.
6. Use Resource Allocation Reports
You can reallocate if you don’t know where your resources are allocated. You might have planned them out well, but change happens in projects. How can you tell what’s happening on the ground compared to your plans? Project reports .
You can generate all sorts of reports to give you a full picture of the project and how it’s progressing, which helps you balance your resources. For example, resource reports give you an overview of your team’s workload and whether they’re over-tasked or idle.
Task reports keep you updated and variance reports help you determine whether the project is proceeding as planned. The latter gives you vital information, such as if you’re behind schedule and need to redistribute the work to get back on track.
Resource Allocation Example
Let’s say you’re a manager for an IT organization and you’re tasked with hiring an architect for an upcoming project. You know the importance of an architect position to the overall success of the project but you know that they’re usually an expensive hire.
You’ll need to consider if it makes more sense to hire an architect for a specific project or if you want to assign him or her to multiple projects . You can utilize resource allocation tools to determine what makes the most financial sense for your organization.
Resource Allocation Tips
Even though there may be blind spots when managing resources, there are some tips to keep in mind to help you allocate resources as effectively as possible.
1. Know Your Resource Dependencies
By planning beforehand, you can avoid bottlenecks that trap your resources when you need them most in the course of the project execution . Planning also helps you keep your resources from falling short. This doesn’t mean you won’t have a bottleneck or resource shortage, but it’s less likely if you know your resource dependencies.
Part of planning for dependencies is having a contingency plan in place in case team members are blocked or you run low on needed resources. Keep your plans from being over-dependent on one resource to avoid trouble down the line.
2. Track Time
You always want to keep a close eye on the time, how your team is working and if they’re being efficient. It’s your job to make sure that a task that can be completed in a day doesn’t take a week. There are ways to improve time tracking .
To do this, you must keep track of your team’s workload. That requires the right tools to give you real-time data collected on one page where you can see and schedule ahead when needed.
3. Use Resource Allocation Tools
Project management software like ProjectManager is a great asset for managing your resources more productively. With an online tool, you get project data instantly updated.
You can see where your resources are allocated across a calendar that’s color-coded to note whether they’re on- or off-task, on vacation or sick. Rescheduling to help a team member who is overtasked is a simple click of the keyboard.
How to Allocate Resources With ProjectManager
ProjectManager is robust project management software with multiple tools that allow project managers to allocate project resources, track utilization and availability, control costs and deliver project success. Regardless of how you prefer to manage and schedule your resources, ProjectManager has the tools to help you every step of the way. Here are some of our most popular resource management features.
Schedule Resources With Multiple Planning Tools
Tools such as Gantt charts, kanban boards, task lists and project calendars allow you to allocate resources in multiple ways. Use online Gantt charts to create interactive project timelines that let you easily assign the needed resources for each project task or create task lists that make it easy to stay on track. In addition, ProjectManager’s workload charts help you plan and oversee each team member’s workload at a glance so you can keep your team working at capacity.

Track Costs With Project Dashboards & Timesheets
Once you’ve allocated your project resources, you’ll need to track their costs to ensure that you’re sticking to your budget. ProjectManager’s real-time dashboards make it easy to monitor costs, timelines and progress so nothing is overlooked. Use the dashboard to make timely updates and catch problems before they snowball. In addition, you can use our project timesheets to help you keep track of labor costs.

Related Content
If you’re still interested in resource management, you’ve come to the right place. ProjectManager isn’t just superior software, it’s the online hub for all things project management. You not only get free templates but regular blog posts, thorough eBooks, whitepapers and more. Here’s a sample of that content as related to our topic.
- Best Resource Management Software Rankings
- Resource Management: Process, Tools & Techniques
- Resource Planning: The Ultimate Guide
- Resource Smoothing Steps, Templates and Tools
- Resource Forecasting in Project Management
- How to Track Resource Availability
If you’re looking for a project management tool that can help you implement those tips and manage your resources properly, then look no further. ProjectManager has all the features mentioned above to help you manage your resources, and it’s online software, which means the information you’re working with is in real time. See how it can help you by taking this free 30-day trial today!

Deliver your projects on time and on budget
Start planning your projects.

Research project planning with the right resources
In the last blog post , I introduced a series of posts that deal with project planning in the research context. This post thus forms part of a larger set of posts and should ideally be read in conjunction with them. This is the second post of the series, and in the first post, I wrote about the vision and objectives of your research project. It is important that this conceptual step is not skipped in a research project, otherwise, you will be on your way to nowhere slowly.
In this post, I will touch on the resources which are needed to successfully see the project through to the end. This is very important to consider in a research project as it often touches on the feasibility of the project. Without the necessary resources, you are unlikely to finish your project in good time or at all. These may come in a number of different forms, but the 6 which were highlighted by Dr Rob Drennan, whose workshop I draw these insights from were: (1) people, (2) money, (3) equipment, (4) utilities, (5) consumables, and (6) space. Let’s look at each of these in turn.
As a researcher, ‘people’ includes you! To know what type of human capacity you will need to complete your project, you need to go back to your vision and objectives, so if you haven’t done that part, you won’t be able to move forward. What types of methods have you proposed? Do you have the skills? Do you need extra human power to carry out the project?
For instance, if you are going to do data collection, will you be able to do it alone or will you need an assistant to help you? Perhaps you are doing research as an outsider and you need someone to accompany you as a translator.
Maybe you have proposed a method that requires you to have a certain skill set, like a complex statistical procedure. Can you up-skill yourself by attending a training course, is it (ethically) possible to outsource this part of the work to someone else, or do you need to bring a co-author onboard who can assist with that part of the analysis?
When thinking about people, you are really thinking of the skill sets and ‘hands-on-deck’ you will need to finish the project. But you would also want to think about the extent to which you can draw on someone else’s time and skills. The restrictions on this would be different if you’re writing a master’s dissertation versus when you’re writing a journal article, as the rules which govern the production of these documents differ.
Unless you have a generous spouse, cousin, or friend, whose gonna help you, you would need money to pay for any assistance you’re going to need on the project – do you have money? Some research projects don’t just require people, they also have other expenses. For instance, if you’re gonna run a large scale survey through SurveyMonkey or a similar platform, do you have money to pay for that? If not, how will you finish your project?
It’s good practice to draw up a project budget at the time of writing the proposal in order to get a sense of what types of resources will be necessary. Another good reason to do this is if you do spot a call for grant applications, you will already have your budget drawn up, know how much money you need, and simply adjust your costs to cover the requirements set out by the funder.
Equipment & Utilities
Equipment and utilities are largely applicable to researchers in the natural sciences who need lab equipment and the items which allow them to perform their experiments. If you as a social sciences researcher and you are doing an experimental design or need special software (such as statistical programmes) to do your analysis, you will need to budget for this as part of your equipment and/or utilities. It is thus important, at the proposal stage, to gather as much information as possible in relation to what carrying out your project will cost you. Collect quotes and make phone calls if you must. The worst outcome would be learning that you need expensive materials too late and not having raised funds for them.
Consumables
Consumables will be present on every project budget. These are items you need to carry out your project, but which do not represent something that is a long-term investment, as they will get used up in the course of the project. These could include office stationery, money for photocopying, and other office supplies. It is often difficult to pinpoint exactly how many consumables you will need, but it’s good to take a guess and prepare for some consumables up front.
Lastly, you would want to think about space. Where will you carry out your work? What type of space do you need? Will you need space to conduct interviews or keep lab equipment? This is an important aspect of your project, specifically if you will be conducting your research away from home or your home institution. Perhaps you will collect data in another country or another city. Maybe you need to write up your work and your institution does not offer dedicated research areas. This would significantly impact your productivity and your ability to finish your project in good time. So think about this ahead of time if you can.

You May Also Like

How to read when time is limited

6 tips to help you get your New Year’s Resolutions back on track

Getting it right with sustainable planning in 2022
Leave a reply cancel reply.
Your email address will not be published. Required fields are marked *
Save my name, email, and website in this browser for the next time I comment.
The 4 Steps of Resource Planning
June 28, 2019 by Bernie Roseke, P.Eng., PMP Leave a Comment

Like a carpenter without a hammer.
Like programmer without a computer.
Like a speaker without a microphone.
Resource planning is an indispensable component of project management. In fact, it’s so important that the Project Management Body of Knowledge (PMBOK Guide) dedicates a full knowledge area to resource management . In order to effectively manage project resources, they must be planned in advance. The primary output of the Project Resource Management knowledge area is a resource management plan.
There are four steps to a strong project resource management .
- Determine required resources
- Acquire resources
- Manage resources
- Control resource usage
Determine Required Resources
The first step in resource planning is to determine the resources required to perform the work.
Generally speaking, there are five types of resources that are required to complete a project:
- Type is the skill set of the person, for example, a carpenter or an engineer.
- Class is the skill level of the person, for example, junior, intermediate, or senior.
- Materials This category includes the components that become part of the finished product. This includes supplies like construction materials, databases for a web application, or handouts for a training course. The finished product must be rigorously analyzed during the resource planning stage to ensure that all of its constituent materials are identified. Often you have to order more than the exact quantity to account for defective product, production methods, manufacturing waste, and so forth.
- Equipment This category includes the tools, equipment, machines, and other items that don’t become part of the finished product but are necessary to produce the product.Tools and equipment are often rented, leased, or obtained from another part of the business, particularly the larger items. In this case, the organizational unit that owns the equipment must be compensated. Rental rates become part of the project estimate and are attributed to the task that requires the equipment.
- Facilities All projects require some sort of facility to perform their work in. Whether just a small office or a large manufacturing plant, this is a major consideration for many projects. Facilities are often rented or leased as well, and the cost is attributed to the project administration, or a dedicated facilities budget if one exists.
- Organizational / Administration resources are the organizational costs that the project must bear. Although outside of the project, these costs include administration, shared resources, and shared facilities. For example, the CEO’s salary must be spread out among all projects.
- Subcontractors and vendors that must be procured to ensure necessary products and services that cannot be produced with internal resources.
- Financing costs can be a major burden on some projects.
- Contingencies are often tracked separately from individual project resources.
- Overtime is often tracked separately and applies to the project team as well as rental equipment via higher rates for greater use.
Employee and resource availability are recorded in a resource calendar. This ranges from a simple listing of employee vacation time to sophisticated tracking software.
The result is a list of resources allocated to each project task. For example, here is a resource list for the task Build Fence:
| 100 – Build Fence | ||
|---|---|---|
| Type | Average Use | Total |
| Jon | 50 hrs @ $75/hr | $3,750 |
| Bob | 30 hrs @ $50/hr | $1,500 |
| Fence Material | Lump Sum | $650 |
| Tools | Lump Sum | $100 |
| TOTAL | $6,000 | |
Acquire Resources

