
An official website of the United States government
Here’s how you know
Official websites use .gov A .gov website belongs to an official government organization in the United States.
Secure .gov websites use HTTPS A lock ( Lock Locked padlock icon ) or https:// means you’ve safely connected to the .gov website. Share sensitive information only on official, secure websites.

Anabolic Steroids and Other Appearance and Performance Enhancing Drugs (APEDs)
- Anabolic-androgenic steroids are the best-studied class of appearance and performance enhancing drugs (APEDs). APEDs are used to improve appearance by building muscle mass or to enhance athletic performance.
- Although anabolic steroids and other APEDs may directly and indirectly have effects on a person’s mood, they do not typically produce a euphoric high. However, people who use these substances may develop a substance use disorder, defined as continued use despite adverse consequences.
- Anabolic steroids can cause severe, long-lasting, and in some cases, irreversible damage. They can lead to early heart attacks, strokes, liver tumors, kidney failure, and psychiatric problems. In addition, stopping steroid use can cause depression, often leading to resumption of use.
What are anabolic steroids and other appearance and performance enhancing drugs (APEDs)?
Anabolic-androgenic steroids , often shortened to "anabolic steroids," "steroids," or "androgens," 2,3 are the most widely misused APED. These are synthetic substances similar to the male sex hormone testosterone. They promote the growth of skeletal muscle (anabolic effects) and the development of male sexual characteristics (androgenic effects) in both males and females. 2
These compounds are sometimes used medically to treat delayed puberty and muscle loss due to disease 4 and to treat low levels of testosterone in men with an associated medical condition. 5 Anabolic androgenic steroids can also improve feelings of well-being and increase bone strength, but are not approved for these purposes. However, testosterone-supplementation therapy is an increasingly common treatment for mood and sexual performance problems associated with male aging, and it is controversially being prescribed even for younger men. 6
Note that in the context of this report, anabolic steroids refer only to the non-prescribed use (misuse) of testosterone and testosterone-like substances by athletes and non-athlete bodybuilders. This research report will not cover image enhancers, such as dermal fillers , Botox , or the skin tanner, melanotan . 7
Non-steroidal anabolics , include insulin, insulin-like growth hormone (IGF), and human growth hormone (HGH)—substances that are produced by the human body and are prescribed for legitimate medical uses but also sometimes misused for performance enhancement.
Ergo/thermogenics are compounds used to decrease body fat or to promote leanness versus muscle mass in endurance athletes. 8 The three main categories of ergo/thermogenics are:
- Xanthines : compounds that increase attention and wakefulness and suppress appetite. Examples are caffeine, the asthma drug theophylline, and theobromine—a substance found in chocolate, coffee, and tea. 9
- Sympathomimetics : drugs that are similar in structure and action to epinephrine and norepinephrine—natural chemicals in the body that increase heart rate, constrict blood vessels, and raise blood pressure. An example is ephedrine, which is derived from the ephedra plant. Ephedrine/ephedra used to be included in dietary supplements that promoted weight loss, increased energy, and enhanced athletic performance. 10 In 2004, the FDA banned the U.S. sale of dietary supplements containing ephedrine/ephedra due to various possible health risks including cardiovascular and nervous system effects. 11
- Thyroid hormones : substances that regulate metabolism by altering the function of the thyroid. 12 Cytomel is an example.
Nutritional/dietary supplements are substances purchased legally from nutritional stores or via the internet that are often taken in combination with other APEDs. Creatine, which boosts exercise capacity, is one common example.
In the United States, dietary supplements containing steroid precursors such as tetrahydrogestrinone (THG) and androstenedione previously could be purchased legally without a prescription. Athletes took steroid precursors in an effort to boost testosterone levels. Less is known about the side effects of steroid precursors, but if large quantities of these compounds substantially increase testosterone levels in the body, then they also are likely to produce the same side effects as anabolic steroids themselves. 13 The purchase of these supplements, with the notable exception of dehydroepiandrosterone (DHEA), became illegal after the passage of the Anabolic Steroid Control Act of 2004, which amended the Controlled Substances Act. 14
What is the scope of anabolic steroid use in the United States?
All data refer to the United States population.
It is difficult to estimate the prevalence of steroid misuse in the United States because many national surveys that ask about drug use do not include questions about steroids. However, data on steroid misuse among young students are available from the NIDA-supported Monitoring the Future Survey .
How many young students use steroids?
In 2022, an estimated 0.8% of 8th graders, 0.5% of 10th graders, and 1.3% of 12th graders reported misusing steroids in the past 12 months. Source: 2022 Monitoring the Future Survey .
Why are anabolic steroids misused?
Anabolic steroids increase lean muscle mass when used in conjunction with weight training. The aim, for non-athlete weightlifters, is typically improvement of appearance. Steroid use is often associated with a form of male body dysmorphic disorder called muscle dysmorphia, a preoccupation with the perceived inadequate size of their muscles. 19
As a result, some users report taking anabolic steroids to increase confidence and because they feel that they are at a point where they can no longer get bigger through weight training alone. Most users report that anabolic steroids help them achieve their ideal body. 28
Increasing muscle mass may also promote strength, which can improve performance in certain types of sports. More benefit is seen for strength-dependent sports (weightlifting, shot-put throwing, football) than for sports that require speed, agility, flexibility, and/or endurance. 29
Anabolic steroid users also report that their muscles recover faster from intense strain and muscle injury. 30 Research in animals has not conclusively supported this belief, with some showing that anabolic steroids can enhance recovery from certain types of muscle damage, 31,32 but others finding no benefit in taking anabolic steroids to enhance muscle recovery. 33
Anabolic steroid users report using an average of about 11 APEDs per year. They are also more likely than non-steroid users to take supplements such as protein powders and creatine; estrogen blockers; ergo/thermogenics, such as caffeine or ephedrine; medications for erectile dysfunction; and other hormones such as insulin, thyroid hormones, and human growth hormone. 26
How are anabolic steroids used?
Commonly misused steroids.
- Anadrol (oxymetholone)
- Anavar (oxandrolone)
- Dianabol (methandienone )
- Winstrol (stanozolol)
- Restandol (testosterone undecanoate)
Injectable Steroids
- Deca-Durabolin (nandrolone decanoate)
- Durabolin (nandrolone phenpropionate)
- Depo-Testosterone (testosterone cypionate)
- Agovirin (testosterone propionate)
- Retandrol (testosterone phenylpropionate)
- Equipoise (boldenone undecylenate) 29,34
Cycling, stacking, pyramiding, and plateauing
Steroids are often used in patterns called "cycling." This involves taking multiple doses of steroids over a specific period of time, stopping for a period, and starting again. People who misuse steroids also typically "stack" the drugs, meaning that they take two or more different anabolic steroids, mix oral and/or injectable types, and sometimes even take compounds that are designed for veterinary use. 37,38 The belief is that different steroids interact to produce an effect on muscle size that is greater than the effects of each drug individually, 36 a theory that has not been tested scientifically.
Another common mode of steroid misuse is referred to as "pyramiding," which typically involves taking them in a cycle of six to 12 weeks, tapering gradually rather than starting and finishing a cycle abruptly. At the beginning of a cycle, the person starts with low doses of the drugs being stacked and then slowly increases the doses. In the second half of the cycle, the doses are slowly decreased to zero. This is sometimes followed by a second cycle in which the person continues to train but without drugs. Steroid users believe that pyramiding allows the body time to adjust to the high doses, and the drug-free cycle allows the body's hormonal system time to recuperate. 2
A technique called "plateauing" may also be used, whereby steroids are staggered, overlapped, or substituted with another type of steroid to avoid developing tolerance. 36 As with stacking, the effects of pyramiding, cycling, and plateauing have not been substantiated scientifically.
What are the side effects of anabolic steroid misuse?
A variety of side effects can occur when anabolic steroids are misused, ranging from mild effects to ones that are harmful or even life-threatening. Most are reversible if the user stops taking the drugs. However, others may be permanent or semi-permanent.
Most data on the long-term effects of anabolic steroids in humans come from case reports rather than formal epidemiological studies. Serious and life-threatening adverse effects may be underreported, especially since they may occur many years later. One review found 19 deaths in published case reports related to anabolic steroid use between 1990 and 2012; however, many steroid users also used other drugs, making it difficult to show that the anabolic steroid use caused these deaths. 39 One animal study found that exposing male mice for one fifth of their lifespan to steroid doses comparable to those taken by human athletes caused a high frequency of early deaths. 40
Cardiovascular System
Steroid use has been associated with high blood pressure; 41 decreased function of the heart’s ventricles; 23,41,42 and cardiovascular diseases such as heart attacks, 43 artery damage, 44 and strokes, 45,46 even in athletes younger than 30. Steroids contribute to the development of cardiovascular disease partly by increasing the level of low-density lipoprotein (LDL) 47 and decreasing the level of high-density lipoprotein (HDL). 47,48 High LDL and low HDL levels increase the risk of atherosclerosis, a condition in which fatty substances are deposited inside arteries and disrupt blood flow. If blood is prevented from reaching the heart or brain, the result can be a heart attack or stroke, respectively. Steroids also increase the risk that blood clots will form in blood vessels, potentially disrupting blood flow and damaging the heart muscle, so that it does not pump blood effectively. 49
Hormonal System
Steroid use disrupts the normal production of hormones in the body. Changes that can be reversed include decreased sperm production, 56–59 decreased function of the testes (hypogonadism) that leads to low testosterone levels, 60 and shrinking of the testicles (testicular atrophy). 56,61 Irreversible changes include male-pattern baldness and breast development (gynecomastia) in men. 59,62 Anabolic steroids may also act upon the hormone system to increase the risk of testicular cancer, especially when steroids are used in combination with insulin-like growth factor. 63
In females, anabolic steroids cause masculinization. Specifically, breast size and body fat decrease, the skin becomes coarse, and the voice deepens. 64 Women may experience excessive growth of body hair but lose scalp hair. 65 With continued administration of steroids, some of these effects become irreversible. It is commonly believed that anabolic steroids will produce irreversible enlargement of the clitoris in females, although there are no studies on this. 66
Many people who inject anabolic steroids may use nonsterile injection techniques or share contaminated needles with other users. This puts these steroid users at risk for acquiring life threatening viral infections, such as HIV and hepatitis B and C. 76 In addition, animal models indicate that anabolic steroids suppress the immune system, 77 which could worsen infections.
Steroid misuse has been associated with liver damage, 50,51 tumors, 46,52,53 and a rare condition called peliosis hepatis, in which blood-filled cysts form in the liver. 54 The cysts can rupture, causing internal bleeding and even death in rare cases. 55
Musculoskeletal System
Rising levels of testosterone and other sex hormones normally trigger the growth spurt that occurs during puberty and adolescence. These rising levels of testosterone also provide the signals to stop growth. 67 When a child or adolescent takes anabolic steroids, the resulting artificially high sex hormone levels can prematurely signal the bones to stop growing. 68
Evidence suggests that weightlifters who misuse anabolic steroids have stiffer tendons, which could lead to an increased risk for tendon injury. 69
Steroid misuse can cause acne, 70–72 hair loss on the head, cysts, and oily hair and skin. 65 Users who inject steroids may also develop pain and abscess formation at injection sites. 73
Anabolic steroids can also produce jaundice, or yellowing of the skin or eyes, as a result of damage to the liver. 74,75
How does anabolic steroid misuse affect behavior?
Case reports and small studies indicate that anabolic steroids increase irritability and aggression, 75 although findings may be confounded by personality traits that are overrepresented in steroid users (i.e., antisocial, borderline, and histrionic personality disorder) 78 and use of other drugs. 79 People who misuse anabolic steroids report more anger than nonusers, 80 as well as more fights, verbal aggression, and violence toward their significant others, 81 sometimes called "roid rage." One study suggests that the mood and behavioral effects seen during anabolic-androgenic steroid misuse may result from secondary hormonal changes. 82
Scientists have attempted to test the association between anabolic steroids and aggression by administering high steroid doses or placebo for days or weeks to human volunteers and then assessing behavioral symptoms. In one such study, researchers found that testosterone over a six week period was associated with increased aggression, as assessed by a questionnaire and computer-based model of aggressive behavior. 83 In addition, high steroid doses produced greater feelings of irritability and aggression than placebo, 84 although the effects appear to be highly variable across individuals, 19 and other studies have not shown that effect. 85 One possible explanation, according to the researchers, is that some but not all anabolic steroids increase irritability and aggression.
Psychiatric Disorders
Anabolic steroid users are more likely than nonusers to report anxiety. 34,86 Moderate to high doses of anabolic steroids are also associated with major mood disorders such as mania, hypomania, 87 and major depression. 86,87 In one study, manic symptoms were not uniform across individuals, with most showing little psychological change, whereas a few demonstrated prominent effects. 19
Other Drug Use
Anabolic steroid users are more likely to use drugs such as marijuana, prescription opioids, cocaine, 88 or heroin. 86 In a study of men admitted to treatment for opioid use disorders, 25 percent reported prior use of anabolic steroids. Some described first learning about opioids from friends at the gym, and that they first purchased opioids from the same person who had sold them the anabolic steroids. 89 In a study of anabolic steroid users dependent upon the injectable opioid analgesic nalbuphine, most reported that they began using nalbuphine to treat pain from weightlifting injuries. They also described widespread use of nalbuphine in their gyms. 90
Research also indicates that some users might turn to other drugs to alleviate some of the negative effects of anabolic steroids. For example, a study of 227 men admitted in 1999 to a private treatment center for addiction to heroin or other opioids found that 9.3 percent had previously misused anabolic steroids. Of these, most reported using opioids to counteract insomnia, irritability, depression, and withdrawal from anabolic steroids. 91
What are the risks of anabolic steroid use in teens?
Unlike most illicit drug use, misuse of anabolic steroids most commonly begins in young adulthood rather than adolescence. But steroid use in teens is of concern, especially since the hormonal systems they interact with play a critical role in brain development during these years. 92–96 In adolescent rodents, exposure to anabolic steroids increased neuronal spine densities in the hippocampus and amygdala—brain regions involved in learning and emotions (e.g., aggression), respectively. Four weeks after withdrawal, these increases in neuronal spine densities returned to normal in the amygdala, but not in the hippocampus. This suggests that pubertal steroid exposure could produce long-lasting structural changes in certain brain regions. 97
Teens who use anabolic steroids may also be at increased risk for some cognitive side effects compared with adults. For example, males who begin using anabolic steroids during the teen years show increased impulsivity and decreased attention, compared to men who began using steroids in their adult years. 98 In adolescent rats, anabolic steroid exposure is associated with electrolytic imbalances, hyperactivity, anxiety, and increased sympathetic autonomic modulation (e.g., fight or flight response) during adulthood, even when steroid use was discontinued during adolescence. 99 In addition, adolescent male hamsters given anabolic steroids show increased aggression, even after steroid use is discontinued. These aggressive effects are paralleled by changes in levels of serotonin 100,101 and androgen receptors in the rodent brain. 102
How do anabolic steroids work in the brain?
Anabolic steroids act at androgen receptors to influence cellular functioning and gene expression. In addition to regulating pathways involved in the development of male characteristics, 103 activation of androgen receptors also produces rapid increases in calcium levels within skeletal muscle, heart, and brain cells. 104 Calcium plays important roles in neuronal signaling.
Research with human cells demonstrates that anabolic steroids also interact with certain types of GABA A receptors, which could mediate the increased anxiety reported by steroid users. 105,106 In addition, animal studies show that anabolic steroids increase serotonin levels in brain regions involved in mood 107 and dopamine levels in reward-related brain regions. 107,108 Chronic use of anabolic steroids has also been shown to cause dysfunction of these reward pathways in animals. Specifically, rats given twice daily nandrolone injections for four weeks showed loss of sweet preference (a sign of reward dysfunction) that was accompanied by reductions of dopamine, serotonin, and noradrenaline in the nucleus accumbens, a reward-related brain region. 109
Are anabolic steroids addictive?
An undetermined percentage of steroid users may develop a steroid use disorder. Substance use disorders are defined by continued use despite adverse consequences; for steroid users, these may include physical or psychological problems such as breast growth (in men), sexual dysfunction, high blood pressure, excessive fats in the blood, heart disease, mood swings, severe irritability, or aggressiveness. Anabolic steroid users also may give up other important activities for fear that they will miss workouts, violate their dietary restrictions, or be prevented from using steroids. Steroid users also typically spend large amounts of time and money obtaining the drugs, and they may try to reduce or stop anabolic steroid use without success—possibly due to depression, anxiety about losing muscle mass, or and other unpleasant effects of withdrawal. 110
Withdrawal from steroids occurs when an individual develops dependence. A review of the research suggests that about 32 percent of people who misuse anabolic steroids become dependent. 23 Symptoms of dependence can include tolerance, which is needing to take more steroids to achieve the same effects. Another indicator of dependence is withdrawal once anabolic steroid use stops. 110 Withdrawal symptoms can include fatigue, restlessness, loss of appetite, insomnia, reduced sex drive, and steroid cravings. 111 The most dangerous of the withdrawal symptoms is depression, because it sometimes leads to suicide attempts. 112
How are anabolic steroids tested in athletes?
Although non-athlete weightlifters account for the bulk of anabolic steroid misuse, occasional steroid use by professional and Olympic athletes to improve performance or cheat in competition ("doping") has done the most to raise awareness of steroid misuse. The World Anti-Doping Agency (WADA) was founded in 1999 to consistently apply anti-doping policies across sports organizations and governments around the world. Non-compliant organizations can face sanctions such as event cancellation, loss of WADA funding, or ineligibility to host events. 114

Refinements in drug testing have improved the ability to detect anti-doping violations, resulting in increased numbers of reported violations over recent years. For example, the discovery of long-term steroid metabolites has lengthened the drug detection window, making it more difficult for athletes to pass drug tests by simply discontinuing steroid use just prior to an event. In addition, more sensitive technologies have allowed detection of lower metabolite thresholds. 115
Although testing procedures are now in place to deter steroid use among professional and Olympic athletes, new designer drugs constantly become available that can escape detection and put athletes willing to cheat one step ahead of testing efforts. 116–118 To detect early use of designer steroids and provide more accurate baseline standards for each athlete, testing laboratories store data from each drug testing sample. These samples are then used as reference points for future testing, thereby eliminating the possibility that a person tests positive simply because he or she has naturally elevated levels of testosterone when compared to the general population. 119 Long-term use of designer steroids suppresses levels endogenous steroids in urine samples, which could be the first indication that an athlete is taking a designer steroid. 117
Drug Testing and Nutritional Supplements
Athletes taking over-the-counter nutritional supplements may believe that such products are safe. However, nutritional supplements are not subjected to the same pre-approval requirements and quality tests as FDA-approved medications. 120 For example, some supplements advertised to promote weight loss have been found to contain banned stimulants such as ephedrine 121 or clenbuterol. 122 Other research shows that supplements sometimes contain prohormones or anabolic steroids. 123 In a study looking at 634 nutritional supplements from 13 different countries, 15 percent included some type of prohormone not listed on the label. 115 Another study showed that some non-labeled prohibited substances could be detected by drug tests up to 144 hours later. 124
Nutritional supplements sometimes contain banned substances that are not indicated in their labels. 115,124 The FDA notes that consumers should be wary if a product meets any of these criteria:
- products claiming to be alternatives to FDA-approved drugs or to have effects similar to prescription drugs
- products claiming to be a legal alternative to anabolic steroids
- products that are marketed primarily in a foreign language or those that are marketed through mass e-mails
- sexual enhancement products promising rapid effects such as working in minutes to hours, or long-lasting effects such as 24 hours to 72 hours
- products that provide warnings about testing positive in performance enhancement drug tests 125
According to WADA’s codes, athletes are responsible for any prohibited substance found in their samples, regardless of whether ingestion was intentional or unintentional. However, sanctions may be reduced or avoided if the athlete can demonstrate that the substance was ingested through no significant fault or negligence on his/her part, or in some circumstances where the athlete did not intend to enhance performance. 126
What can be done to prevent steroid misuse?
Research suggests that high school athletes are less likely to use steroids if their peers and parents disapprove, indicating that peers and parents can be strong partners in prevention efforts. 127
However, research shows that simply teaching students about steroids' adverse effects does not convince adolescents that they will be adversely affected, nor does such instruction discourage young people from taking steroids in the future. Presenting both the risks and benefits of anabolic steroid use is more effective in convincing adolescents about steroids' negative effects, apparently because the students find a balanced approach more credible. 128
Research also indicates that some adolescents misuse steroids as part of a pattern of high-risk behaviors such as drinking and driving, carrying a gun, driving a motorcycle without a helmet, and using other illicit drugs. This suggests that a prevention program should focus on comprehensive high-risk behavior screening and counseling among teens who use anabolic steroids. 129
NIDA-Funded Prevention Research Helps Reduce Steroid Misuse
Studies show that one year after completion of the program, compared with a control group, ATLAS-trained football student athletes in 15 high schools had:
- less use of anabolic steroids and less intention to misuse them in the future
- less misuse of alcohol, amphetamines, and narcotics
- less misuse of "athletic enhancing" supplements
- less likelihood of engaging in hazardous behaviors such as drinking and driving
- better knowledge about anabolic steroid, alcohol, and marijuana effects; better knowledge of alternatives to steroid misuse; greater confidence in athletic abilities; and improved nutritional behaviors 130
What treatments are effective for anabolic steroid misuse?
People who use steroids often do not seek treatment for their use, with one study reporting that 56 percent of users had never told their physician about their use. 133 This could be because users feel their physician lacks knowledge about anabolic steroids. 133 In addition, many internet sites devoted to anabolic steroids and other APEDs challenge the professionalism of health care providers and offer their own medically questionable advice on the use of APEDs. 134 This makes it important for health care providers to be educated on the signs and symptoms of steroid use in their patients. 111
Current views recommend that treatment for steroid use address the underlying causes of the steroid use. This can include:
- psychological therapies (and possibly medications) for muscle dysmorphia
- endocrine therapies to restore function in those suffering from hypogonadism and to alleviate symptoms of depression
- antidepressants for those whose depression does not respond to endocrine therapies
- pharmacological and psychosocial treatments for patients who are also dependent on opioids, which appear to also be effective in alleviating signs of anabolic steroid dependence 135
Find More Resources on Anabolic Steroids and Other Appearance and Performance Enhancing Drugs
- Learn more about steroids and their legal status from the U.S. Drug Enforcement Administration
- Review patient resources on anabolic steroids from MedlinePlus .
- Explore publications about steroids from the U.S. Substance Abuse and Mental Health Services Administration.
- Kanayama G, Pope HG. History and epidemiology of anabolic androgens in athletes and non-athletes. Mol Cell Endocrinol . March 2017. doi:10.1016/j.mce.2017.02.039
- Rashid H, Ormerod S, Day E. Anabolic androgenic steroids: what the psychiatrist needs to know. Adv Psychiatr Treat . 2007;13(3):203-211.
- Lipsett MB, Korenman SG. Androgen Metabolism. JAMA . 1964;190(8):757-762. doi:10.1001/jama.1964.03070210063011
- Shahidi NT. A review of the chemistry, biological action, and clinical applications of anabolic-androgenic steroids. Clin Ther . 2001;23(9):1355-1390.
- Testosterone Information. https://www.fda.gov/drugs/drugsafety/ postmarketdrugsafetyinformationforpatientsandproviders/ucm161874.htm . Published March 3, 2015. Accessed May 26, 2017.
- Rao PK, Boulet SL, Mehta A, et al. Trends in Testosterone Replacement Therapy Use from 2003 to 2013 among Reproductive-Age Men in the United States. J Urol . 2017;197(4):1121-1126. doi:10.1016/j.juro.2016.10.063.
- Brennan R, Wells JSG, Van Hout MC. The injecting use of image and performance-enhancing drugs (IPED) in the general population: a systematic review. Health Soc Care Community . January 2016. doi:10.1111/hsc.12326.
- Hildebrandt T, Langenbucher JW, Carr SJ, Sanjuan P. Modeling population heterogeneity in appearance- and performance-enhancing drug (APED) use: applications of mixture modeling in 400 regular APED users. J Abnorm Psychol . 2007;116(4):717-733. doi:10.1037/0021-843X.116.4.71.
- Gennaro MC, Abrigo C. Caffeine and theobromine in coffee, tea and cola-beverages. Fresenius J Anal Chem . 1992;343(6):523-525.
- Ephedra. NCCIH. https://nccih.nih.gov/health/ephedra . Published November 9, 2011. Accessed November 6, 2017.
- Office of Dietary Supplements. Ephedra. https://ods.od.nih.gov/Health_Information/Ephedra.aspx . Published n.d. Accessed December 13, 2017.
- American Thyroid Association. Thyroid and Weight FAQ. June 2012. http://www.thyroid.org/thyroid-and-weight/ . Accessed November 6, 2017.
- 108th Congress FS. Regulation of Dietary Supplements: Hearing Before the Committee on Commerce, Science and Transportation .; 2003. https://www.gpo.gov/fdsys/pkg/CHRG-108shrg20196/pdf/CHRG-108shrg20196.pdf . Accessed February 7, 2018.
- 108th Congress. Anabolic Steroid Control Act of 2004 . Vol S.2195.; 2004. https://www.congress.gov/bill/108th-congress/senate-bill/2195/all-info . Accessed April 28, 2017.
- Freeman ER, Bloom DA, McGuire EJ. A brief history of testosterone. J Urol . 2001;165(2):371-373. doi:10.1097/00005392-200102000-00004.
- Altschule MD, Tillotson KJ. The use of testosterone in the treatment of depressions. N Engl J Med . 1948;239(27):1036-1038. doi:10.1056/NEJM194812302392704.
- Wade N. Anabolic Steroids: Doctors Denounce Them, but Athletes Aren’t Listening. Science . 1972;176(4042):1399-1403. doi:10.1126/science.176.4042.1399.
- Buckley WE, Yesalis CE, Friedl KE, Anderson WA, Streit AL, Wright JE. Estimated prevalence of anabolic steroid use among male high school seniors. JAMA . 1988;260(23):3441-3445.
- Pope HG, Kouri EM, Hudson JI. Effects of supraphysiologic doses of testosterone on mood and aggression in normal men: a randomized controlled trial. Arch Gen Psychiatry . 2000;57(2):133-140; discussion 155-156.