Human resources are usually, but not always, require the most management effort. The project team requirements must be determined and the job descriptions written. These job descriptions are advertised in the appropriate media, resumes (CV’s) are received and interviews are held.
Project equipment must be sourced and contractors procured.
The following items are important components of the resource plan:
- Project management team roles
- Project team roles
- Procurement needs
- Types and sizes of contracts
- Pre-qualification methods
- Contractor selection criteria
- Resource budgets
- Advertising media and methods
- Performance measurement
- Off-specification policies and procedures
Manage Resources
Once the resources are acquired and available to perform the project work, they must be managed to ensure they contribute at their maximum performance level:

- Subcontractors similarly need to know that a strong reference is available after the project is complete. However, they are highly motivated by fair treatment of project changes. Most projects experience changes from their original plans. It’s how these changes are managed that determine the performance level of the project management team.
- Tools and equipment must be returned in a condition that includes normal wear and tear.
- Facilities must be maintained in a condition that includes normal wear and tear, otherwise damage payments could be a significant (and unexpected) part of project costs.
Decision making is one of the primary day to day tasks of project management . How to best allocate resources, how to minimize resource conflicts, and how to resolve resource conflicts. The ability to make strong decisions is foundational to strong project management.
When resource conflicts occur, problem solving becomes a major part of a project manager’s duties. There are six steps to effective problem solving:
- Identify the problem
- Define the problem
- Investigate
- Check the Solution
Control Resource Usage
During resource planning, the methods for monitoring and controlling the resources to ensure they are delivering the required results are determined.
This involves calculating the utilization rate, which measures how efficiently the resources are being used. The utilization rate is calculated by taking the number of billable hours divided by the total working hours. For example, if a piece of construction equipment was working for 24 hours out of a total 40 hours, the utilization rate would be:
Utilization Rate = 24 / 40 = 60%
Generally, absence hours such as holidays, sick time, or leave are not included in the utilization rate, but the exact implementation of the method is open to whatever is most useful for you.
When resource utilization is too low , or corrective actions are required, a cost benefit analysis provides the basis for project changes.
Resource Planning in the PMBOK
In the Project Management Body of Knowledge (PMBOK) the process Plan Resource Management is the first out of six within the Project Resource Management knowledge area. As you might expect, it is located within the planning process group.
PMBOK, 6th Edition, Section 9.1, “Plan Resource Management”
Plan Resource Management is the process of defining how to estimate, acquire, manage, and use team and physical resources. The key benefit of this process is that it establishes the approach and level of management effort needed for managing project resources based on the type and complexity of the project.
Related posts:

About Bernie Roseke, P.Eng., PMP
Bernie Roseke, P.Eng., PMP, is the president of Roseke Engineering . As a bridge engineer and project manager, he manages projects ranging from small, local bridges to multi-million dollar projects. He is also the technical brains behind ProjectEngineer , the online project management system for engineers. He is a licensed professional engineer, certified project manager, and six sigma black belt. He lives in Lethbridge, Alberta, Canada, with his wife and two kids.
Leave a Reply Cancel reply
Your email address will not be published. Required fields are marked *

- Project Initiation
- Project Planning
- Project Execution
- Monitoring and Controlling
- Project Closure
- Project Management Tutorial
- Project Scheduling Tutorial
- Earned Value Tutorial
- PMP Exam Tutorial
- Find Talent
- PRINCE2 Foundation
- PRINCE2 Practitioner
- PRINCE2 Professional
- IPMA Level A
- IPMA Level B
- IPMA Level C
- IPMA Level D
- Learning Videos
Certification
Recent posts.
- PMI Project Knowledge Areas, Intro
- PMI Project Knowledge Areas, Video 1: Project Integration
- Project Risk Checklist
- Creating a Risk Register
- 50 SMART Goals
- Reporting Earned Value
- Analogous Estimating
- Variance at Completion (Earned Value Analysis)
- TCPI (Earned Value Analysis)
FIND IT HERE
Subscibe to ProjectEngineer.NET channel – YouTube
- WordPress.org
- Documentation
- Support Forums
- Skip to primary navigation
- Skip to content
Understanding Resource Allocation Efficiency
- November 6, 2023

In today’s competitive business environment, organizations constantly strive to optimize their resource allocation . Efficient resource allocation is essential for achieving organizational goals, improving operational performance, and driving sustainable growth. This article aims to provide a comprehensive understanding of resource allocation efficiency, its importance, key principles, management’s role, metrics for measurement, challenges faced, and future trends.

Defining Resource Allocation
Resource allocation refers to the process of distributing available resources in an optimal manner to achieve desired outcomes. These resources can include human capital, financial assets, technology, equipment, and time. Effective resource allocation ensures that resources are used wisely , maximizing their impact and minimizing waste.
Let’s delve deeper into the concept of resource allocation and explore its various aspects.
The Importance of Efficient Resource Allocation
Efficient resource allocation is the cornerstone of organizational success. When resources are allocated effectively , companies can optimize productivity, reduce costs, and enhance overall performance. It enables organizations to focus on core objectives, make informed decisions, and adapt to changing market dynamics.
Imagine a scenario where a company has limited financial resources. By allocating these resources efficiently, the company can invest in key areas that will yield the highest returns. This could involve hiring skilled employees, upgrading technology, or improving production processes. Such strategic resource allocation not only boosts productivity but also helps the company stay competitive in the market.
Key Principles of Resource Allocation
Efficient resource allocation is guided by several key principles:, alignment with strategic objectives.
Resources should be allocated in alignment with the organization’s overall strategic goals and priorities. This means that resources should be directed towards activities that directly contribute to the achievement of these goals. For example, if a company’s strategic objective is to expand into new markets, resource allocation should prioritize marketing and sales initiatives in those markets.
Flexibility
Resource allocation should be adaptable to changes in the business environment, enabling organizations to make timely adjustments. In today’s fast-paced and dynamic market, businesses need to be agile in their resource allocation strategies. This involves regularly evaluating the allocation of resources and reallocating them as needed to capitalize on emerging opportunities or mitigate risks.
Data-driven Decision Making
Effective resource allocation requires accurate and timely data analysis to inform decision-making processes. By leveraging data, organizations can gain insights into resource utilization, identify areas of inefficiency or underutilization, and make data-driven decisions to optimize resource allocation . For instance, data analysis might reveal that a particular department is overstaffed, prompting the reallocation of human capital to other areas of the organization where it is needed more.
Cross-functional Collaboration
Collaboration between different departments and stakeholders is crucial to ensure efficient resource allocation. By involving key stakeholders from various functions, organizations can gain diverse perspectives and insights that can lead to more effective resource allocation decisions. For example, when allocating financial resources, collaboration between finance, marketing, and operations teams can help ensure that the allocation is aligned with the needs and goals of each department.
By adhering to these key principles, organizations can optimize their resource allocation strategies and achieve better outcomes. Efficient resource allocation is not a one-time task but an ongoing process that requires continuous evaluation, adjustment, and collaboration.
In conclusion, resource allocation plays a vital role in organizational success. It involves distributing available resources in an optimal manner to maximize their impact and minimize waste. By aligning resource allocation with strategic objectives, being flexible, making data-driven decisions, and fostering cross-functional collaboration, organizations can enhance their performance and stay competitive in today’s dynamic business landscape.
The Role of Management in Resource Allocation
Management plays a vital role in resource allocation, as it involves decision-making, strategic planning, and execution. Effective management ensures that resources are allocated in line with organizational goals and objectives, fostering productivity and efficiency.
Resource allocation is a complex process that requires careful consideration of various factors. It is not simply about distributing resources, but rather about making informed decisions that will maximize their impact. This involves assessing the available resources, understanding the needs of different projects or tasks, and evaluating the potential returns on investment.
Decision-Making in Resource Allocation
Resource allocation decisions are strategic in nature and involve choosing the most appropriate allocation options based on available resources and anticipated outcomes. Decision-making in resource allocation should consider factors such as resource availability, project importance, risk assessment, and potential returns on investment.
When making resource allocation decisions, managers need to consider the overall objectives of the organization. They must assess which projects or tasks align with these objectives and allocate resources accordingly. This requires a deep understanding of the organization’s priorities and the ability to prioritize projects based on their importance and urgency.
Furthermore, managers must also consider the potential risks associated with resource allocation decisions. They need to assess the likelihood of success for each project or task and weigh it against the potential impact on the organization. This requires a careful evaluation of the available resources and a realistic assessment of the expected outcomes.
Strategies for Effective Resource Management
To effectively manage resources, organizations can employ various strategies:
- Prioritization: Prioritize resource allocation based on the importance and urgency of projects or tasks. This ensures that resources are allocated to the most critical areas, maximizing their impact on the organization.
- Optimization: Optimize resource allocation by identifying areas for improvement, minimizing waste, and eliminating bottlenecks. This involves analyzing the resource allocation process and identifying inefficiencies that can be addressed to improve overall effectiveness.
- Monitoring and Evaluation: Continuously monitor and evaluate resource allocation to ensure its alignment with objectives and make necessary adjustments. This requires regular assessment of the outcomes of resource allocation decisions and the ability to adapt and make changes as needed.
- Delegation and Empowerment: Delegate responsibilities and empower individuals or teams to make resource allocation decisions within defined parameters. This not only distributes the decision-making process but also allows for a more agile and responsive approach to resource allocation.
By implementing these strategies, organizations can enhance their resource allocation processes and ensure that resources are allocated in a way that maximizes productivity, efficiency, and overall organizational success.
Metrics for Measuring Resource Allocation Efficiency
Measuring resource allocation efficiency is essential to assess the effectiveness of resource management strategies and identify areas for improvement. Organizations can utilize quantitative and qualitative metrics to evaluate resource allocation efficiency.
Resource allocation efficiency is a critical aspect of any organization’s success. It ensures that resources are utilized optimally, resulting in improved productivity, cost-effectiveness, and overall performance. To measure resource allocation efficiency, organizations rely on a combination of quantitative and qualitative metrics.
Quantitative Metrics for Efficiency