- Significant Dates in U.S. Food and Drug Law History. 2014. https://wayback.archive-it.org/7993/20170406045722/https://www.fda.gov/AboutFDA/WhatWeDo/History/Milestones/ucm128305.htm . Accessed June 4, 2016.
- A Dangerous and Illegal Way to Seek Athletic Dominance and Better Appearance - A Guide for Understanding the Dangers of Anabolic Steroids. March 2004. https://www.deadiversion.usdoj.gov/pubs/brochures/steroids/public/. Accessed April 25, 2017.
- Kanayama G, Boynes M, Hudson JI, Field AE, Pope HG. Anabolic steroid abuse among teenage girls: an illusory problem? Drug Alcohol Depend . 2007;88(2-3):156-162. doi:10.1016/j.drugalcdep.2006.10.013.
- Pope HG, Kanayama G, Athey A, Ryan E, Hudson JI, Baggish A. The lifetime prevalence of anabolic-androgenic steroid use and dependence in Americans: current best estimates. Am J Addict Am Acad Psychiatr Alcohol Addict . 2014;23(4):371-377. doi:10.1111/j.1521-0391.2013.12118.x.
- Irving LM, Wall M, Neumark-Sztainer D, Story M. Steroid use among adolescents: findings from Project EAT. J Adolesc Health Off Publ Soc Adolesc Med . 2002;30(4):243-252.
- Pope HG, Khalsa JH, Bhasin S. Body Image Disorders and Abuse of Anabolic-Androgenic Steroids Among Men. JAMA . 2017;317(1):23-24. doi:10.1001/jama.2016.17441.
- Ip EJ, Barnett MJ, Tenerowicz MJ, Perry PJ. The Anabolic 500 survey: characteristics of male users versus nonusers of anabolic-androgenic steroids for strength training. Pharmacotherapy . 2011;31(8):757-766. doi:10.1592/phco.31.8.757.
- Gruber AJ, Pope HG. Compulsive weight lifting and anabolic drug abuse among women rape victims. Compr Psychiatry . 1999;40(4):273-277.
- Wright S, Grogan S, Hunter G. Motivations for Anabolic Steroid use Among Bodybuilders. J Health Psychol . 2000;5(4):566-571. doi:10.1177/135910530000500413.
- American Academy of Pediatrics. Adolescents and anabolic steroids: a subject review. American Academy of Pediatrics. Committee on Sports Medicine and Fitness. Pediatrics . 1997;99(6):904-908.
- Bahrke MS, Wright JE, Strauss RH, Catlin DH. Psychological moods and subjectively perceived behavioral and somatic changes accompanying anabolic-androgenic steroid use. Am J Sports Med . 1992;20(6):717-724.
- Beiner JM, Jokl P, Cholewicki J, Panjabi MM. The effect of anabolic steroids and corticosteroids on healing of muscle contusion injury. Am J Sports Med . 1999;27(1):2-9.
- Ferry A, Noirez P, Page CL, Salah IB, Daegelen D, Rieu M. Effects of anabolic/androgenic steroids on regenerating skeletal muscles in the rat. Acta Physiol Scand . 1999;166(2):105-110. doi:10.1046/j.1365-201x.1999.00549.x.
- Ferry A, Vignaud A, Noirez P, Bertucci W. Respective effects of anabolic/androgenic steroids and physical exercise on isometric contractile properties of regenerating skeletal muscles in the rat. Arch Physiol Biochem . 2000;108(3):257-261. doi:10.1076/1381345520000710831ZFT257.
- Eklöf A-C, Thurelius A-M, Garle M, Rane A, Sjöqvist F. The anti-doping hot-line, a means to capture the abuse of doping agents in the Swedish society and a new service function in clinical pharmacology. Eur J Clin Pharmacol . 2003;59(8-9):571-577. doi:10.1007/s00228-003-0633-z.
- Medline Plus. Testosterone Topical. June 2016. https://www.nlm.nih.gov/medlineplus/druginfo/meds/a605020.html#why .
- Trenton AJ, Currier GW. Behavioural manifestations of anabolic steroid use. CNS Drugs . 2005;19(7):571-595.
- Evans NA. Gym and tonic: a profile of 100 male steroid users. Br J Sports Med . 1997;31(1):54-58.
- Wilson JD. Androgen abuse by athletes. Endocr Rev . 1988;9(2):181-199. doi:10.1210/edrv-9-2-181.
- Frati P, Busardò FP, Cipolloni L, Dominicis ED, Fineschi V. Anabolic Androgenic Steroid (AAS) related deaths: autoptic, histopathological and toxicological findings. Curr Neuropharmacol . 2015;13(1):146-159. doi:10.2174/1570159X13666141210225414.
- Bronson FH, Matherne CM. Exposure to anabolic-androgenic steroids shortens life span of male mice. Med Sci Sports Exerc . 1997;29(5):615-619.
- Urhausen A, Albers T, Kindermann W. Are the cardiac effects of anabolic steroid abuse in strength athletes reversible? Heart Br Card Soc . 2004;90(5):496-501.
- Kaskutas LA. Alcoholics anonymous effectiveness: faith meets science. J Addict Dis . 2009;28(2):145-157. doi:10.1080/10550880902772464.
- Vanberg P, Atar D. Androgenic anabolic steroid abuse and the cardiovascular system. Handb Exp Pharmacol . 2010;(195):411-457. doi:10.1007/978-3-540-79088-4_18.
- Baggish AL, Weiner RB, Kanayama G, et al. Cardiovascular Toxicity of Illicit Anabolic-Androgenic Steroid Use. Circulation . 2017;135(21):1991-2002. doi:10.1161/CIRCULATIONAHA.116.026945.
- El Scheich T, Weber A-A, Klee D, Schweiger D, Mayatepek E, Karenfort M. Adolescent ischemic stroke associated with anabolic steroid and cannabis abuse. J Pediatr Endocrinol Metab JPEM . 2013;26(1-2):161-165. doi:10.1515/jpem-2012-0057.
- Santamarina RD, Besocke AG, Romano LM, Ioli PL, Gonorazky SE. Ischemic stroke related to anabolic abuse. Clin Neuropharmacol . 2008;31(2):80-85. doi:10.1097/WNF.0b013e3180ed4485.
- Palatini P, Giada F, Garavelli G, et al. Cardiovascular effects of anabolic steroids in weight-trained subjects. J Clin Pharmacol . 1996;36(12):1132-1140.
- Bhasin S, Woodhouse L, Casaburi R, et al. Testosterone dose-response relationships in healthy young men. Am J Physiol Endocrinol Metab . 2001;281(6):E1172-1181.
- Linton MF, Yancey PG, Davies SS, Jerome WG (Jay), Linton EF, Vickers KC. The Role of Lipids and Lipoproteins in Atherosclerosis. In: De Groot LJ, Chrousos G, Dungan K, et al., eds. Endotext . South Dartmouth (MA): MDText.com, Inc.; 2000. https://www.ncbi.nlm.nih.gov/books/NBK343489/ . Accessed April 21, 2017.
- Robles-Diaz M, Gonzalez-Jimenez A, Medina-Caliz I, et al. Distinct phenotype of hepatotoxicity associated with illicit use of anabolic androgenic steroids. Aliment Pharmacol Ther . 2015;41(1):116-125. doi:10.1111/apt.13023.
- Schwingel PA, Cotrim HP, Santos CR dos, et al. Recreational Anabolic-Androgenic Steroid Use Associated With Liver Injuries Among Brazilian Young Men. Subst Use Misuse . 2015;50(11):1490-1498. doi:10.3109/10826084.2015.1018550.
- Kosaka A, Takahashi H, Yajima Y, et al. Hepatocellular carcinoma associated with anabolic steroid therapy: report of a case and review of the Japanese literature. J Gastroenterol . 1996;31(3):450-454.
- Socas L, Zumbado M, Pérez-Luzardo O, et al. Hepatocellular adenomas associated with anabolic androgenic steroid abuse in bodybuilders: a report of two cases and a review of the literature. Br J Sports Med . 2005;39(5):e27. doi:10.1136/bjsm.2004.013599.
- Wakabayashi T, Onda H, Tada T, Iijima M, Itoh Y. High incidence of peliosis hepatis in autopsy cases of aplastic anemia with special reference to anabolic steroid therapy. Acta Pathol Jpn . 1984;34(5):1079-1086.
- Hansma P, Diaz FJ, Njiwaji C. Fatal Liver Cyst Rupture Due to Anabolic Steroid Use: A Case Presentation. Am J Forensic Med Pathol . 2016;37(1):21-22. doi:10.1097/PAF.0000000000000218.
- Bonetti A, Tirelli F, Catapano A, et al. Side effects of anabolic androgenic steroids abuse. Int J Sports Med . 2008;29(8):679-687. doi:10.1055/s-2007-965808.
- Liu PY, Swerdloff RS, Christenson PD, Handelsman DJ, Wang C, Hormonal Male Contraception Summit Group. Rate, extent, and modifiers of spermatogenic recovery after hormonal male contraception: an integrated analysis. Lancet Lond Engl . 2006;367(9520):1412-1420. doi:10.1016/S0140-6736(06)68614-5.
- Torres-Calleja J, González-Unzaga M, DeCelis-Carrillo R, Calzada-Sánchez L, Pedrón N. Effect of androgenic anabolic steroids on sperm quality and serum hormone levels in adult male bodybuilders. Life Sci . 2001;68(15):1769-1774.
- Calzada L, Torres-Calleja J, Martinez JM, Pedrón N. Measurement of androgen and estrogen receptors in breast tissue from subjects with anabolic steroid-dependent gynecomastia. Life Sci . 2001;69(13):1465-1469.
- Christou MA, Christou PA, Markozannes G, Tsatsoulis A, Mastorakos G, Tigas S. Effects of Anabolic Androgenic Steroids on the Reproductive System of Athletes and Recreational Users: A Systematic Review and Meta-Analysis. Sports Med Auckl NZ . March 2017. doi:10.1007/s40279-017-0709-z.
- Schürmeyer T, Knuth UA, Belkien L, Nieschlag E. Reversible azoospermia induced by the anabolic steroid 19-nortestosterone. Lancet Lond Engl . 1984;1(8374):417-420.
- Orlandi MA, Venegoni E, Pagani C. Gynecomastia in two young men with histories of prolonged use of anabolic androgenic steroids. J Ultrasound . 2010;13(2):46-48. doi:10.1016/j.jus.2010.07.006.
- Chimento A, Sirianni R, Zolea F, et al. Nandrolone and stanozolol induce Leydig cell tumor proliferation through an estrogen-dependent mechanism involving IGF-I system. J Cell Physiol . 2012;227(5):2079-2088. doi:10.1002/jcp.22936.
- Baker J. A report on alterations to the speaking and singing voices of four women following hormonal therapy with virilizing agents. J Voice Off J Voice Found . 1999;13(4):496-507.
- Scott MJ, Scott AM. Effects of anabolic-androgenic steroids on the pilosebaceous unit. Cutis . 1992;50(2):113-116.
- Nieschlag E, Vorona E. MECHANISMS IN ENDOCRINOLOGY: Medical consequences of doping with anabolic androgenic steroids: effects on reproductive functions. Eur J Endocrinol Eur Fed Endocr Soc . 2015;173(2):R47-58. doi:10.1530/EJE-15-0080.
- Zemel BS, Katz SH. The contribution of adrenal and gonadal androgens to the growth in height of adolescent males. Am J Phys Anthropol . 1986;71(4):459-466. doi:10.1002/ajpa.1330710409.
- Bierich JR. Effects and side effects of anabolic steroids in children. Acta Endocrinol Suppl (Copenh) . 1961;39(Suppl 63):89-110.
- Seynnes OR, Kamandulis S, Kairaitis R, et al. Effect of androgenic-anabolic steroids and heavy strength training on patellar tendon morphological and mechanical properties. J Appl Physiol Bethesda Md 1985 . 2013;115(1):84-89. doi:10.1152/japplphysiol.01417.2012.
- Kraus SL, Emmert S, Schön MP, Haenssle HA. The dark side of beauty: acne fulminans induced by anabolic steroids in a male bodybuilder. Arch Dermatol . 2012;148(10):1210-1212. doi:10.1001/archdermatol.2012.855.
- Melnik B, Jansen T, Grabbe S. Abuse of anabolic-androgenic steroids and bodybuilding acne: an underestimated health problem. J Dtsch Dermatol Ges J Ger Soc Dermatol JDDG . 2007;5(2):110-117. doi:10.1111/j.1610-0387.2007.06176.x.
- Voelcker V, Sticherling M, Bauerschmitz J. Severe ulcerated “bodybuilding acne” caused by anabolic steroid use and exacerbated by isotretinoin. Int Wound J . 2010;7(3):199-201. doi:10.1111/j.1742-481X.2010.00676.x.
- Rich JD, Dickinson BP, Flanigan TP, Valone SE. Abscess related to anabolic-androgenic steroid injection. Med Sci Sports Exerc . 1999;31(2):207-209.
- Cabb E, Baltar S, Powers DW, Mohan K, Martinez A, Pitts E. The Diagnosis and Manifestations of Liver Injury Secondary to Off-Label Androgenic Anabolic Steroid Use. Case Rep Gastroenterol . 2016;10(2):499-505. doi:10.1159/000448883.
- Yoshida EM, Erb SR, Scudamore CH, Owen DA. Severe cholestasis and jaundice secondary to an esterified testosterone, a non-C17 alkylated anabolic steroid. J Clin Gastroenterol . 1994;18(3):268-270.
- Ip EJ, Yadao MA, Shah BM, Lau B. Infectious disease, injection practices, and risky sexual behavior among anabolic steroid users. AIDS Care . 2016;28(3):294-299. doi:10.1080/09540121.2015.1090539.
- Hughes TK, Fulep E, Juelich T, Smith EM, Stanton GJ. Modulation of immune responses by anabolic androgenic steroids. Int J Immunopharmacol . 1995;17(11):857-863.
- Perry PJ, Kutscher EC, Lund BC, Yates WR, Holman TL, Demers L. Measures of aggression and mood changes in male weightlifters with and without androgenic anabolic steroid use. J Forensic Sci . 2003;48(3):646-651.
- Lundholm L, Frisell T, Lichtenstein P, Långström N. Anabolic androgenic steroids and violent offending: confounding by polysubstance abuse among 10,365 general population men. Addict Abingdon Engl . 2015;110(1):100-108. doi:10.1111/add.12715.
- Burnett KF, Kleiman ME. Psychological characteristics of adolescent steroid users. Adolescence . 1994;29(113):81-89.
- Choi PY, Pope HG. Violence toward women and illicit androgenic-anabolic steroid use. Ann Clin Psychiatry Off J Am Acad Clin Psychiatr . 1994;6(1):21-25.
- Daly RC, Su T-P, Schmidt PJ, Pagliaro M, Pickar D, Rubinow DR. Neuroendocrine and behavioral effects of high-dose anabolic steroid administration in male normal volunteers. Psychoneuroendocrinology . 2003;28(3):317-331.
- Kouri EM, Lukas SE, Pope HG, Oliva PS. Increased aggressive responding in male volunteers following the administration of gradually increasing doses of testosterone cypionate. Drug Alcohol Depend . 1995;40(1):73-79.
- Bahrke MS, Yesalis CE, Wright JE. Psychological and behavioural effects of endogenous testosterone and anabolic-androgenic steroids. An update. Sports Med Auckl NZ . 1996;22(6):367-390.
- Tricker R, Casaburi R, Storer TW, et al. The effects of supraphysiological doses of testosterone on angry behavior in healthy eugonadal men--a clinical research center study. J Clin Endocrinol Metab . 1996;81(10):3754-3758. doi:10.1210/jcem.81.10.8855834.
- Ip EJ, Lu DH, Barnett MJ, Tenerowicz MJ, Vo JC, Perry PJ. Psychological and physical impact of anabolic-androgenic steroid dependence. Pharmacotherapy . 2012;32(10):910-919. doi:10.1002/j.1875-9114.2012.01123.
- Pope HG, Katz DL. Psychiatric and medical effects of anabolic-androgenic steroid use. A controlled study of 160 athletes. Arch Gen Psychiatry . 1994;51(5):375-382.
- Kanayama G, Pope HG. Illicit use of androgens and other hormones: recent advances. Curr Opin Endocrinol Diabetes Obes . 2012;19(3):211-219. doi:10.1097/MED.0b013e3283524008.
- Kanayama G, Cohane GH, Weiss RD, Pope HG. Past anabolic-androgenic steroid use among men admitted for substance abuse treatment: an underrecognized problem? J Clin Psychiatry . 2003;64(2):156-160.
- Wines JD, Gruber AJ, Pope HG, Lukas SE. Nalbuphine hydrochloride dependence in anabolic steroid users. Am J Addict . 1999;8(2):161-164.
- Arvary D, Pope HG. Anabolic-androgenic steroids as a gateway to opioid dependence. N Engl J Med . 2000;342(20):1532. doi:10.1056/NEJM200005183422018.
- Keenan BS, Richards GE, Ponder SW, Dallas JS, Nagamani M, Smith ER. Androgen-stimulated pubertal growth: the effects of testosterone and dihydrotestosterone on growth hormone and insulin-like growth factor-I in the treatment of short stature and delayed puberty. J Clin Endocrinol Metab . 1993;76(4):996-1001. doi:10.1210/jcem.76.4.8473416.
- Morris JA, Jordan CL, Breedlove SM. Sexual differentiation of the vertebrate nervous system. Nat Neurosci . 2004;7(10):1034-1039. doi:10.1038/nn1325.
- Romeo RD, Richardson HN, Sisk CL. Puberty and the maturation of the male brain and sexual behavior: recasting a behavioral potential. Neurosci Biobehav Rev . 2002;26(3):381-391.
- Schulz KM, Molenda-Figueira HA, Sisk CL. Back to the future: The organizational-activational hypothesis adapted to puberty and adolescence. Horm Behav . 2009;55(5):597-604. doi:10.1016/j.yhbeh.2009.03.010.
- Zehr JL, Nichols LR, Schulz KM, Sisk CL. Adolescent development of neuron structure in dentate gyrus granule cells of male Syrian hamsters. Dev Neurobiol . 2008;68(14):1517-1526. doi:10.1002/dneu.20675.
- Cunningham RL, Claiborne BJ, McGinnis MY. Pubertal exposure to anabolic androgenic steroids increases spine densities on neurons in the limbic system of male rats. Neuroscience . 2007;150(3):609-615. doi:10.1016/j.neuroscience.2007.09.038.
- Hildebrandt T, Langenbucher JW, Flores A, Harty S, Berlin HA, Berlin H. The influence of age of onset and acute anabolic steroid exposure on cognitive performance, impulsivity, and aggression in men. Psychol Addict Behav J Soc Psychol Addict Behav . 2014;28(4):1096-1104. doi:10.1037/a0036482.
- Olivares EL, Silveira ALB, Fonseca FV, et al. Administration of an anabolic steroid during the adolescent phase changes the behavior, cardiac autonomic balance and fluid intake in male adult rats. Physiol Behav . 2014;126:15-24. doi:10.1016/j.physbeh.2013.12.006.
- Grimes JM, Melloni RH. Prolonged alterations in the serotonin neural system following the cessation of adolescent anabolic-androgenic steroid exposure in hamsters (Mesocricetus auratus). Behav Neurosci . 2006;120(6):1242-1251. doi:10.1037/0735-7044.120.6.1242.
- Ricci LA, Rasakham K, Grimes JM, Melloni RH. Serotonin-1A receptor activity and expression modulate adolescent anabolic/androgenic steroid-induced aggression in hamsters. Pharmacol Biochem Behav . 2006;85(1):1-11. doi:10.1016/j.pbb.2006.06.022.
- Menard CS, Harlan RE. Up-regulation of androgen receptor immunoreactivity in the rat brain by androgenic-anabolic steroids. Brain Res . 1993;622(1-2):226-236.
- Matsumoto T, Sakari M, Okada M, et al. The androgen receptor in health and disease. Annu Rev Physiol . 2013;75:201-224. doi:10.1146/annurev-physiol-030212-183656.
- Vicencio JM, Estrada M, Galvis D, et al. Anabolic androgenic steroids and intracellular calcium signaling: a mini review on mechanisms and physiological implications. Mini Rev Med Chem . 2011;11(5):390-398.
- Yang P, Jones BL, Henderson LP. Mechanisms of anabolic androgenic steroid modulation of alpha(1)beta(3)gamma(2L) GABA(A) receptors. Neuropharmacology . 2002;43(4):619-633.
- Yang P, Jones BL, Henderson LP. Role of the alpha subunit in the modulation of GABA(A) receptors by anabolic androgenic steroids. Neuropharmacology . 2005;49(3):300-316. doi:10.1016/j.neuropharm.2005.03.017.
- Kindlundh AM, Lindblom J, Bergström L, Wikberg JE, Nyberg F. The anabolic-androgenic steroid nandrolone decanoate affects the density of dopamine receptors in the male rat brain. Eur J Neurosci . 2001;13(2):291-296.
- Thiblin I, Finn A, Ross SB, Stenfors C. Increased dopaminergic and 5-hydroxytryptaminergic activities in male rat brain following long-term treatment with anabolic androgenic steroids. Br J Pharmacol . 1999;126(6):1301-1306. doi:10.1038/sj.bjp.0702412.
- Zotti M, Tucci P, Colaianna M, et al. Chronic nandrolone administration induces dysfunction of the reward pathway in rats. Steroids . 2014;79:7-13.
- Kanayama G, Brower KJ, Wood RI, Hudson JI, Pope HG. Issues for DSM-V: clarifying the diagnostic criteria for anabolic-androgenic steroid dependence. Am J Psychiatry . 2009;166(6):642-645. doi:10.1176/appi.ajp.2009.08111699.
- Brower KJ, Blow FC, Young JP, Hill EM. Symptoms and correlates of anabolic-androgenic steroid dependence. Br J Addict . 1991;86(6):759-768.
- Malone DA, Dimeff RJ, Lombardo JA, Sample RH. Psychiatric effects and psychoactive substance use in anabolic-androgenic steroid users. Clin J Sport Med Off J Can Acad Sport Med . 1995;5(1):25-31.
- 2015 Anti-Doping Rule Violations (ADRVs) Report .; 2017. https://www.wada-ama.org/sites/default/files/resources/files/2015_adrvs_report_web_release_0.pdf .
- Compliance Monitoring. https://www.wada-ama.org/en/what-we-do/compliance-monitoring/compliance-monitoring-program . Published 2017. Accessed May 18, 2017.
- Geyer H, Schänzer W, Thevis M. Anabolic agents: recent strategies for their detection and protection from inadvertent doping. Br J Sports Med . 2014;48(10):820-826. doi:10.1136/bjsports-2014-093526.
- Catlin DH, Sekera MH, Ahrens BD, Starcevic B, Chang Y-C, Hatton CK. Tetrahydrogestrinone: discovery, synthesis, and detection in urine. Rapid Commun Mass Spectrom RCM . 2004;18(12):1245-1049. doi:10.1002/rcm.1495.
- Catlin DH, Ahrens BD, Kucherova Y. Detection of norbolethone, an anabolic steroid never marketed, in athletes’ urine. Rapid Commun Mass Spectrom RCM . 2002;16(13):1273-1275. doi:10.1002/rcm.722.
- Sekera MH, Ahrens BD, Chang Y-C, Starcevic B, Georgakopoulos C, Catlin DH. Another designer steroid: discovery, synthesis, and detection of “madol” in urine. Rapid Commun Mass Spectrom RCM . 2005;19(6):781-784. doi:10.1002/rcm.1858.
- Mareck U, Geyer H, Opfermann G, Thevis M, Schänzer W. Factors influencing the steroid profile in doping control analysis. J Mass Spectrom JMS . 2008;43(7):877-891. doi:10.1002/jms.1457.
- Yonamine M, Garcia PR, de Moraes Moreau RL. Non-intentional doping in sports. Sports Med Auckl NZ . 2004;34(11):697-704.
- Jung J, Hermanns-Clausen M, Weinmann W. Anorectic sibutramine detected in a Chinese herbal drug for weight loss. Forensic Sci Int . 2006;161(2-3):221-222. doi:10.1016/j.forsciint.2006.02.052.
- Parr MK, Koehler K, Geyer H, Guddat S, Schänzer W. Clenbuterol marketed as dietary supplement. Biomed Chromatogr BMC . 2008;22(3):298-300. doi:10.1002/bmc.928.
- Geyer H, Braun H, Burke LM, Stear SJ, Castell LM. A-Z of nutritional supplements: dietary supplements, sports nutrition foods and ergogenic aids for health and performance--Part 22. Br J Sports Med . 2011;45(9):752-754. doi:10.1136/bjsports-2011-090180.
- De Cock KJ, Delbeke FT, Van Eenoo P, Desmet N, Roels K, De Backer P. Detection and determination of anabolic steroids in nutritional supplements. J Pharm Biomed Anal . 2001;25(5-6):843-852.
- Tainted Products Marketed as Dietary Supplements. https://www.accessdata.fda.gov/scripts/sda/sdNavigation.cfm?sd=tainted_supplements_cder . Accessed January 9, 2018.
- World Anti-Doping Code. 2009. https://www.wada-ama.org/sites/default/files/resources/files/wada_anti-doping_code_2009_en_0.pdf . Accessed May 23, 2017.
- Elliot D, Goldberg L. Intervention and prevention of steroid use in adolescents. Am J Sports Med . 1996;24(6 Suppl):S46-47.
- Goldberg L, Bents R, Bosworth E, Trevisan L, Elliot DL. Anabolic steroid education and adolescents: do scare tactics work? Pediatrics . 1991;87(3):283-286.
- Middleman AB, Faulkner AH, Woods ER, Emans SJ, DuRant RH. High-risk behaviors among high school students in Massachusetts who use anabolic steroids. Pediatrics . 1995;96(2 Pt 1):268-272.
- Goldberg L, MacKinnon DP, Elliot DL, Moe EL, Clarke G, Cheong J. The adolescents training and learning to avoid steroids program: preventing drug use and promoting health behaviors. Arch Pediatr Adolesc Med . 2000;154(4):332-338.
- Elliot DL, Goldberg L, Moe EL, Defrancesco CA, Durham MB, Hix-Small H. Preventing substance use and disordered eating: initial outcomes of the ATHENA (athletes targeting healthy exercise and nutrition alternatives) program. Arch Pediatr Adolesc Med . 2004;158(11):1043-1049. doi:10.1001/archpedi.158.11.1043.