Quantitative metrics provide objective data for assessing resource allocation efficiency. These metrics are based on numerical values and help organizations gauge the effectiveness of their resource allocation strategies. By analyzing these metrics, organizations can identify areas of improvement and make data-driven decisions.
Financial ratios are one of the most commonly used quantitative metrics for measuring resource allocation efficiency. These ratios, such as return on investment (ROI) and cost per unit, provide insights into the financial performance of resource allocation strategies. By comparing the costs incurred with the outcomes achieved, organizations can determine if their resource allocation is yielding desirable results.
Project timelines are another important quantitative metric. By tracking the time taken to complete projects and comparing it to the allocated resources, organizations can assess the efficiency of their resource allocation. Timely project completion indicates effective resource utilization, while delays may indicate inefficiencies that need to be addressed.
Resource utilization rates are also key quantitative metrics. These rates measure the extent to which resources are being utilized. High utilization rates indicate efficient allocation, while low rates may suggest underutilization or misallocation of resources. By monitoring and analyzing these rates, organizations can identify areas where resources are not being optimally utilized and take corrective actions.
Qualitative Metrics for Efficiency
While quantitative metrics provide valuable insights, they do not capture the complete picture of resource allocation efficiency. Qualitative metrics, on the other hand, provide subjective insights into the effectiveness of resource allocation strategies.
Employee satisfaction is a crucial qualitative metric for measuring resource allocation efficiency. Satisfied employees are more likely to be productive and engaged, indicating that resources are being allocated effectively to support their work. Regular employee feedback surveys can help organizations gauge employee satisfaction levels and identify any issues related to resource allocation that need to be addressed.
Customer feedback is another important qualitative metric. By collecting feedback from customers, organizations can assess how well their resources are meeting customer needs and expectations. Positive feedback suggests that resources are being allocated effectively to deliver value to customers, while negative feedback may indicate areas where resource allocation can be improved to enhance customer satisfaction.
Process improvement and innovation are qualitative metrics that reflect the effectiveness of resource allocation strategies. Organizations that allocate resources efficiently are more likely to have streamlined processes and foster a culture of innovation. By encouraging knowledge sharing and providing resources where they are most needed, organizations can drive continuous improvement and innovation.
In conclusion, measuring resource allocation efficiency requires a combination of quantitative and qualitative metrics. While quantitative metrics provide objective data, qualitative metrics offer subjective insights into the effectiveness of resource allocation strategies. By analyzing these metrics, organizations can identify areas for improvement and make informed decisions to optimize their resource allocation.
Challenges in Resource Allocation
Despite its importance, resource allocation can be challenging for organizations. It involves balancing multiple priorities, managing limited resources, and navigating complex decision-making processes.
Resource allocation is a critical aspect of organizational management. It determines how resources, such as time, money, and manpower, are distributed among different projects, departments, or initiatives. Effective resource allocation ensures that resources are utilized optimally, maximizing productivity and achieving strategic objectives.
However, there are several challenges that organizations commonly face when it comes to resource allocation.
Common Obstacles in Efficient Resource Allocation
Some common obstacles that organizations face in resource allocation include:
- Uncertainty and Lack of Visibility: Unclear demand forecasts and lack of visibility into resource availability can hinder efficient allocation. Organizations may struggle to accurately predict future resource needs, leading to overallocation or underutilization of resources.
- Competing Stakeholder Interests: Different stakeholders may have conflicting priorities, making it challenging to allocate resources fairly. Balancing the needs and expectations of various stakeholders, such as project managers, department heads, and executives, requires careful negotiation and compromise.
- Legacy Systems and Processes: Outdated systems and processes can limit organizations’ ability to allocate resources optimally. Manual resource allocation methods, spreadsheets, and outdated software may result in inefficiencies, errors, and delays.
- Resistance to Change: Resistance to change within the organization can impede resource allocation optimization efforts. Employees may be reluctant to adopt new resource allocation practices, fearing job insecurity or disruption to established routines.
Overcoming Resource Allocation Challenges
To overcome resource allocation challenges, organizations can implement various strategies:
- Improved Data Collection and Analysis: Enhance data collection and analysis capabilities to gain better insights into resource allocation needs and opportunities. Organizations can leverage advanced analytics tools and techniques to gather and analyze data on resource utilization, demand patterns, and project requirements.
- Collaborative Decision-Making: Foster collaboration and communication across departments to ensure shared decision-making in resource allocation. By involving key stakeholders in the allocation process, organizations can increase transparency, accountability, and buy-in.
- Investment in Technology: Embrace innovative technologies such as resource management software and automation tools to streamline resource allocation processes. These tools can automate resource tracking, scheduling, and allocation, reducing manual effort and improving accuracy.
- Regular Evaluation and Feedback: Continuously evaluate and seek feedback on resource allocation processes to identify areas for improvement and make necessary adjustments. Organizations can conduct regular reviews, surveys, or feedback sessions to gather insights from employees and stakeholders.
By addressing these challenges and implementing effective resource allocation strategies, organizations can optimize their resource utilization, improve project outcomes, and enhance overall operational efficiency.
Future Trends in Resource Allocation
In the rapidly evolving business landscape, resource allocation is expected to face new challenges and opportunities. Several key trends are shaping the future of resource allocation:
Technological Advances and Resource Allocation
Advancements in technology, such as artificial intelligence (AI) and machine learning, are revolutionizing resource allocation. These technologies can analyze vast amounts of data, identify patterns, and make data-driven recommendations for optimal resource allocation.
For example, AI-powered algorithms can analyze historical data on customer preferences, market trends, and production capabilities to determine the most efficient allocation of resources. By leveraging AI, organizations can make informed decisions that maximize productivity, minimize waste, and enhance overall performance.
Furthermore, machine learning algorithms can continuously learn and adapt based on real-time data, enabling organizations to dynamically adjust their resource allocation strategies in response to changing market conditions.
As technology continues to advance, resource allocation processes will become increasingly automated and efficient, allowing organizations to optimize their operations and stay competitive in the digital age.
The Impact of Globalization on Resource Allocation
Globalization has expanded market opportunities and created new complexities in resource allocation. Organizations must navigate global supply chains, consider cultural and regulatory differences, and adapt to diverse customer needs in their resource allocation strategies.
With the rise of e-commerce and global trade, organizations now have access to a broader customer base and a wider range of suppliers. However, this also means that resource allocation decisions must take into account factors such as shipping costs, import/export regulations, and cultural preferences.
For example, a multinational company operating in multiple countries may need to allocate resources differently in each market to accommodate local preferences and regulations. This could involve adjusting product offerings, distribution channels, or marketing strategies to effectively serve diverse customer needs.
Additionally, globalization has increased competition, requiring organizations to optimize their resource allocation to gain a competitive edge. By strategically allocating resources to areas with the highest growth potential or the greatest demand, organizations can position themselves for success in the global marketplace.
Efficient resource allocation continues to be a critical factor in the success of organizations across industries. By understanding the principles, challenges, and future trends in resource allocation, businesses can optimize their allocation strategies, drive efficiency, and achieve sustainable growth.
Table of Contents
Project tools your team will stick with..
Chat • Projects • Docs
Related Posts
Ultimate Speaker Guide for Online Events Template
Streamline Your Sales Pipeline Project with This Template
The Ultimate Customer Feedback Tracking Template
The future of team collaboration.
Teamhub is made for your entire organization. Collaborate across departments and teams.
Privacy first
Create private projects or docs inside public Hubs. The structure of every Hub can be as unique as your organization.
Advanced Dashboard
Get a high level view of everything in your team, department and organization
Guest Accounts
Invite your clients and contractors and collaborate on projects together.
Custom Views
See your tasks and work the way you prefer. Create views custom to your team.
Use pre-made project templates to save time and get you started.
Time-off Coming soon
Powerful time-off management capabilities. Employee directories, attachments, leave management and onboarding.
Development
Human resources, what makes us great.
The magic that sets us apart from everyone else
A single price
One price for access to all our apps. Save a ton in SaaS costs.

Time-off built right in
Assign tasks and be alerted right away if team members are away.

Powerful Workflow engine
Map out your business processes. Take the thinking out of flows.
Private Hubs
Your personal space, visible only to those you invite in.