- Elliot DL, Goldberg L, Moe EL, et al. Long-term Outcomes of the ATHENA (Athletes Targeting Healthy Exercise & Nutrition Alternatives) Program for Female High School Athletes. J Alcohol Drug Educ . 2008;52(2):73-92.
- Pope HG, Kanayama G, Ionescu-Pioggia M, Hudson JI. Anabolic steroid users’ attitudes towards physicians. Addict Abingdon Engl . 2004;99(9):1189-1194. doi:10.1111/j.1360-0443.2004.00781.x.
- Brennan BP, Kanayama G, Pope HG. Performance-enhancing drugs on the web: a growing public-health issue. Am J Addict Am Acad Psychiatr Alcohol Addict . 2013;22(2):158-161. doi:10.1111/j.1521-0391.2013.00311.x.
- Kanayama G, Brower KJ, Wood RI, Hudson JI, Pope HG. Treatment of anabolic-androgenic steroid dependence: Emerging evidence and its implications. Drug Alcohol Depend . 2010;109(1-3):6-13. doi:10.1016/j.drugalcdep.2010.01.011

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- My Bibliography
- Collections
- Citation manager
Save citation to file
Email citation, add to collections.
- Create a new collection
- Add to an existing collection
Add to My Bibliography
Your saved search, create a file for external citation management software, your rss feed.
- Search in PubMed
- Search in NLM Catalog
- Add to Search
From a single steroid to the steroidome: Trends and analytical challenges
Affiliations.
- 1 Institute of Pharmaceutical Sciences of Western Switzerland, University of Geneva, Switzerland; School of Pharmaceutical Sciences, University of Geneva, Switzerland; Swiss Centre for Applied Human Toxicology (SCAHT), Switzerland.
- 2 Institute of Pharmaceutical Sciences of Western Switzerland, University of Geneva, Switzerland; School of Pharmaceutical Sciences, University of Geneva, Switzerland.
- 3 Institute of Pharmaceutical Sciences of Western Switzerland, University of Geneva, Switzerland. Electronic address: [email protected].
- PMID: 33259940
- DOI: 10.1016/j.jsbmb.2020.105797
For several decades now, the analysis of steroids has been a key tool in the diagnosis and monitoring of numerous endocrine pathologies. Thus, the available methods used to analyze steroids in biological samples have dramatically evolved over time following the rapid pace of technology and scientific knowledge. This review aims to synthetize the advances in steroids' analysis, from classical approaches considering only a few steroids or a limited number of steroid ratios, up to the new steroid profiling strategies (steroidomics) monitoring large sets of steroids in biological matrices. In this context, the use of liquid chromatography coupled to mass spectrometry has emerged as the technique of choice for the simultaneous determination of a high number of steroids, including phase II metabolites, due to its sensitivity and robustness. However, the large dynamic range to be covered, the low natural abundance of some key steroids, the selectivity of the analytical methods, the extraction protocols, and the steroid ionization remain some of the current challenges in steroid analysis. This review provides an overview of the different analytical workflows available depending on the number of steroids under study. Special emphasis is given to sample treatment, acquisition strategy, data processing, steroid identification and quantification using LC-MS approaches. This work also outlines how the availability of steroid standards, the need for complementary analytical strategies and the improvement of calibration approaches are crucial for achieving complete steroidome quantification.
Keywords: Challenges; Quantification; Relative estimation; Steroid analysis; Steroidome.
Copyright © 2020 The Author(s). Published by Elsevier Ltd.. All rights reserved.
PubMed Disclaimer
Similar articles
- Comprehensive steroid profiling by liquid chromatography coupled to high resolution mass spectrometry. Kaabia Z, Laparre J, Cesbron N, Le Bizec B, Dervilly-Pinel G. Kaabia Z, et al. J Steroid Biochem Mol Biol. 2018 Oct;183:106-115. doi: 10.1016/j.jsbmb.2018.06.003. Epub 2018 Jul 3. J Steroid Biochem Mol Biol. 2018. PMID: 30196848
- Multiplexed steroid profiling of gluco- and mineralocorticoids pathways using a liquid chromatography tandem mass spectrometry method. Travers S, Martinerie L, Bouvattier C, Boileau P, Lombès M, Pussard E. Travers S, et al. J Steroid Biochem Mol Biol. 2017 Jan;165(Pt B):202-211. doi: 10.1016/j.jsbmb.2016.06.005. Epub 2016 Jun 23. J Steroid Biochem Mol Biol. 2017. PMID: 27339652
- Evaluation of steroidomics by liquid chromatography hyphenated to mass spectrometry as a powerful analytical strategy for measuring human steroid perturbations. Jeanneret F, Tonoli D, Rossier MF, Saugy M, Boccard J, Rudaz S. Jeanneret F, et al. J Chromatogr A. 2016 Jan 22;1430:97-112. doi: 10.1016/j.chroma.2015.07.008. Epub 2015 Jul 7. J Chromatogr A. 2016. PMID: 26195035 Review.
- Profiling intact steroid sulfates and unconjugated steroids in biological fluids by liquid chromatography-tandem mass spectrometry (LC-MS-MS). Galuska CE, Hartmann MF, Sánchez-Guijo A, Bakhaus K, Geyer J, Schuler G, Zimmer KP, Wudy SA. Galuska CE, et al. Analyst. 2013 Jul 7;138(13):3792-801. doi: 10.1039/c3an36817c. Analyst. 2013. PMID: 23671909
- Ultra high performance liquid chromatography tandem mass spectrometry determination and profiling of prohibited steroids in human biological matrices. A review. Gosetti F, Mazzucco E, Gennaro MC, Marengo E. Gosetti F, et al. J Chromatogr B Analyt Technol Biomed Life Sci. 2013 May 15;927:22-36. doi: 10.1016/j.jchromb.2012.12.003. Epub 2012 Dec 20. J Chromatogr B Analyt Technol Biomed Life Sci. 2013. PMID: 23317577 Review.
- C11-hydroxy and C11-oxo C 19 and C 21 Steroids: Pre-Receptor Regulation and Interaction with Androgen and Progesterone Steroid Receptors. Gent R, Van Rooyen D, Atkin SL, Swart AC. Gent R, et al. Int J Mol Sci. 2023 Dec 20;25(1):101. doi: 10.3390/ijms25010101. Int J Mol Sci. 2023. PMID: 38203272 Free PMC article.
- The steroid hormone ADIOL promotes learning by reducing neural kynurenic acid levels. Lemieux GA, Yoo S, Lin L, Vohra M, Ashrafi K. Lemieux GA, et al. Genes Dev. 2023 Dec 26;37(21-24):998-1016. doi: 10.1101/gad.350745.123. Genes Dev. 2023. PMID: 38092521 Free PMC article.
- Differentiation of steroid isomers by steroid analogues adducted trapped ion mobility spectrometry-mass spectrometry. Li Y, Qin Y, Wei S, Ling L, Ding CF. Li Y, et al. Anal Bioanal Chem. 2024 Jan;416(1):313-319. doi: 10.1007/s00216-023-05019-5. Epub 2023 Nov 8. Anal Bioanal Chem. 2024. PMID: 37940728
- Simultaneous extraction and detection of peptides, steroids, and proteins in small tissue samples. Lu C, Peng D, Erandani WCKU, Mitchell K, Martyniuk CJ, Trudeau VL. Lu C, et al. Front Endocrinol (Lausanne). 2023 Oct 9;14:1266985. doi: 10.3389/fendo.2023.1266985. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37876537 Free PMC article.
- Ocular steroidome in human eyes and in eyes with complex central serous chorioretinopathy (CSCR). Zola M, Bousquet E, Bourges JL, Azan F, Zhao M, Jaworski T, Pussard E, Behar-Cohen F. Zola M, et al. Sci Rep. 2023 Aug 29;13(1):14111. doi: 10.1038/s41598-023-41126-0. Sci Rep. 2023. PMID: 37644063 Free PMC article.
Publication types
- Search in MeSH
LinkOut - more resources
Full text sources.
- Elsevier Science
Other Literature Sources
- scite Smart Citations
- MedlinePlus Health Information

- Citation Manager
NCBI Literature Resources
MeSH PMC Bookshelf Disclaimer
The PubMed wordmark and PubMed logo are registered trademarks of the U.S. Department of Health and Human Services (HHS). Unauthorized use of these marks is strictly prohibited.

- Get new issue alerts Get alerts
- Submit a Manuscript
Secondary Logo
Journal logo.
Colleague's E-mail is Invalid
Your message has been successfully sent to your colleague.
Save my selection
Steroids and immunotherapy
The good, bad, or the ugly.
Chandrasekharan, Arun; Sreelesh, K. P.; Gangadharan, K. V.
Department of Medical Oncology, Aster Malabar Institute of Medical Sciences, Kozhikode, Kerala, India
Address for correspondence: Dr. Arun Chandrasekharan, Department of Medical Oncology, Aster Malabar Institute of Medical Sciences, Mini Bypass Road, Govindapuram, Kozhikode - 673 016, Kerala, India. E-mail: [email protected]
Received December 31, 2019
Accepted January 08, 2020
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
The article by Kapoor et al . and the accompanying editorial highlight the important issue of the usage of corticosteroids along with immunotherapy in advanced cancers.[ 1 2 ]
The use of steroids with immunotherapy is inevitable in certain situations. With the approval of immunotherapy combined with chemotherapy as the best first-line option in advanced non-small cell lung cancer, the use of steroids as antiemetics becomes necessary. Similarly, with around 20% of patients presenting with brain metastasis, steroids form an integral part of treatment and their concurrent use with immunotherapy may be unavoidable.
It is a difficult question to answer, whether the use of steroids actually jeopardizes the efficacy of immunotherapy or selects out a group of patients with poor prognosis (brain metastases) or more aggressive disease who will not have any benefit with immunotherapy.
Banna et al. developed a tool for choosing between immunotherapy and chemotherapy in lung cancer and listed performance status ≧1, high neutrophil-to-lymphocyte ratio, and high-dose corticosteroids as unfavorable for immunotherapy.[ 3 ] Very recent data in a larger subset of patients using corticosteroids and immunotherapy were presented as an abstract at ESMO 2019.[ 4 ] A total of 146 patients received corticosteroids (the largest number thus far compared to other studies), and it was seen that the overall survival (OS) was longer in the group that did not receive steroids or <10 mg of steroids (14.7 vs. 8.3 months). However, there was no difference in progression-free survival. On multivariate analysis, the use of steroids was identified as an independent variable for poorer outcomes. The study also looked at the role of antibiotics affecting the efficacy of immunotherapy, and no significant correlation was found, with comparable OS. This is in opposition to the findings of Kapoor et al .,[ 1 ] which may be explained by the fact that the former study had many more patients (141) who received antibiotics versus fewer number of patients (27) in the latter study. However, how many out of these 141 patients received both steroids and antibiotics is not detailed in the abstract. The timing of antibiotics is also crucial as a recent study showed that antibiotic therapy administered before immunotherapy, not concurrently, was associated with worse response to treatment and OS.[ 5 ]
The studies discussed in the article by Kapoor et al. largely show a negative impact of steroids. The latest study from Europe also walks the same path although it may be due to the steroids selecting out patients with larger volume and more aggressive tumors. One must be prudent while using steroids with immunotherapy, and a risk–benefit assessment is essential before their use, especially in emergency situations such as brain metastases, where steroid use is unavoidable.
Financial support and sponsorship
Conflicts of interest.
There are no conflicts of interest.
- Cited Here |
- Google Scholar
- + Favorites
- View in Gallery
Readers Of this Article Also Read
Lenvatinib plus pembrolizumab for advanced endometrial cancer, alk</em> and <em xmlns:mrws=\"http://webservices.ovid.com/mrws/1.0\">egfr</em>) alterations', 'behel vichitra; noronha, vanita; patil, vijay; menon, nandini; chandrani, pratik; kumar, rajiv; rastogi, shivam; mahajan, abhishek; chougule, anuradha; dutt, amit; prabhash, kumar', 'cancer research, statistics, and treatment', 'apr-jun 2022', '5', '2' , 'p 312-316');" onmouseout="javascript:tooltip_mouseout()" class="ejp-uc__article-title-link">molecular tumor board–guided treatment of non-small-cell lung cancer with dual..., regorafenib: a narrative drug review, met</em>: a narrative review of exon 14 skipping mutation in non-small-cell lung carcinoma', 'nathany shrinidhi; batra, ullas', 'cancer research, statistics, and treatment', 'apr-jun 2022', '5', '2' , 'p 284-292');" onmouseout="javascript:tooltip_mouseout()" class="ejp-uc__article-title-link"> met : a narrative review of exon 14 skipping mutation in non-small-cell lung..., vaccination practices, efficacy, and safety in adults with cancer: a narrative ....

The Science of Steroids: The Physiology and Psychology of How Steroids Make You Stronger
- by Greg Nuckols
- Articles , Steroids
Steroids are a very taboo subject in our culture. They are Schedule III controlled substances in the U.S., meaning they are illegal to own without a prescription and illegal to distribute unless you are an MD. Furthermore, they are banned in almost all athletic competitions (with the exceptions being some untested strength sports). This is not meant to be read as an article condoning steroid use.
Steroids carry numerous short-term risks (high blood pressure, high cholesterol, liver toxicity, etc.), with the potential for long-term risks (atherosclerosis, infertility, hypogonadism, etc.) dependent on the particular compounds used, the dosages, and the duration you take them. Anyone who knows anything about steroids has probably heard about the risks they carry, so I’m not going to beat you over the head with that.
With that standard disclaimer out of the way, I still think steroids are worth having frank, open discussions about, for two main reasons.
- They’re really interesting.
- People are going to use anyway, so they may as well be informed.
In fact, as of 2002, 4% of high school students were willing to self-report that they had used steroids, and that number was trending upward. If I had to take a guess, that number is probably low since people are known to underreport their involvement in socially undesirable behavior, even if they know they’ll remain anonymous.
Other surveys indicate that between 1-3 million Americans use steroids . For context, there are about 60 million people with gym memberships in the country, and 2/3 of those people never go to the gym, taking the number of actual gymgoers down to about 20 million. If we assume that the people using steroids are actually working out, that means that between 1 in 20 and 1 in 6 people you see in the gym are on, or have at least tried, steroids. It’s hard to pin down an exact number because these types of surveys about illegal behavior are notoriously unreliable, but it’s safe to say that it’s certainly not a negligible proportion of the gym going population.
Odds are, whether they’re open about it or not, you know someone on steroids.
(If you’re interested in understanding the basic physiology of how steroids work, then just keep reading from here. If you already know it, or if it doesn’t interest you, skip ahead a couple of paragraphs to the subheading “Steroids work, in part, because you expect them to work.”)
The first question is, how do they work?
The mechanism of action for steroid hormones (like the anabolic steroids we’re talking about, though the same is true of any steroid hormone including cortisol, estrogen, aldosterone, etc.) is pretty straightforward. They’re lipid-soluble, so they can diffuse directly into a cell (rather than needing to bind to a receptor on the surface of the cell like peptide hormones – like insulin and IGF-1), bind to their particular steroid receptor, and go to the nucleus of the cell so they can influence gene transcription. Those transcribed genes determine what proteins are produced, and those proteins affect the structure and function of that cell.
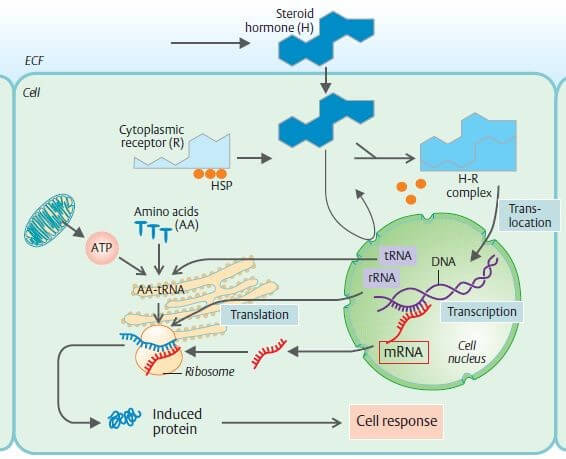
The steroids we’re talking about are mostly derivatives of testosterone (or similar hormones like DHT, though some like Deca-Durabolin are derivatives of progesterone), and have the same mechanism of action. They diffuse into the cell, bind to a receptor, influence gene transcription, and ultimately influence the proteins the cell produces. Different steroid hormones cause cells to produce different proteins, but in skeletal muscle, testosterone and its derivatives primarily increase the production of the actin and myosin that are the major proteins that make you strong and jacked.
Backing up a step, though, before these steroids can make their way into the muscle to have an effect, they have to actually travel in the blood to the muscle.
So the first issue is getting those steroids into your blood. Routes of administration that don’t involve digestion tend to be the safest for your liver, including injections and transdermal administration (like Androgel). Oral steroids have to be modified so your liver can’t immediately excrete them – things you swallow are absorbed, and they then must pass through your liver before they can make it to general circulation. Your liver isn’t particularly keen to pass high doses of steroid hormones directly to general circulation, so it will break them down into non-bioactive metabolites unless they’re modified to resist this process. Because of this, your liver tends to have to work quite a bit harder to handle orals than injectables, so orals tend to be more damaging to your liver. There are orals that aren’t very hepatotoxic (damaging to your liver), and there are injectables that are quite hepatotoxic, but since this post isn’t meant to be a how-to guide for steroid use, recognize I’m painting in broad strokes here.
Now that the steroids are in your blood (either by direct injection, or because they survived their first pass through the liver), they need to make it to your muscles.
Most testosterone in your body is bound to proteins in your blood, most notably albumin and sex hormone binding globulin (SHBG). If you get your testosterone levels checked, the lab should report total testosterone and free testosterone. The free testosterone is the stuff that’s most available to diffuse into your cells and affect the body.
This is a key point and is the main reason why steroids don’t seem to have much effect until they’re taken in supraphysiological doses – presenting your body with a concentration it wouldn’t experience in normal circumstances. When you don’t have any major endocrine problems and your testosterone levels are within the normal physiological range, your body will produce more or less binding proteins to make sure you have the right amount of free testosterone – not too little, and not too much.
Your body can’t just jack up albumin production because it plays a critical role in keeping fluid concentrations stable between your cells and the extracellular fluid, and while SHBG levels increase when you introduce high levels of some exogenous steroid hormones into the body (including estrogen, which is a major reason many women experience loss of sex drive when they go on birth control – increased SHBG binds more of their precious, tiny amounts of testosterone that are so important for sex drive), testosterone actually decreases SHBG levels slightly for reasons I admittedly don’t quite understand.
This is the main reason why over-the-counter “testosterone boosters” don’t work for building mass and strength if you have normal testosterone levels, and steroids work really, really well. Even if your test booster increases your testosterone by 40% like it claims, you’re still relying on your testes to produce it, and they simply won’t pump out enough to push you to supraphysiological concentrations to outrun the effects of the binding proteins. You could have 40% more testosterone but the same free testosterone.
So, this was a long way of explaining why steroids “work.” You put enough of a hormone into the body that the body’s normal regulatory mechanisms can’t quite cope, so you wind up with more free androgens to make it to your muscles and make you jacked.
This is quite a bit more dry physiology than I like going into, but I think it’s important to cover because a lot of people are ignorant of it, and it can help provide a basic backdrop of understanding for discussions about steroids.
Of course, an article basically saying “steroids make you strong, and here’s the physiology behind why steroids work,” really wouldn’t be saying much that’s relevant to you. So now it’s time to actually delve into the fun stuff.
Steroids work, in part, because you expect them to work.
Let’s take a look at two studies examining the placebo effect’s impact on “steroid-induced” strength gains.
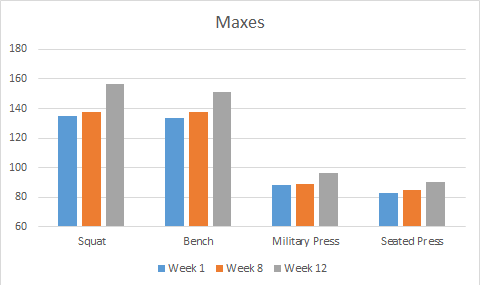
In the first ( Ariel, 1974 ), researchers told 15 trained athletes they could get their hands on some free, legal steroids. The subjects were already relatively strong at the start of the study – with squat and bench press maxes around 300 pounds, and military press maxes a shade under 200 pounds.
They trained for 7 weeks with the promise that the people who made the best strength gains (to give them an incentive to train hard and make as much progress as possible) in those 7 weeks would get free, legal steroids. So the athletes trained for 7 weeks, and put a combined total of ~22 pounds on their bench, military press, seated press, and squat.
Then, 6 of the participants were selected at random to take part in the “steroid” trial. They were told they were being given 10mg/day of Dianabol, when really they were taking placebo pills.
They trained for another 4 weeks, thinking they were on drugs.
In just 4 weeks, they put a combined total of ~100 pounds on those same four lifts. 100 pounds instead of 22, in 4 weeks instead of 7. Simply because they THOUGHT they were on steroids.
So the placebo effect clearly increases your strength gains from training when you simply *think* you’re on steroids. You expect more gains, so you get more gains.
However, what about lifting more today ?
For that we turn to another study ( Maganaris, 2000 ).
In this one, the researchers were in a perfect position to study the placebo effect. The researchers were coaching a powerlifting team, and the eleven members of the team actually asked their coaches about using steroids. Presumably they trusted their coaches, so when their coaches told the lifters they were providing them with fast-acting steroids, the lifters bought it hook, line, and sinker.
Their coaches gave them saccharine pills, telling them they were steroids. Then they maxed out on squat, bench, and deadlift.
An important thing to note is that these were all nationally ranked powerlifters. The average bodyweight was around 85kg, with average maxes of 257kg squat, 207kg bench, and 260kg deadlift (566 squat, 456 bench, 573 deadlift at ~187 pounds). Based on how close the bench is to the squat and deadlift, I’m assuming they were lifting in powerlifting gear, but I’m not positive. However, they weren’t new lifters – these guys were really strong.
When they maxed, thinking they were on steroids, every single one of them hit PRs on every lift. The smallest PR on any lift was 5kg. Most were 10 or 12.5kg PRs. These PRs represented 4-5% improvements on their maxes, taking their 724kg average total to ~755kg (1597 pounds to ~1670).
After that, they trained for two more weeks, continuing to think they were on steroids.
After these two weeks of training, they were asked how their training had been going. All of them reported that they’d been lifting heavier weights, lifting the same weights for more reps, and generally feeling more energetic and having better training sessions.
Then they maxed again. However, the coaches put a twist on it. 6 of the lifters were allowed to continue believing they were on steroids. 5, however, were told they had been taking a placebo the whole time.
The results were astounding.
The group that continued to believe they were on steroids stayed at about the same level they had reached two weeks prior. There were a few small regressions and a few small new PRs, but on the whole they held onto the 4-5% extra strength they’d gained by thinking they were on steroids.
The group that was informed they’d been taking a placebo absolutely tanked. Their maxes essentially returned to their pre-placebo baseline. None of them could hit a single lift that equaled what they’d done two weeks prior. This is IN SPITE OF knowing they hadn’t been taking steroids when they had hit PRs two weeks before, and in spite of reporting better training for the two intervening weeks. As soon as the mental crutch was removed, they couldn’t perform on the same level, even though they knew the initial PRs and the two good weeks of training were just the result of their hard work – not drugs.
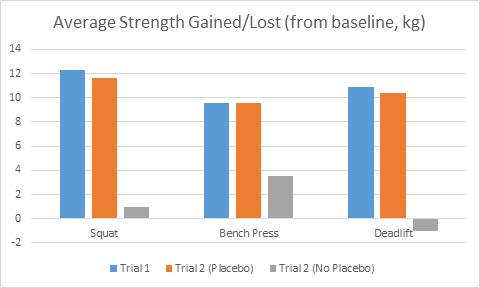
So from these two studies we see a piece of why steroids are so effective. On top of how well they work physiologically, when people go on steroids, they THINK they’re going to get a ton stronger. They can lift more weight just by thinking they’re on, and they’ll gain more strength from training just by thinking they’re on. Part of the reason steroids work so well is that you expect them to work so well.
Of course, the effects of steroids aren’t just all in your head. They do, very much, work .
Let’s take a look at a major study ( Bashin, 1996 ) that confirmed what bodybuilders had known for years – namely that supraphysiological doses of testosterone work really really well for building size and strength.
The subjects were split into 4 groups. One group was given a placebo (sesame seed oil injection instead of a testosterone injection) and didn’t lift. One group was given testosterone and didn’t lift. One group was given a placebo and lifted. The last group was given testosterone and lifted.
They maxed on bench press and squat at the beginning and end of the 10 week program. The program itself was a mix of DUP and linear progression, by the sound of it – pretty decent programming if you’re trying to get people bigger and stronger.
The results:

Yes, you’re reading that chart correctly. The group that took a placebo and worked out only gained slightly more strength than the group that took testosterone and sat on the couch for 10 weeks. The group that took testosterone without exercise gained just as much, if not more, muscle mass than the people taking a placebo and actually working out.
Keep in mind, the dose for this study was 600mg/week of testosterone with nothing else added in. This wasn’t a several-grams-per-week pro bodybuilder steroid stack. This was a fairly low dose that might represent someone sticking their pinky toe into the world of steroids.
So for people who say, “oh, steroids don’t make you bigger and stronger. They just let you work harder,” I’m sad to inform you that such a statement is patently false . They may help with recovery and let you work harder, but I guarantee you that you could stick with the exact training routine you have now, start taking steroids, and gain more size and strength from it – no extra work required. And an untrained person might (would probably) gain more muscle from just taking steroids than they would if they actually worked out.
Clearly, steroids make you stronger and bigger. But how much of an advantage do they actually provide for sports?
For sports where absolute strength and size are paramount, they give a huge advantage: The superheavyweight class of any sport where you can weigh as much as you want comes to mind. Powerlifters, weightlifters, and strongmen in the very top weight division. Obviously bodybuilding and physique sports as well.
For everything else – I think they help, but not to the degree people would like to make it seem, and not at super high doses.
Most sports, at their core, are about producing as much force as possible relative to your bodyweight, while effectively meeting the energetic demands of the sport. The “relative to your bodyweight” piece is the part I’d like to hone in on.