Custom Hierarchy
Organize each hub or folders to your own preference.
Smart automations
Set up triggers for dozens of different actions and reduce manual effort.
Adding {{itemName}} to cart
Added {{itemName}} to cart
Get instant access to detailed competitive research, SWOT analysis, buyer personas, growth opportunities and more for any product or business at the push of a button, so that you can focus more on strategy and execution.
Table of contents, the benefits of resource scheduling in project management.
- 4 May, 2024

Importance of Resource Scheduling
Efficient resource scheduling plays a vital role in the success of any project. It involves identifying when project resources are needed and allocating them appropriately to ensure timely and within-budget project completion. By effectively managing resources, project managers can avoid over or under-allocation, leading to smoother project execution and improved outcomes.
Impact on Project Success
Poor resource scheduling can have significant implications for project success. When resources are not properly allocated, delays in individual tasks can occur, causing a domino effect that ultimately delays the entire project. This delay can result in additional project costs and potential compromises in project scope or deliverable quality to save time ( ProjectManager.com ). On the other hand, effective resource scheduling ensures that the required resources are available when needed, minimizing delays and keeping the project on track.
Key Planning Areas
Resource scheduling directly affects several key project planning areas, including time, scope, cost, risk, quality, and resources. Each of these areas is interconnected and relies on efficient resource management to achieve project objectives. Here’s a brief overview of how resource scheduling impacts these planning areas:
- Time: Resource scheduling ensures that resources are allocated appropriately, helping to prevent delays and keeping the project on schedule.
- Scope: Proper resource allocation assists in managing project scope by ensuring that the necessary resources are available to complete the defined project scope.
- Cost: Resource scheduling helps control project costs by avoiding over-allocation or under-utilization of resources, thereby optimizing resource usage.
- Risk: Effective resource scheduling helps mitigate risks by ensuring that the right resources are allocated to critical tasks, reducing the likelihood of issues arising.
- Quality: By allocating resources based on their skills and expertise, resource scheduling contributes to maintaining the quality of deliverables and meeting project requirements.
- Resources: Resource scheduling ensures that resources such as raw materials, human resources, and machinery are available as needed, preventing bottlenecks and shortages.
By managing these planning areas efficiently through resource scheduling, project managers can enhance project performance, maintain stakeholder satisfaction, and achieve successful project outcomes.
To effectively implement resource scheduling, project managers can utilize various project scheduling tools and techniques for resource allocation. These tools and techniques aid in planning and organizing resources, ensuring optimal utilization throughout the project lifecycle. By following best practices for resource management, such as identifying resource needs and allocating resources wisely, project managers can navigate the challenges associated with resource scheduling and maximize project success.
Resource scheduling is a critical aspect of project management, and its significance cannot be understated. By recognizing its impact on project success and understanding its role in key planning areas, project managers can prioritize resource scheduling and ensure efficient resource utilization throughout the project lifecycle.
Approaches to Resource Scheduling
Resource scheduling plays a crucial role in project management resource planning . It involves effectively managing and allocating project resources to ensure timely and efficient project completion. Two main approaches followed by project managers for scheduling resources are time-constrained scheduling and resource-constrained scheduling, each with its own considerations and benefits.
Time-Constrained Scheduling
Time-constrained scheduling is an approach that places a higher priority on meeting project deadlines. In this approach, the project manager sets specific project timelines and deadlines, and the resources are allocated based on these predetermined timeframes. The focus is on completing the project within the given time constraints.
With time-constrained scheduling, the project manager typically has less flexibility in resource allocation. Resources may need to be adjusted or reallocated to meet the predetermined project timeline. This approach requires careful planning and coordination to ensure that the necessary resources are available when needed.
Resource-Constrained Scheduling
Resource-constrained scheduling, on the other hand, focuses on distributing available resources evenly throughout the project. In this approach, the project manager considers the availability and capacity of resources before allocating them to specific tasks. The goal is to optimize resource utilization and avoid over or under allocation.
Resource-constrained scheduling takes into account factors such as the availability of human personnel, equipment, materials, and finances. It involves balancing the workload and resource capacity to ensure that resources are not overwhelmed or underutilized. This approach requires effective resource management and coordination to achieve efficient project execution.
The choice between time-constrained scheduling and resource-constrained scheduling depends on various factors, including project requirements, resource availability, and the project manager’s priorities. It is essential to assess the project’s specific needs and constraints to determine the most suitable approach for resource scheduling.
By adopting the appropriate approach, project managers can maximize the utilization of available resources, meet project deadlines, and ensure the successful completion of projects. Efficient resource scheduling is crucial for effective project resource management and plays a significant role in the overall success of a project.
Tools for Effective Resource Scheduling
To ensure efficient resource scheduling in project management , it is crucial to utilize appropriate tools and techniques that facilitate effective planning and allocation of resources.
Project Scheduling Tools
Utilizing project scheduling tools is essential for effective resource scheduling. These tools provide a centralized platform for managing and tracking resources, tasks, and timelines. With these tools, resource managers can gain a comprehensive view of resource availability, allocate resources to specific tasks, and monitor project progress in real-time.
One notable example of project scheduling tools is ProjectManager. This resource management software offers features that streamline resource scheduling, including detailed team availability, management of global holidays, and resource utilization tracking ( ProjectManager ). These tools enable resource managers to create task lists, import data from spreadsheets, and make informed decisions based on real-time project data.
Techniques for Allocation
In addition to project scheduling tools, employing effective techniques for resource allocation is crucial in resource scheduling. These techniques ensure that resources are allocated optimally, considering factors such as skill sets, availability, and project requirements.
One common challenge faced by resource managers is understanding the overall workload for each employee, which can lead to inefficiencies and additional costs ( eResource Scheduler ). To overcome this, it is important to have a clear understanding of resource capacity and utilize resources at around 70-80% of their maximum capacity. This allows for optimal productivity while avoiding burnout and resource overload.
Implementing resource allocation techniques that optimize productivity and reduce costs can have significant benefits. For example, one customer reported a 90% increase in efficiency by utilizing resource schedules, reducing time spent waiting for instructions and dedicating more time to actual work ( Float ). By utilizing these techniques, resource managers can ensure that resources are effectively allocated, leading to improved project outcomes.
By leveraging project scheduling tools and employing effective resource allocation techniques, resource managers can streamline the resource scheduling process, optimize productivity, and achieve project success. These tools and techniques provide the necessary support for efficient allocation and utilization of resources, enabling teams to work collaboratively and meet project goals.
Best Practices for Resource Management
To effectively manage project resources and optimize resource scheduling in project management, it is essential to follow best practices. By identifying resource needs and allocating resources wisely, resource managers can ensure efficient utilization of resources and successful project outcomes.
Identifying Resource Needs
Identifying resource needs is a crucial step in resource management. It involves determining the types and quantities of resources required to complete project tasks within set timeframes and budgets. Resource managers should collaborate closely with project managers and stakeholders to understand project requirements and define resource requirements accordingly.
To identify resource needs, consider the following factors:
- Skills and Expertise : Determine the specific skills and expertise required for each task. This will help in selecting the right personnel who possess the necessary qualifications and experience to complete the work effectively.
- Resource Availability : Assess the availability of resources within the organization or externally. Consider factors like existing workloads, team capacity, and any potential constraints that may impact resource availability.
- Equipment and Materials : Identify the equipment, tools, and materials necessary to carry out project tasks. Ensure that the required resources are procured or reserved in a timely manner to avoid delays.
By accurately identifying resource needs, resource managers can ensure that the right resources are allocated to the right tasks, minimizing the risk of bottlenecks and project delays.
Allocating Wisely
Once resource needs have been identified, the next step is to allocate resources wisely. Resource allocation involves assigning resources to specific tasks and projects based on their availability, skills, and the requirements of each task.
Consider the following strategies for efficient resource allocation:
- Capacity Planning : Evaluate the capacity and workload of each resource to determine their availability for new projects or tasks. Avoid overloading resources with excessive workloads, as this can lead to burnout or compromised quality of work. Utilize resource management tools to gain insights into resource availability and make informed allocation decisions.
- Resource Skills Matrix : Maintain a skills matrix or a RACI chart to track the skills and responsibilities of individual resources. This helps in quickly identifying suitable resources for specific project tasks based on their expertise and availability.
- Collaboration and Communication : Foster effective communication and collaboration between resource managers, project managers, and team members. Regularly review and adjust resource allocations based on changing project requirements or unforeseen circumstances.
By allocating resources wisely, resource managers can optimize resource utilization, improve project efficiency, and ensure that projects are completed on time and within budget.
By implementing these best practices for resource management, resource managers can streamline the resource scheduling process, effectively allocate resources, and ultimately contribute to the success of project outcomes.
Challenges in Resource Scheduling
Resource scheduling in project management comes with its fair share of challenges. Effective management of workload and accurate time estimates are two key areas that resource managers often struggle with.
Workload Management
Understanding and managing the overall workload for each employee, also known as resource capacity, can be a significant challenge. Many companies still rely on manual systems, which can lead to inefficiencies and extra costs. It is important to optimize resource utilization to ensure productivity while avoiding burnout or dissatisfaction ( Teamdeck ).
To overcome this challenge, resource managers should aim to use resources at around 70-80% of their maximum capacity. This allows for optimal productivity while leaving room for unforeseen circumstances and flexibility. By leveraging comprehensive project resource planning software, managers can gain insights into resource capacity, track workloads, and make informed decisions to balance and allocate resources effectively ( eResource Scheduler ).
Time Estimates
Accurate time estimates play a crucial role in resource scheduling. Without proper estimation, it becomes challenging for managers to allocate resources effectively and ensure tasks are completed on time. Inaccurate time estimates can lead to delays, bottlenecks, and frustration among team members.
To improve time estimates, resource managers can leverage project management tools that provide insights into historical data, task dependencies, and team performance. By analyzing past projects and considering various factors that can impact time estimation, managers can make more accurate predictions, allocate resources accordingly, and prevent potential delays ( eResource Scheduler ).
By addressing these challenges in resource scheduling, resource managers can enhance the overall efficiency and productivity of their teams. Leveraging workforce scheduling tools and implementing best practices in workload management and time estimation can help ensure the successful execution of projects and the optimal utilization of resources.
Benefits of Efficient Resource Scheduling
Efficient resource scheduling plays a crucial role in project management resource planning and offers several benefits for resource managers. By effectively allocating and managing resources, organizations can enhance productivity and improve client satisfaction. Let’s explore these benefits in more detail.
Enhanced Productivity
Resource scheduling enhances employee engagement and productivity by ensuring reliable project schedules, matching employees with tasks based on their skills, and maintaining maximum efficiency across all project tasks. By utilizing project resource allocation techniques, resource managers can assign the right resources to the right tasks, optimizing productivity and minimizing downtime.
With efficient resource scheduling, teams have a clear understanding of their upcoming tasks and deadlines, preventing project delays and reducing the time spent waiting for instructions. This leads to improved time management and better utilization of resources. For example, according to Float , one customer increased efficiency by 90% using resource schedules, allowing more time for actual work and reducing hours wasted on waiting.
Improved Client Satisfaction
Resource scheduling contributes to improved client satisfaction by providing real-time updates on project progress and reducing waste of time and resources. By having a clear overview of resource availability and task allocation, resource managers can ensure that projects are on track and meet client expectations.
Efficient resource scheduling helps strengthen client relationships and enhances brand image. Clients appreciate organizations that can deliver projects on time and within budget. By effectively managing resources, organizations can increase profits and maintain high-quality project delivery. As a result, client satisfaction is enhanced, leading to positive reviews, repeat business, and referrals.
In summary, efficient resource scheduling in project resource management offers multiple benefits. It enhances productivity by optimizing resource allocation and reducing downtime, leading to improved project performance. Additionally, it improves client satisfaction by providing real-time updates, reducing waste, and enhancing project delivery. By implementing effective resource scheduling strategies, organizations can streamline their operations, save time, and achieve better project outcomes.
Perform Deep Market Research In Seconds
Automate your competitor analysis and get market insights in moments
Create Your Account To Continue!
Automate your competitor analysis and get deep market insights in moments, stay ahead of your competition. discover new ways to unlock 10x growth., just copy and paste any url to instantly access detailed industry insights, swot analysis, buyer personas, sales prospect profiles, growth opportunities, and more for any product or business..
More From Forbes
14 tips to create an effective strategy for resource planning.
- Share to Facebook
- Share to Twitter
- Share to Linkedin
One of the biggest mistakes new businesses make is failing to properly utilize the resources they have. You can have the right amount of products in place, the right amount of funds to run the business and the best team put together, but if you're mishandling all your resources, everything will eventually fall out of balance and you'll find yourself scrambling to cover deficits.
The only way for business owners to be sure they're getting the most out of their available resources is to gain an understanding of how to effectively utilize them and then make a strategic plan to follow. To help ensure that small businesses are following an effective strategy, 14 professionals from Forbes Business Council weigh in below to share their top tips for starting resource planning.
Members of Forbes Business Council share advice on crafting a strategy for resource planning.
1. Dream Big, But Start Small
Have a big dream but start small. Do an initial check of the capacity and demand of a certain product or service, thus maximizing its benefits before venturing on to other services and expanding. This will provide a realistic view of the outcome and the capacity to commit while learning the operations. It also gives ample time if changes are needed in place. - Lane Kawaoka , SimplePassiveCashflow.com
2. Know How To Value Your Resources
To get the most out of available resources, you first need to know how to value a company's resources in the first place. First of all, key performance indicators (KPIs) have to be defined. Once these have been defined, you can start thinking about a solution or optimization. I have observed that many companies are not even aware of the actual KPI. - Fabian Siegler , Expertiserocks SL
Best Travel Insurance Companies
Best covid-19 travel insurance plans.
Forbes Business Council is the foremost growth and networking organization for business owners and leaders. Do I qualify?
3. Have Defined Goals For Each Resource
Small businesses have limited resources, and it's an unrealistic expectation to believe they will be deployed perfectly. Set goals first. My one tip in the early stages of a business is that every resource deployed must have a defined purpose with a clear goal. A business leader has to clearly understand when to be resourceful and when to deploy resources to push the business strategy forward. - Austin Speck , Titan Brands
4. Optimize The Most Important Resource
One of the most important resources of any business is its employees. Optimizing employees is getting the most out of them while providing a medium for growth. Good employees are constantly evolving and growing over time, taking on more and more responsibilities. Therefore, all businesses need a well-functioning system for employees’ professional growth that, as a result, improves productivity. - Mark Snell , Polestar Plumbing, Heating & Air Conditioning
5. Have An Effective Social Media Strategy
I believe it is important to have an effective social media strategy based on your budget and company's outreach. For example, there is always a way to partner with a nonprofit that is aligned with your company's values. Bridging together and planning a social media campaign around a national holiday together can be an easy way to promote your brand while giving goodwill to others. - Lisa Caprelli , Unicorn Jazz
6. Identify Resources And Needs To Meet Goals
First, identify what resources you have and what you will need to achieve your goals. For every project, evaluate what resources the project needs and the return you expect from the investment, and prioritize accordingly. It’s critical for small businesses to continually evaluate their resource levels and adapt their strategy as needed to ensure they are using their resources effectively. - Matthew Ramirez , Paraphrase Tool
7. Use A Resource Mapping Exercise
Try using a resource mapping exercise. Brainstorm with your team all of your core resources, going through each one of these to make sure you are fully utilizing its capacity. Define what is unique and competitive about each resource, and what can be done to make it even more useful. It can be done as a bulleted list or a graphical diagram map. - James Langabeer , Yellowstone Consulting, LLC
8. Hire People With A Growth Mindset
Resource planning is a lot easier if you hire self-motivated people with a learning and growth mindset that have shown the willingness and ability to challenge themselves and wear multiple hats in the past. Experience is important for the core role you are hiring for, but talent, mindset and a willingness to operate outside of one's comfort zone is a key attribute for success in a small company. - Gabriel Smith , Pricefx
9. Focus On Your Core Competencies
Focus on core competencies, hire for weaknesses and outsource anything that is not a core business activity. For example, we are a PR firm and outsourcing accounting has been a boon to our business—we focus on what we do well and they help us measure our results. - Michelle Lyng , Novitas Communications
10. Do Internal SWOT Analysis Of Resources
A very simple approach would be to do an internal SWOT (strengths, weaknesses, opportunities and threats) analysis of the resources. Look to see how, what or even if they are contributing to the company's mission or are a drag on resources. - Howard Rosen , LifeWIRE Corp
11. Limit Number Of Parallel Tasks Assigned
I recommend limiting multitasking! Multitasking may sound efficient, but it often results in lower overall productivity. Therefore, it is essential to limit the number of parallel tasks assigned at any given time. Doing this will significantly optimize resource utilization. - Bhaskar Ahuja , Originscale Corp
12. Understand Your Company's Capitals
Have a deep understanding of your company's "4C’s" or the four intangible capitals that drive profits and value up—human, structural, customer and social. These drive the entire business forward. Having a deep understanding of them will allow the leader to understand what resources are needed to make them cross-functional or effective and efficient. - Scott Snider , Exit Planning Institute
13. Define Vision, Focus On Pain Points
Define your vision. What does success look like? Identify all pain points that would inhibit achieving the vision and rank these pain points in order of greatest impact. Focus resources on the one with the greatest impact. Then the next. As the pain dissipates, the way becomes clearer and momentum begins to build. List the biggest impacts to build momentum, and focus resources on the greatest "one." Focus is key! - Margo Jay , 365 Integrated
14. Have A Comprehensive Hiring Plan
Having a well-thought-out hiring plan is so important. A bloated business can lead to challenges in communication with your team and your customers. If you really must hire, only do so when your resources are above and beyond what your organization needs to succeed. Funny enough though, we've actually seen the best results when working lean. - Ted Dhillon , FigBytes