You see, steroids don’t directly make you stronger. They directly make you bigger. They cause your muscles to synthesize more protein, but there’s more to strength than muscle protein accretion. There is a relationship between “bigger” and “stronger” (obviously), but the relationship isn’t 1 to 1.
(edit: the statement “they don’t directly make you stronger” may not be entirely true. Testosterone does have nervous system effects that could directly improve strength output, and many lifters report substantial acute benefits of various fast-acting oral compounds due to mood alteration and lowering of central inhibition. However, the former works on a slightly longer time scale compared to muscle protein synthesis, and the latter DOES probably contribute, but there’s no research to determine how effective orals are at altering mood, perception, and expectancy relative to placebos. Thanks to Dr. Mike Israetel for the catch.)
Especially in sports with weight classes, added muscle mass isn’t good for much if your strength doesn’t increase at the same rate. At least based on the scant research available, it looks like it may be the case that if you take too high of a dose, it’ll actually hinder your performance by increasing your mass much more than your strength.
The first place I’d like to look is at a study examining the effects of different doses of testosterone. Participants’ natural testosterone production was slowed down, and then they were given test in doses ranging from 25mg/week (really really low) to 600mg/week (well above the physiological range).
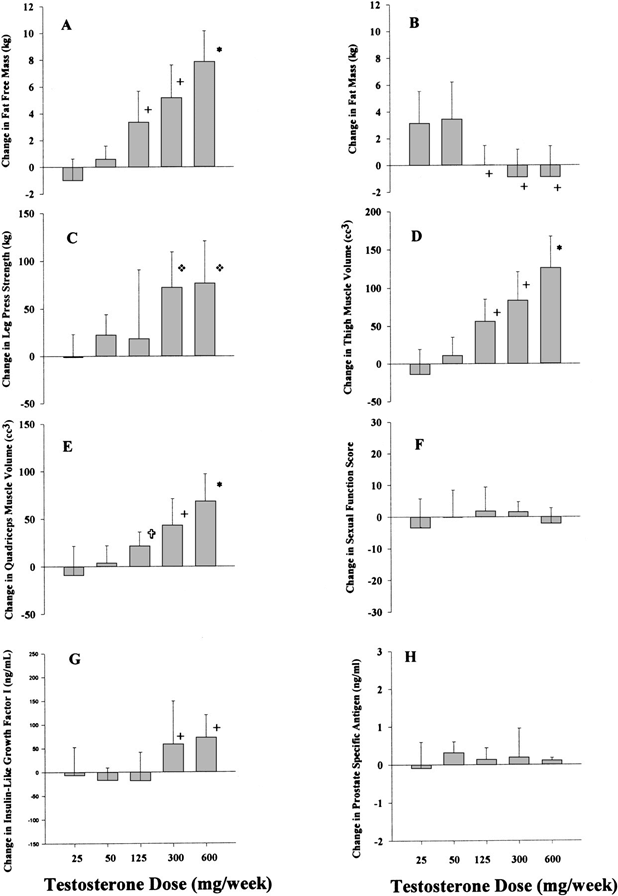
Gain in muscle size was quite linear. However, gains in strength were not. The 300mg/week group got nearly the exact same strength gains as the 600mg/week group, but with less hypertrophy (about 5 pounds less fat free mass). Over time, this could potentially mean lower force output relative to bodyweight for the group taking a higher dose.
This notion is borne out in further research ( Yu, 2014 ), comparing strength and muscle characteristics between lifetime drug free lifters and long-term steroid users. In this study, the steroid users had larger legs and more lean mass, but the drug free lifters squatted considerably more relative to lean body mass and leg muscle volume. Each pound of leg muscle for the drug free lifters could produce more force than a pound of leg muscle for the steroid users.
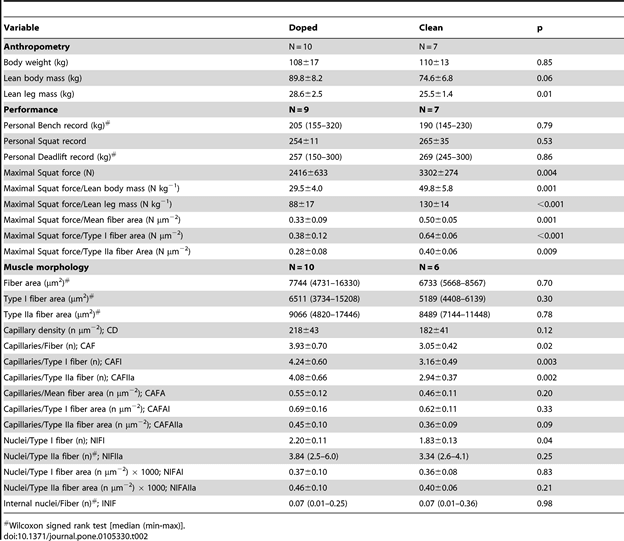
Of course, in this study, a confounding factor is training histories. Due to ethical constraints, there was no intervention – it was merely an observational study. The drug free lifters were all weightlifters or powerlifters, whereas the steroid users included a mix of lifters, strongmen, and bodybuilders. So it could simply be that the differences could be attributable to the sport-specific training, not the drugs. Because the difference was SO profound, though (almost 50% higher force output per pound of leg muscle in the drug free lifters), I don’t think we can chalk it all up to training.
However, I’m not entirely sure WHY someone would be stronger, relatively, if they built their muscle without drugs. Maybe the rapid protein synthesis and decrease in protein breakdown doesn’t allow for effective remodeling. Maybe muscle strength increases faster than tendon strength, so sensory mechanisms like the golgi tendon organ don’t allow the muscles to contract maximally. Maybe the muscle is being built so fast that neural factors simply can’t keep up, so the lifters in these studies wind up with large, inefficient muscles that could be made more efficient with training and by transitioning into a training phase focusing on adding strength without any more mass.
Or, of course, I could be entirely wrong. There’s not a lot of research on steroid use in healthy, athletic populations, and there are obvious confounding factors in both of these studies. I will say, though, it matches some of my observations. The guys on drugs who tend to do the best in weight class dominated sports like powerlifting, are the ones who add mass slowly, gradually increasing their doses or sticking with a conservative cycle for a long time instead of aggressively trying to add a lot of mass all at once. Look how long it took for Ed Coan to go from 165 to 242, as an example. Based on what I’ve seen, the guys who get the most out of their drugs – for strength – are the ones who take enough to primarily improve recovery, while gradually add mass over time – not put on 20+ pounds over night. Going back to Bashin, 2001, if you’re a powerlifter, you want the results of the 300mg/week group, not the 600mg/week group.
The last thing I’d like to talk about is how long steroid use benefits you.
The short answer – basically forever.
When your muscles grow, your muscle fibers add new myonuclei – each nucleus can only “manage” a finite amount of real estate in a muscle fiber, so your fibers have to add more as they grow. If you stop training, you may lose muscle size, but those myonuclei stick around for much, much longer. That’s the main reason behind the phenomenon of “muscle memory.” If you take a few months off lifting, you can come back to the gym and get back to your old levels of strength and muscularity pretty quickly, because your body doesn’t have to fuse new myonuclei again. The old ones are still sticking around (unless the muscle fiber itself dies, as could happen with aging or severe injury), so your body just ramps up protein synthesis and voila! It takes you a month or two to gain back the muscle it initially took you years to build, because protein accretion can proceed at a quicker rate than gaining new myonuclei.
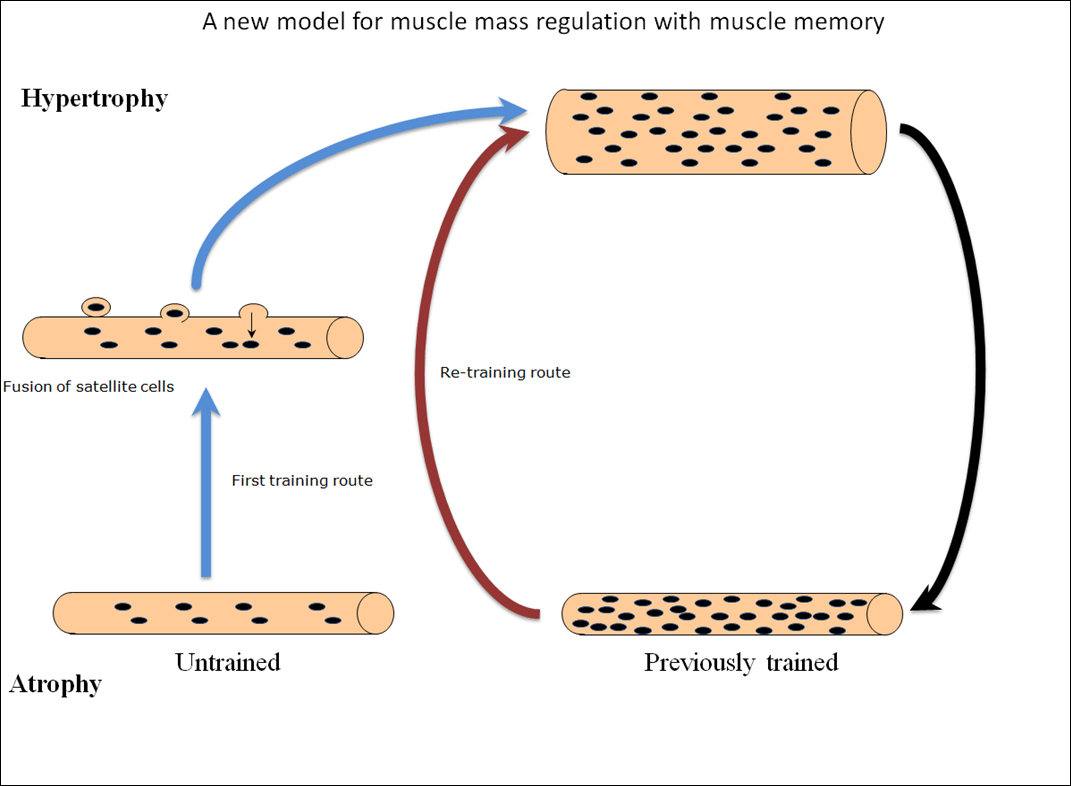
Of course, the application for steroids is pretty obvious. You take steroids, you gain mass, you go off, and those myonuclei are still hanging around, keeping you more jacked than you would have been otherwise.
So, here are some takeaways:
1) Steroids, physiologically, work. This much is not debatable.
2) On top of how well they work physiologically, a major factor is how well they work psychologically – if you do something expecting to get a ton stronger, there’s a good chance you’ll get a ton stronger. This applies to much more than steroids.
3) Steroids do provide a substantial advantage for sports that aren’t governed by weight classes. However, taking too high of a dose right off the bat may actually decrease performance (increased strength and mass, but decreased relative strength), especially in sports with weight classes. If you decide to use steroids, you’ll probably get the best bang for your buck, strength-wise, with very conservative doses initially.
4) If you take steroids and then come off of them, you’ll probably lose some of the size and strength you gained, but you’ll always be at an advantage relative to a lifetime drug-free athlete.
Share this on Facebook and join in the conversation
Next: Making Sense of Strength → Unleash Your Inner Superhero →
Greg Nuckols

Overshooting, Undershooting, Or Just Right? How To Perfect Your Ability To Predict Repetitions In Reserve.

Do Lengthened Partials Really Stimulate Stretch-Mediated Hypertrophy?

When to Use Specific Progressive Overload Strategies
Copyright © 2023 Stronger by Science
Appointments at Mayo Clinic
Prednisone and other corticosteroids.
Weigh the benefits and risks of corticosteroids, such as prednisone, when choosing a medicine.
Corticosteroid medicines include cortisone, hydrocortisone and prednisone. They are useful in treating rashes, inflammatory bowel disease, asthma and other conditions. But corticosteroids also carry a risk of side effects.
How do corticosteroids work?
When prescribed in certain doses, corticosteroids help reduce inflammation. This can ease symptoms of inflammatory conditions, such as arthritis, asthma and skin rashes.
Corticosteroids also suppress the immune system. This can help control conditions in which the immune system mistakenly attacks its own tissues.
How are corticosteroids used?
Corticosteroid medicines are used to treat rheumatoid arthritis, inflammatory bowel disease (IBD), asthma, allergies and many other conditions. They also are used to prevent organ rejection in transplant recipients. They do that by helping to suppress the immune system. Corticosteroids also treat Addison's disease. This is a rare disease that occurs when the adrenal glands don't produce enough of the corticosteroid that the body needs.
Corticosteroids are given in many different ways, depending on the condition being treated:
- By mouth. Tablets, capsules or syrups help treat the inflammation and pain associated with certain chronic conditions, such as rheumatoid arthritis and lupus.
- By inhaler and intranasal spray. These forms help control inflammation associated with asthma and nasal allergies.
- In the form of eye drops. This form helps treat swelling after eye surgery.
- Topically. Creams and ointments can help heal many skin conditions.
- By injection. This form is often used to treat muscle and joint symptoms, such as the pain and inflammation of tendinitis.
What side effects can corticosteroids cause?
Corticosteroids carry a risk of side effects. Some side effects can cause serious health problems. When you know what side effects are possible, you can take steps to control their impact.
Side effects of corticosteroids taken by mouth
Corticosteroids that you take by mouth affect your entire body. For this reason, they are the most likely type of corticosteroid to cause side effects. Side effects depend on the dose of medication you receive and may include:
- A buildup of fluid, causing swelling in your lower legs.