- Editorial Standards
- Reprints & Permissions
| is an online business magazine covering Business Strategies, Business Theories, & Business Stories. |
4 Effective Ways to Manage Resources More Efficiently
What is resource management.

All organizations have finite, limited resources. Therefore, effective managers who are able to make the best strategic decisions around resource allocation to maximize the productivity of the organization’s resources will outcompete their competition–even those competitors with greater pools of resources at hand.
It is also important to differentiate between key, critical resources and non-critical resources. In fact, the pioneer of Disruptive Innovation, Clayton Christensen, defines “Key Resources” as one of the 4 core components of a successful business model –with the other components being the Customer Value Proposition, Profit Formula, and Key Processes (see PowerPoint slide below).
These resources are essential for delivering the Customer Value Proposition and ensuring the business operates efficiently and effectively.
Key Resources are the assets that are crucial for creating value for the customer. These resources enable the business to deliver its value proposition, maintain relationships with customer segments, and earn revenue. They are integral to the business’s capability to execute its strategy and achieve its goals.
Let’s delve deeper into the 7 types of key resources, as defined by Christensen, and their importance.
Types of Key Resources
- People: Human resources are the backbone of any organization. This includes the talent, skills, and expertise of the employees. People are critical for innovation, problem-solving, and delivering high-quality services or products.
- Technology: Technological resources include software, hardware, and other digital tools that facilitate business operations. Advanced technology can provide a competitive edge by improving efficiency, enabling innovation, and enhancing customer experiences.
- Equipment: Physical resources such as machinery, tools, and facilities are essential for the production and delivery of goods and services. The quality and reliability of equipment directly impact the business’s operational efficiency.
- Information: Data and knowledge are invaluable resources. Access to accurate and timely information helps in decision-making, understanding market trends, and responding to customer needs effectively.
- Channels: Distribution channels, whether physical or digital, are critical for reaching customers. Effective management of these channels ensures that products and services are delivered efficiently and meet customer expectations.
- Partnerships and Alliances: Strategic partnerships and alliances can enhance a business’s capabilities. These relationships can provide access to new markets, technologies, or expertise that the business may not possess internally.
- Brand: A strong brand is a powerful asset. It represents the business’s reputation and can significantly influence customer loyalty and trust. Investing in brand development can differentiate a business from its competitors.
You learn more about Clayton Christensen’s thought leadership on Business Model Innovation (BMI) here.
How to Manage Resources
All workplaces are an integration of numerous departments working together as one to ensure the business runs smoothly. Almost every sector is reliant on other departments and cannot function at its full potential without the rest putting in their best as well. One reason why companies end up compromising their profits is due to the inefficient use of the resources at hand.
Through efficient utilization of resources, businesses can reach new heights of success. On the other hand, inefficient utilization will lead to bigger losses. You will not be able to get any value out of your investments unless you know how to make the most out of them.
The tips mentioned below on how to manage resources will do wonders for your corporation if implemented in the correct manner.
1. Plan to Plan
Planning is important when it comes to being efficient. Time is money and it is best to plan for effective resource management from the very beginning of projects. When starting a project, planning should be first on your to-do list. It is via planning that you will be able to fully gauge the types and amount of resources you will be requiring. Many projects fail because businesses end up investing in too many or too few resources.
After figuring out what you will need, you can then plan their use by dividing the project up into stages.
- Identify resources that are needed for completion of the project. Add to the list any resources you will be requiring, whether it is in the first stage of completion or the last.
- Analyze and put up an estimate of the time each resource needs and its role in completion of a particular task.
- Go through the outline of the entire project and ensure that no resource is left out.
- Finalize the list of resources and their details before the project can officially begin. It is essential to have the list ready for everyone to see so that the details are clear in everyone’s minds and the risks of confusion are reduced.
2. Take a Systematic Approach
One of the most effective ways of using resources and minimizing their use at work when possible is by adopting a systematic approach. This can be achieved by:
- Setting a baseline – Using your previous performance as a base for improvement will help pave the path for productivity.
- Benchmarking your performance – Comparing your own performance against that of similar companies (preferably your competitors).
- Forming an action strategy – Once the prospective improvements have been highlighted, it is time to form an action scheme about how to accomplish them.
- Fixing targets and responsibilities – While setting targets ensure that they are achievable in the allocated time by the employees.
- Observing and reporting – Set up reporting procedures and measure your performance at regular intervals to ensure that you are on track.
- Reviewing actions and performance – This step will ensure that you keep learning and improving.
3. Use Technology Where Possible
The use of technology goes a long way in speeding and easing up processes significantly. Any feature of the project that can be completed using technology should be automated. This will in turn minimize the risk of mistakes occurring and free up manpower that can then be reallocated to other projects.
Using technology ensures efficient allocation of resources. There is less wastage and more effective usage of resources. Technology will show you exactly what’s needed so you use specific resources, leaving others free to be utilized for the completion of other projects.
The implementation of automated procedures will revolutionize the running of projects and provide a more streamlined approach to resource planning and management. Any automated processes must be initially tried and tested to ensure that there are no glitches, as slip-ups will add a heavy cost down the road.
The balance between technology and business resource management is a key part of business development. The use of technology will make the running of the company much more efficient and allow several projects to run at the same time due to the resources that free up when technology is used instead of the assets.
4. Use Resource Management Software
Resource management software is a useful tool to significantly enhance the operations of your business. Invest in resource management software that offers a long list of features tailored to boost the management of resources and improve the overall performance and productivity. One popular example is the Timewax resource software which allows managers to share the resource planning with their employees via the company’s calendar system or mobile application. The following are some of the features you should look for in the software you are investing in.
Scheduling the Projects
Efficient time management includes adding every little task to your schedule. Create a schedule if you don’t want to be nagged by the problems you face. If the project has a long deadline, then adding a rough outline of the task until you can add to it in detail will help plan resources and steps out accordingly and more competently.
Generating a Work Schedule
Resourceful allocation includes assigning employees to projects and tasks within those projects. Operational schedules should be implemented for the upcoming stages of the project. Projects that run longer than two weeks must be broken down into parts and resources must be assigned and allocated accordingly.
Producing a Weekly Schedule
Organizing work on a weekly basis allows companies to set a clear cut off point. A new schedule is created at the end of every week using employees that can then perform their tasks and be ready beforehand. Scheduling on a daily basis is also feasible, especially for those companies that have to deal with technical breakdowns that appear without any prior notice.
Resource management software makes use of a convenient planning board to give clients instant overview of all the ventures and resources. The planning board has features like multiple views, time scale, resource requests and alerts, and emails that set it aside from other resource management tools.
Resource management can be a real hassle if not done properly. The drawbacks of an insufficient resource management system include failure to utilize the potential of your existing resources, making the entire organization suffer.
Inadequate resource management will lead to resources being under-utilized or over exhausted. It can also result in wastage of assets that could have been utilized to generate revenues if a proper management system was implemented.
These tips, if implemented properly will go a long way in assisting companies in revolutionizing their resource management and utilization. Focus on the importance of planning and invest in smarter resource management software.
Bonus Tip: Utilize the Balanced Scorecard (or Similar Performance Management Methodology)
The Balanced Scorecard (BSC) is a strategy performance management tool —a semi-standard structured report, supported by proven design methods and automation tools, that can be used by managers to keep track of the execution of activities by the staff within their control and to monitor the consequences arising from these actions. The BSC methodology was developed by Robert Kaplan and David Norton.
BSC relies on 4 key management processes to tie short-term activities with long-term objectives:
- Translating the Vision
- Communication and Linking
- Business Planning
- Feedback and Learning
Let’s dig deeper into the 3rd management process, Business Planning. Most organizations have separate processes for Strategic Planning , Resource Allocation, and Budgeting. This third process enables companies to integrate their business and financial plans
A separate Resource Allocation and Budgeting process run by Finance sets financial numbers that generally bear little relation to the targets in the strategic plan. When implementing the Balanced Scorecard’s measures as the basis for Resource Allocation and priority setting, management can undertake and coordinate only those initiatives that the company toward its long-term strategic objectives. This ensures the allocation and management of resources is efficient, as resources ties directly to driving the business towards its organizational goals and strategic objectives.
To familiarize yourself with other Performance Management frameworks, take a look at these materials available on Flevy (and those listed at the end of this article):
- Performance Management Toolkit
- Performance Management Frameworks
- Performance Management Stream
Caveat: Key Resources vs. Disruptive Innovations
As aforementioned, Clayton Christensen defined key resources as the critical assets and capabilities that a company possesses to maintain its competitive advantage in a given market. These resources are often essential for the company’s current success and play a significant role in serving existing customers and meeting their needs.
However, the very same key resources that contribute to a company’s success can also be a liability when facing “ Disruptive Innovations .” Disruptive Innovations often emerge from new technologies or approaches that initially target underserved or overlooked customer segments. These innovations may not require the same level of sophistication or features as the existing solutions, which means they do not rely on the same key resources.
The dilemma arises when established companies focus too much on protecting and optimizing their existing key resources to serve their current customers better. In doing so, they may miss out on the potential of disruptive innovations that target emerging markets or new customer segments. Eventually, these Disruptive Innovations can surpass the established incumbent organizations, leading to their decline or even failure.
According to Christensen, it is essential for organizations to be aware of the distinction between sustaining innovations that build on existing key resources and Disruptive Innovations that often require new and different resources. To address this dilemma, organizations may need to explore separate units or divisions that can focus on disruptive opportunities without being constrained by existing key resources and processes.

Want to Achieve Excellence in Performance Management?
Readers of this article are interested in these resources.


About Shane Avron
Top 10 recommended documents on performance management.

| | Many companies develop robust strategies, but struggle with operationalizing their strategies into implementable steps. This presentation from flevy introduces 12 powerful business frameworks spanning both Strategy Development and Strategy Execution. | This 48-page whitepaper, authored by consultancy , provides the frameworks, tools, and insights needed to manage serious Change—under the backdrop of the business lifecycle. These lifecycle stages are each marked by distinct attributes, challenges, and behaviors. | ||
| We've developed a very comprehensive collection of Strategy & Transformation PowerPoint templates for you to use in your own business presentations, spanning topics from Growth Strategy to Brand Development to Innovation to Customer Experience to Strategic Management. | We have compiled a collection of 10 Lean Six Sigma templates (Excel) and Operational Excellence guides (PowerPoint) by a multitude of LSS experts. These tools cover topics including 8 Disciplines (8D), 5 Why's, 7 Wastes, Value Stream Mapping (VSM), and DMAIC. |
|
|
|
|
|
|
|
| ( ) is a leading source of information on business strategies, business theories, and business stories. Most of our articles are authored by management consultants and industry executives with over 20 years of experience. |
|
| · · · · · · · / / / Contact Us: | | | | |
The Top 101 Consulting Frameworks
Get our free guide..

No thanks, this isn't something I need right now.

- Twitter icon
- Facebook icon
- LinkedIn icon
Resource allocation 101: How to manage your team’s resources

10 ways to stay calm under pressure (at work and in life)

How to create a project implementation plan

What are limiting beliefs? How to overcome them and succeed
Working with planio, see how our customers use planio.
- Partner Program
- Partner Login
- Feature Overview
- Project Management
- Professional Services Automation (PSA)
- By Company Role
- By Industry
- Business & Economic Impact
PRODUCT SUPPORT
- Pricing Plans
- Success Plans
- Resource Utilization and 5 Ways to Maximize it within your Organization
- January 25, 2022

What’s a business without resources? Not much. But, having access to resources isn’t a direct ticket to attaining your business goals. The secret lies in allocating and utilizing these resources in the most efficient way to bring maximum value to the business. We understand that resource utilization and allocation may not always be your strongest suit—it’s not for most businesses.
However, to reach your goals and have a competitive edge in your market, you must learn how to improve resource allocation and utilization rates for your business.
To help you get started, we’ve put together the key information you need including:
- What resource allocation and utilization are,
- How the two impact your business,
- Best practices to improve resource utilization, and
- The best technology to use.
Let’s dive in!
What is Resource Allocation and Utilization?
In project management , the two key resources-related phrases we use are “resource allocation” and resource utilization”.
Despite sounding similar, resource allocation and resource utilization are two different things. They’re both equally important to the effectiveness and efficiency of your projects and operations.
Resource allocation is the process of assigning resources appropriately in order to achieve certain deliverables and overall company goals. As the project manager, it’s important to keep an eye on how the resources assigned perform as the project progresses and reshuffle them whenever necessary.
On the other hand, resource utilization is the process of measuring how effectively your company is making use of all available resources. Resource utilization rates show how much of your resources are being spent on billable tasks. Tracking utilization can also be helpful for measuring productivity.
How Does Effective Resource Utilization Impact Your Business?
So why should you care about resource utilization within your business? For good and bad reasons.
Ineffective utilization can create business challenges and even lead to losses. It’s also important to be aware of why paying attention to your resource utilization can be beneficial for the business and ultimately lead to better profits.
Challenges of ineffective resource utilization
First, let’s discuss the challenges.
For a business to thrive, it must have the right resources at its disposal. However, it isn’t enough to just have resources, you must ensure that they’re utilized where they bring the most value. Ineffective or suboptimal resource utilization can lead to poor productivity, project delays, decreased quality, increased costs, missed opportunities, and low morale.
Failing to make the most of your resources could easily hamper the ability to deliver on projects as promised. And when this happens, you’ll certainly have unhappy clients and this could quickly destroy your company’s reputation and affect your revenue.
Benefits of effective capacity management
On the other hand, effective resource utilization will enable your organization to:
- Improve your ROI: Proper utilization of your available resources ensures that they’re invested in productive work. You’re able to ensure that you focus your resources on work that brings the most returns. In return, they generate revenue for the company thereby improving your RO .
- Plan your project resources better: Real-time visibility of resource utilization enables project managers to better monitor resource performance. This allows you to know which resource is better utilized in specific projects hence enabling you to plan your resources better .
- Forecast future requirements better: Tracking your utilization will enable you to better forecast resource requirements in the future. Take cues from how you’re utilizing resources for current projects and use the learnings to predict and plan for future projects.
5 Strategies to Improve Your Business’ Resource Utilization
According to Gartner analyst Robert Handler , the best utilization rate is between 70-80%. Why not 100% you ask?
If your resources are spending more than 80% of their time on billable tasks, there’s a high likelihood they’re less productive than they need be. Ultimately this costs your company time and money. Therefore, project managers, must ensure resources are utilized in the most essential activities instead of mundane ones.
So how do you maximize the utilization rate without draining your resources? Here are five best practices that will help you achieve this:
1. Take stock of your resources
To start with, take stock of all internal and external resources available and assess their ability to meet your business’s needs. Consider the capabilities of each resource. When reviewing your human resources, assess their levels of experience and training.
Taking stock of your resources gives you a clear picture of any gaps in how they’re being utilized. Additionally, it may reveal opportunities to leverage the higher-level capabilities of your resources—something you may have previously missed.
Finding and keeping track of all this information manually can be difficult. Mission Control makes it easier for you to track this data and make decisions based on it. For example, the Role Utilization feature gives you a clear overview of how your human resources are performing. You can see how many hours each resource is meant to work per week and compare it to the total hours logged for that week.
2. Choose the best utilization methodologies
Now that you know what resources you have and where they are most useful, you need to decide the kind of methodology you’ll use to ensure they prioritize strategic work.
Popular project management methodologies include Agile, Scrum, Kanban, Stage-Gate and more. Each methodology serves a different purpose, so it’s important to choose one that can help you effectively monitor resource utilization.
You may want to choose a methodology that allows you to monitor unplanned work especially when it comes to your human resources. Unplanned work can easily steal from your resource capacity and create bottlenecks that hold back the progress of the project.
For example, if you were to choose Kanban and create a Kanban board it would be very helpful for getting a visual overview of your project and how your resources are being used. You’d have a clear picture of staff workload and the flow of work throughout the project.
This would be useful for better resource allocation and capturing when certain resources are overcommitted. You don’t want to overwork your resources otherwise you’ll have quality problems and a reduction in overall output.
A project management tool can be very helpful for adopting a project management methodology and making the most of it for resource utilization. Whether it’s Kanban or Scrum or anything in between, Mission Control can be customized to suit your needs.
3. Plan your project
When it comes to being efficient, planning is important. It allows you to align projects and resources to the strategic outcomes they are meant to support. When planning your project, identify resources that you’re likely to need for the completion of the project. Then, have an estimate of the time each resource needs and its role in the completion of a particular task.
Generating a project plan for a new project can eat into your valuable time. Mission Control ’s Project Generation tool has been created to completely streamline project planning. You can quickly launch a new project and include related milestones, actions, checklist items, contributors, etc. You can also automatically generate project plans from previously created templates making your project planning a breeze.
4. Track and report time
Having identified which resources you need to complete the project and determined the time required, next you need to track your resources. Unfortunately, many companies skip this important step. HubSpot’s Marketing Agency Growth Report found that only 58% of agencies were tracking their team’s utilization rates.
Time tracking allows you to get a better view of how resources are performing and identify gaps and available opportunities. It also enables you to generate reports on billable and non-billable hours, which will help you know if you are efficiently or effectively leveraging your resources. Understanding how resources utilize their billable time can give your business a sustainable competitive advantage.
When it comes to tracking your human resource time, keep in mind that not everyone will be immediately receptive to time reporting. Keep things simple and easy. Start with an uncomplicated time tracking tool—like the one built into Mission Control . It’s straightforward and will help ease the adoption of time tracking. It will also make generating timesheets easier (you can actually automate this process!).
5. Keep improving
Don’t go too hard on yourself if things don’t go well at first. Realize resource management is an ongoing process that requires continuous improvement. No matter how well you plan a project, things change. Unexpected events and changes can easily affect your resource utilization system. Don’t fret, simply go back to the drawing board and refocus your resources based on your immediate priorities.
How Technology Can Assist with Resource Utilization
Managing your resources proactively is vital to improving business performance . Project managers have an important role to play in optimizing resource allocation and utilization.
When equipped with the right tools, project managers can tell the type and amount of resources available. They can in return focus on efficient allocation and usage of resources thereby reducing wastage.
Whether you are just getting started or looking to improve your resource management system, Mission Control can help with a data-driven project management solution.
Efficient resource utilization requires proper project planning. Use Mission Control’s Project Generation tool to streamline your project planning and increase efficiency. Once you kick off your project, use the Resource Utilization feature to monitor your resources in real-time. You can view how well resources are being utilized by comparing scheduled billing hours and actual billable hours used.
Request a demo for a real-time view of how Mission Control can help you utilize your resources and increase your ROI.
Recent Articles
- Meet Our New Account Executive: Julian Ricciardi
- Top 10 Project Management Apps for Salesforce
- How to Manage Projects in Salesforce
- Kosmo’s Feature Focus: Action Splitter
- Kosmo’s Feature Focus: Calendar Converter
Related Articles
- Stage Gate Project Management - What it is & How it works
- Project Management Office (PMO): Roles and Responsibilities
- What is the PMBOK Methodology in Project Management?
- Salesforce Summer Release 2023 Guide: Key Dates, New Features and More

SALESFORCE PROJECT MANAGEMENT SOFTWARE
Ready for take off? Click below and take a look around with your free 14 day trial.

THE FEATURES
Explore and discover the latest features of our Mission Control software.
Join our email list for all the latest news and updates at Mission Control HQ.
Sign up to our Newsletter
- Case Studies
- Company Role Benefits
- Industry Benefits
- Business Impact Report
- Getting Started
- Training Videos
- Knowledge Base
- Fundamentals Library
SO WHAT’S NEW
- Release Notes
- Project Management Blog
- Kosmo Campfire Webinars
TALK WITH US
- Get In Touch
- Arrange a Demo
- Create a ticket
- Support options
- Intellimail
- Privacy Policy
- Terms & Conditions

©2024 Aprika Business Solutions Ltd. All rights reserved.
Get your 14 Day FREE TRIAL
Simply enter your email address below, and we will set you on your way to your Free Trial. Enjoy the ride!

Discover the business and economic impacts of Mission Control
Sign up to our newsletter.
EECS Strategic Plan
Strategic plan - eecs department .
Below is a summary of the Jerome J. Lohr College of Engineering Impact 2018 Strategic Goals 1, 2 and 3. In concert with the first three COE goals, a list of key indicators and expectations for each of these goals is provided. This list serves as a guide to the department as the faculty and staff work towards their individual and collective aspirations. To optimally support these endeavors, the department believes it needs to hire one tenure track computer science assistant professor and two tenure track electrical engineering assistant professors in the coming years.
Strategic Goal 1: Enhance academic excellence through relevant programs, engaged learners, and continuous improvement of student learning.
These new professors will be required to:
- Participate in national teaching/learning workshops.
- Lead and/or present at national, university or college-related teaching/learning/advising workshops.
- Consider the regional workforce needs and engage with industry through company sponsored projects (senior design).
- Participate in all assessment activity that will lead towards continuous program improvement of their programs.
- Recruit international undergraduate and graduate students.
- Recruit women and minority students.
- Improve undergraduate student retention.
- Assist with student placement through industry connections.
- Promote SDSU honors program.
- Advise students about regional, state and national scholarships and fellowships.
- Encourage student participation in regional, national and international events.
Teaching areas needed in computer science:
- Database systems
- Network and computer security (cyber security)
- Computer architecture (engineering)
Teaching areas needed in electrical engineering:
- Computer engineering
- Controls and communications engineering
- Biomedical engineering and advanced electronics
Strategic Goal 2: Advance new knowledge, innovation and technology transfer to promote economic development for the state, region and nation.
- Develop a strong research program that is able to provide and sustain funding for M.S. and Ph.D. (EE) students.
- Develop research that leads towards invention disclosures, royalty-bearing IP licenses and/or new start-up companies.
- Publish journal and conference papers in peer-reviewed scholarly venues.
Research areas needed in computer science:
- Strengthen and/or complement existing areas of research in computer science and develop new areas and collaborations with other university research centers.
- Large data sets, including medical image processing, satellite image processing, social information and/or precision agriculture.
- Computer security, including cloud computing and smart power grid concerns.
- Machine learning, including data mining techniques for finding patterns in large bodies of data, finding similar medical images from data warehouse, improving control of stochastic and nonlinear dynamic systems through reinforcement feedback; learning robot control strategies; finding patterns in large bodies of data represented in graphical form, including social networks; extracting or retrieving information in natural language; classification of genetic data; and using learning methods for improving discrete optimization algorithms.
Research areas needed in electrical engineering:
- Strengthen and/or complement existing areas of research, including micro and nanoelectronic materials and devices, power and energy systems and image processing.
- Biomedical research in MEMS, nanoMEMS, or microfluidics in collaboration with the chemistry or biology departments and maximize use of existing research laboratories, including cleanroom, chemistry, laser and characterization labs.
- Controls and communications research applied to power and energy systems or precision agriculture.
- Image processing with emphasis in the satellite remote sensing or biomedical areas.
Strategic Goal 3: Extend outreach through collaborative partnerships and engagement with academic units, public entities and industry.
- strengthen and/or develop industry partnerships with existing companies (EROS, CPSS Members, Sanford/Mayo/Avera, Raven, AGCO), and new companies with needs related to our research strengths.
- develop existing and new relationships with regional and national companies to help improve participation in our career fairs.
- participate in and develop/host regional and national workshops, seminars, courses and conferences.
- assist with and promote K-12 STEM outreach events.
Outreach areas needed in computer science:
- Develop and strengthen partnership with EROS, Mayo, City Bank and AGCO.
- Develop relationships with regional companies to expand student opportunities for internships and full-time employment.
- Contribute in the development and support of the CS Program Design Competition, BEST Robotics, ACM/UPE and other related-events.
Outreach areas needed in electrical engineering:
- Develop and strengthen partnership with EROS, CPSS Members, Raven, Sanford and Mayo.
- Contribute in the development and support of the Robotics Club, electrical engineering summer camp, BEST Robotics, IEEE/HKN and other related-events.
JavaScript seems to be disabled in your browser. For the best experience on our site, be sure to turn on Javascript in your browser.
Cannabis Store
Your Cannabis Store
Visit a Verilife dispensary for all of your cannabis store needs. Browse our medical and recreational dispensary menus, and enjoy shopping for buds with our Buds.
Visit a Verilife dispensary near you for all your cannabis needs. Browse our medical and recreational menus to find your favorite products.

Find a Dispensary Near You
Verilife dispensaries are located throughout Illinois, Maryland, Massachusetts, New York, Ohio, and Pennsylvania. Find your closest dispensary and start shopping today.
Massachusetts
New York
Pennsylvania

Join our dispensary rewards program, and start earning points on all of your purchases. VeriVIP points have no limit and can be used at any time.

Talk About Terpenes
Dive into the world of terpenes, the fascinating little compounds that give cannabis its unique flavors and aromas.

Edible Dosage: What’s Right for You?
How much is too little? How much is too much? In this guide, we’ll break down how edibles are dosed and how to find the right amount for you.
Frequently Asked Questions (FAQs)
Here are some of the most common questions we get at our dispensaries. Remember to check state-specific rules and regulations before visiting a local dispensary.
What do I need to bring with me for my first dispensary visit?
If you are visiting a dispensary, make sure to bring a valid, state-issued photo ID as this is a requirement for every state (most forms of government identification are also accepted). If you are a medical marijuana patient, you’ll also need to bring your valid medical cannabis card. There may be additional requirements, so be sure to review all state-specific guidelines before your visit.
Can I buy marijuana from a dispensary without a medical card?
Some states are medical only, which means you need to have a valid medical marijuana card before you can visit a dispensary. Other states are adult-use, allowing adults 21 and over to shop for cannabis products. Check the rules for your specific state before planning your dispensary trip.
What is the state tax on marijuana?
Taxes on medical and recreational purchases vary by state. Additional taxes may include municipal or county taxes.
How can I become a budtender?
We have a variety of budtender positions available, as well as roles in our dispensaries, cultivation centers, and corporate offices. Check out our careers page for more information.
How do I know what to buy at a dispensary?
We recommend browsing the dispensary menu ahead of time to familiarize yourself with the cannabis products available. Otherwise, you can ask a budtender at the dispensary to help you select the products that will give you the experience you want.
Medical Marijuana Card
How can i apply for a medical marijuana card in illinois.
Click here for step-by-step instructions for how you can apply for a medical cannabis card in Illinois.
Your Remaining Allowances
Illinois residents
Sign In or Create an Account to track your medical allowance
IMAGES
VIDEO
COMMENTS
Here's an example outline of a research plan you might put together: Project title. Project members involved in the research plan. Purpose of the project (provide a summary of the research plan's intent) Objective 1 (provide a short description for each objective) Objective 2. Objective 3.
4. Manage the timeline and resources. Time constraints are an inevitable part of research dissemination. Deadlines for publications can be months apart, conferences may only happen once a year, etc. Any avenue used to disseminate the research must be carefully planned around to avoid missed opportunities.
Study with Quizlet and memorize flashcards containing terms like Managers are responsible for getting things done/achieving goals which means they are __ and for maximizing all available resource to do so which is called __, A common tool in the initial stages of planning is SWOT analysis, When we use our sources of influence to inspire action to be taken by others, we are practicing which of ...
Once a decision has been made that there is a need for change, a proposal to meet that need and implement the decision is developed. When the proposal is drafted, the time and other resources required to implement and evaluate it can be assessed to determine if the benefits outweigh the costs of the exercise and to inform planning.
5. Take Breaks. Taking breaks is essential for managing research time because it helps prevent burnout, improves productivity, and boosts creativity. When you take breaks, you give your brain a chance to recharge and reset, which can help you stay focused and engaged in your research project.
Resource Allocation Process: How to Allocate Project Resources. Resource allocation is a plan that you develop to make the most of the available resources at your disposal in a project, which makes it a critical resource planning activity. This is mostly a short-term plan set in place to achieve goals in the future.
4 Minute Read - . In the last blog post, I introduced a series of posts that deal with project planning in the research context.This post thus forms part of a larger set of posts and should ideally be read in conjunction with them. This is the second post of the series, and in the first post, I wrote about the vision and objectives of your research project.
Project, program, and portfolio management (PPPM) often focuses on how and when things get done, without substantial emphasis on the resources needed to accomplish these activities. Improving the Capacity and Demand Planning capabilities of a team or organization can have a tremendous positive impact on results, even when no other changes are implemented and staffing and funding levels remain ...
In order to effectively manage project resources, they must be planned in advance. The primary output of the Project Resource Management knowledge area is a resource management plan. There are four steps to a strong project resource management. Determine required resources. Acquire resources.
Efficient resource allocation is not a one-time task but an ongoing process that requires continuous evaluation, adjustment, and collaboration. In conclusion, resource allocation plays a vital role in organizational success. It involves distributing available resources in an optimal manner to maximize their impact and minimize waste.
On the other hand, effective resource scheduling ensures that the required resources are available when needed, minimizing delays and keeping the project on track. Key Planning Areas. Resource scheduling directly affects several key project planning areas, including time, scope, cost, risk, quality, and resources.
1. Dream Big, But Start Small. Have a big dream but start small. Do an initial check of the capacity and demand of a certain product or service, thus maximizing its benefits before venturing on to ...
In the context of maintaining flexibility while planning, unlike traditional planning, options-based planning _____. A. involves committing people and resources to a particular course of action B. involves making large investments in many alternative plans over a long period of time C. reduces flexibility D. involves maintaining slack resources
The tips mentioned below on how to manage resources will do wonders for your corporation if implemented in the correct manner. 1. Plan to Plan. Planning is important when it comes to being efficient. Time is money and it is best to plan for effective resource management from the very beginning of projects.
Step 2: Estimate the work and identify the resources required. Step 3: Consider quality and budget to request the right resource level. Step 4: Communicate your resource needs. Step 5: Onboard resources and assign them to tasks with a resource allocation plan. Step 6: Monitor progress, adapting and optimizing as you go.
3. Plan your project. When it comes to being efficient, planning is important. It allows you to align projects and resources to the strategic outcomes they are meant to support. When planning your project, identify resources that you're likely to need for the completion of the project.
The power of lean strategy, a method that combines the bottom-up approach of lean start-ups with the top-down orientation of strategic management, offers a solution. By wisely managing and deploying their resources, entrepreneurs can make the most of their opportunities. This article explores the importance of resource management, understanding ...
Research requires planning, developing, and maximizing the available resources. B. Explain each quality of a good researcher in at least 2 sentences each. ... They are able to adapt to changing circumstances and use all available resources to achieve their research objectives. They are innovative and can think outside the box to develop new ...
Strategic Plan - EECS Department Below is a summary of the Jerome J. Lohr College of Engineering Impact 2018 Strategic Goals 1, 2 and 3. In concert with the first three COE goals, a list of key indicators and expectations for each of these goals is provided. This list serves as a guide to the department as the faculty and staff work towards their individual and collective aspirations. To ...
Some states are medical only, which means you need to have a valid medical marijuana card before you can visit a dispensary. Other states are adult-use, allowing adults 21 and over to shop for cannabis products. Check the rules for your specific state before planning your dispensary trip.