- High blood pressure.
- Problems with mood swings, memory, behavior, and other psychological effects, such as confusion or delirium.
- Upset stomach.
- Weight gain in the belly, face and back of the neck.
When taking corticosteroids by mouth for a longer term, you may experience:
- Problems with the eyes, such as glaucoma or cataracts.
- A round face, which is sometimes called moon face.
- High blood sugar, which can trigger or worsen diabetes.
- Increased risk of infections, especially with common bacterial, viral and fungal microorganisms.
- Bone fractures and thinning bones, called osteoporosis.
- Fatigue, loss of appetite, nausea and muscle weakness.
- Thin skin, bruising and slower wound healing.
Side effects of inhaled corticosteroids
When using a corticosteroid that you breathe in, some of the drug may deposit in your mouth and throat instead of making it to your lungs. This can cause:
- Fungal infection in the mouth, known as oral thrush.
- Hoarseness.
You may be able to avoid mouth and throat irritation if you gargle and rinse your mouth with water after each puff on your corticosteroid inhaler. Be sure not to swallow the rinse water. Some researchers think that inhaled corticosteroid drugs may slow growth rates in children who use them for asthma.
Side effects of topical corticosteroids
Topical corticosteroids can lead to thin skin, skin lesions and acne.
Side effects of injected corticosteroids
Injected corticosteroids can cause temporary side effects near the site of the shot. These side effects include skin thinning, loss of color in the skin and intense pain. This pain is known as post-injection flare. Other symptoms may include facial flushing, insomnia and high blood sugar. Health care providers usually limit corticosteroid injections to three or four a year, depending on each person's situation.
Reduce your risk of corticosteroid side effects
To get the most benefit from corticosteroid medicines with the least amount of risk:
- Ask your health care provider about trying lower doses or intermittent dosing. Newer forms of corticosteroids come in various strengths and lengths of action. Ask your provider about using low-dose, short-term medications or taking oral corticosteroids every other day instead of daily.
- Talk to your provider about switching to nonoral forms of corticosteroids. Inhaled corticosteroids for asthma, for example, reach lung surfaces directly. This reduces the rest of your body's exposure to them and may lead to fewer side effects.
- Ask your provider if you should take calcium and vitamin D supplements. Long-term corticosteroid therapy may cause thinning bones, called osteoporosis. Talk with your provider about taking calcium and vitamin D supplements to help protect your bones.
- Take care when discontinuing therapy. If you take oral corticosteroids for a long time, your adrenal glands may produce less of their natural steroid hormones. To give your adrenal glands time to recover this function, your provider may reduce your dose gradually. If the dosage is reduced too quickly, your adrenal glands may not have time to recover and you may experience fatigue, body aches and lightheadedness.
- Wear a medical alert bracelet. This or similar identification is recommended if you've been using corticosteroids for a long time.
- See your health care provider regularly. If you're taking long-term corticosteroid therapy, see your provider regularly to check for side effects.
Weigh the risks and benefits of corticosteroids
Corticosteroids may cause a range of side effects. But they also may relieve the inflammation, pain and discomfort of many different diseases and conditions. Talk with your health care provider to help you better understand the risks and benefits of corticosteroids and make informed choices about your health.
There is a problem with information submitted for this request. Review/update the information highlighted below and resubmit the form.
From Mayo Clinic to your inbox
Sign up for free and stay up to date on research advancements, health tips, current health topics, and expertise on managing health. Click here for an email preview.
Error Email field is required
Error Include a valid email address
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
Thank you for subscribing!
You'll soon start receiving the latest Mayo Clinic health information you requested in your inbox.
Sorry something went wrong with your subscription
Please, try again in a couple of minutes
- Ritter JM, et al. The pituitary and the adrenal cortex. In: Rang and Dale's Pharmacology. 9th ed. Elsevier; 2020. https://www.clinicalkey.com. Accessed Oct. 28, 2020.
- Grennan D, et al. Steroid side effects. JAMA. 2019; doi:10.1001/jama.2019.8506.
- Saag KG, et al. Major side effects of systemic glucocorticoids. https://www.uptodate.com/contents/search. Accessed Oct. 28, 2020.
- Saag KG, et al. Major side effects of inhaled glucocorticoids. https://www.uptodate.com/contents/search. Accessed Oct. 28, 2020.
- Roberts WN, et al. Joint aspiration or injection in adults: Complications. https://www.uptodate.com/contents/search. Accessed Oct. 28, 2020.
- Nieman LK. Pharmacologic use of glucocorticoids. https://www.uptodate.com/contents/search. Accessed Oct. 28, 2020.
- AskMayoExpert. Long-term glucocorticoid therapy. Mayo Clinic; 2019.
- Wilkinson JM (expert opinion). Mayo Clinic. Nov. 20, 2020.
- 6 tips to manage rheumatoid arthritis symptoms
- A Pain-Free Thumbs Up!
- Acetyl-L-carnitine: Can it relieve MS fatigue?
- Acute flaccid myelitis (AFM)
- Acute sinusitis
- Acute sinusitis: Do over-the-counter treatments help?
- Addison's disease
- Adrenal fatigue: What causes it?
- Albuterol side effects
- Alcoholic hepatitis
- Allergies and asthma
- Allergy medications: Know your options
- Allergy-proof your home
- Aplastic anemia
- Arthritis pain: Do's and don'ts
- Aspergillosis
- Aspirin allergy
- Asthma and acid reflux
- Asthma attack
- Asthma diet
- Asthma inhalers: Which one's right for you?
- Asthma: Colds and flu
- Asthma medications
- Asthma: Testing and diagnosis
- Asthma treatment: 3 steps
- Atopic dermatitis (eczema)
- Atopic dermatitis: 6 ways to manage itchy skin
- Atopic dermatitis: Proper bathing can reduce itching
- Atopic dermatitis: Understand your triggers
- Autoimmune neurological disorder
- Behcet's disease
- Explaining multiple sclerosis
- Treating Pericarditis
- Bullous pemphigoid
- Can I exercise if I have atopic dermatitis?
- Carpal tunnel exercises: Can they relieve symptoms?
- Carpal tunnel syndrome
- Carpal Tunnel Tune-Up
- Chagas disease
- Cholestasis of pregnancy
- Churg-Strauss syndrome
- Cluster headache
- Crohn's Crisis
- Crohn's disease
- Crohn's disease and the gut microbiome
- What is Crohn's disease? A Mayo Clinic expert explains
- Crohn's or Colitis
- De Quervain tenosynovitis
- Demyelinating disease: What can you do about it?
- Dermatomyositis
- Diffuse idiopathic skeletal hyperostosis (DISH)
- Does stress make rheumatoid arthritis worse?
- Drug allergy
- Dust mite allergy
- Ease rheumatoid arthritis pain when grocery shopping
- Ease stress to reduce eczema symptoms
- Eczema bleach bath: Can it improve my symptoms?
- Emerging treatments for multiple sclerosis
- Exercise and multiple sclerosis
- Exercising with arthritis
- Giant cell arteritis
- Glomerulonephritis
- Hand exercises for people with arthritis
- Hip labral tear
- How do I reduce fatigue from rheumatoid arthritis?
- How to treat baby eczema
- Hyperinflated lungs: What does it mean?
- Hypopituitarism
- I have atopic dermatitis. How can I sleep better?
- Inflammatory bowel disease (IBD)
- Inflammatory bowel disease FAQs
- Interstitial lung disease
- Is depression a factor in rheumatoid arthritis?
- Is there a special diet for Crohn's disease?
- Joint protection
- Juvenile idiopathic arthritis
- Keloid scar
- Knee bursitis
- Living better with atopic dermatitis (eczema)
- Living better with Crohn's disease
- Living better with rheumatoid arthritis
- Maintain your social life with Crohn's disease
- Managing Headaches
- Mayo Clinic Minute: Eczema occurs in people of all ages
- Mayo Clinic Minute: Prevent migraines with magnetic stimulation
- Mayo Clinic Minute: Weathering migraines
- Mayo Clinic Minute: What parents need to know about pink eye
- Medication overuse headaches
- What is a migraine? A Mayo Clinic expert explains
- Migraine medicines and antidepressants
- Migraine FAQs
- Migraine treatment: Can antidepressants help?
- Migraines and gastrointestinal problems: Is there a link?
- Migraines and Vertigo
- Migraines: Are they triggered by weather changes?
- Alleviating migraine pain
- Mixed connective tissue disease
- Mononucleosis
- Mononucleosis: Can it recur?
- Mononucleosis and Epstein-Barr: What's the connection?
- Multiple sclerosis
- Infographic: Multiple Sclerosis
- Multiple sclerosis: Can it cause seizures?
- What is multiple sclerosis? An expert explains
- Multiple sclerosis FAQs
- Myasthenia gravis
- Myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD)
- Nasal Cleaning
- Nephrotic syndrome
- Neuromyelitis optica
- New Test for Preeclampsia
- What is ulcerative colitis? A Mayo Clinic expert explains
- Occipital nerve stimulation: Effective migraine treatment?
- Ocular migraine: When to seek help
- Oral lichen planus
- Ozone air purifiers
- Paraneoplastic syndromes of the nervous system
- Pericarditis
- Pink eye (conjunctivitis)
- Pink eye: How long is it contagious?
- Plantar fasciitis
- Pneumonitis
- Polymyalgia rheumatica
- Polymyositis
- Prednisone withdrawal: Why taper down slowly?
- Preeclampsia
- Preterm labor
- Protect your joints while housecleaning
- Ramsay Hunt syndrome
- Rethinking Rheumatoid Arthritis
- Rheumatoid arthritis
- Rheumatoid arthritis: Does pregnancy affect symptoms?
- Rheumatoid arthritis and exercise
- Rheumatoid arthritis: Can it affect the eyes?
- Rheumatoid arthritis: Can it affect the lungs?
- Sacroiliitis
- Salt craving: A symptom of Addison's disease?
- Sarcoidosis
- Sheehan's syndrome
- Sinus infection and toothache: Any connection?
- Spinal stenosis
- Staying active with Crohn's disease
- Sulfa allergy
- Swollen knee
- Takayasu's arteritis
- Tendinitis pain: Should I apply ice or heat?
- Thrombocytopenia
- Thumb arthritis
- Thumb Reconstruction
- Tips for easing stress when you have Crohn's disease
- Tips to make your mornings easier
- Trichinosis
- Ulcerative colitis
- Ulcerative colitis flare-ups: 5 tips to manage them
- Understanding complement 3 glomerulopathy (C3G)
- Asthma attack video
- Carpal tunnel symptoms: Role of nonsurgical treatment
- Carpal tunnel syndrome surgery: Immediate and long-term results
- Dry powder disk inhaler
- Dry powder tube inhaler
- Video: How to use a peak flow meter
- Single-dose dry powder inhaler
- Using a metered dose asthma inhaler and spacer
- Vitamin D and MS: Any connection?
- Vitamins for MS: Do supplements make a difference?
- Vocal cord dysfunction
- What is aspirin-exacerbated respiratory disease (AERD)?
- Where can I learn more about living with Crohn's disease?
- Whipple's disease
Mayo Clinic does not endorse companies or products. Advertising revenue supports our not-for-profit mission.
- Opportunities
Mayo Clinic Press
Check out these best-sellers and special offers on books and newsletters from Mayo Clinic Press .
- Mayo Clinic on Incontinence - Mayo Clinic Press Mayo Clinic on Incontinence
- The Essential Diabetes Book - Mayo Clinic Press The Essential Diabetes Book
- Mayo Clinic on Hearing and Balance - Mayo Clinic Press Mayo Clinic on Hearing and Balance
- FREE Mayo Clinic Diet Assessment - Mayo Clinic Press FREE Mayo Clinic Diet Assessment
- Mayo Clinic Health Letter - FREE book - Mayo Clinic Press Mayo Clinic Health Letter - FREE book
- Prednisone risks, benefits
Your gift holds great power – donate today!
Make your tax-deductible gift and be part of the cutting-edge research and care that's changing medicine.
Find anything you save across the site in your account
Why Is Everyone on Steroids Now?

By Rosecrans Baldwin

Someone in your life is using performance-enhancing drugs. I feel comfortable making that bet because I recently discovered how many people in my life are using performance-enhancing drugs. Maybe your dad scored human growth hormone at an “anti-aging” clinic. Maybe the woman you met on Hinge just ordered her first “peptide stack.” It’s definitely the middle-aged white dude at work who calls you brother, who takes beta blockers before presentations—the same guy who texted you about T, testosterone, a.k.a. test, because he copped a vial off a friend and bro, things were wild, he felt crazy, like he could reply to a thousand emails while running through a wall. Brother, you need to check this shit out asap.
My curiosity about this sudden ubiquity helps explain how I came to meet Nick, 33, a handsome white guy, comprehensively tattooed, dressed in a workwear jacket and nice jeans. Nick looks like somebody you’d meet in an expensive coffee shop. It’s a look that doesn’t suggest, to most eyes, somebody who at times injected himself daily with steroids. Somebody who used to deal them and even “cooked” them in his kitchen. Somebody who once injected himself, Pulp Fiction –style, straight in the chest.
A decade ago, Nick lived with his parents in Southern California and had a day job doing manual labor; going to the gym was his escape. “Training was the only thing I could really do,” he said. “I was kind of a vegetable other than when I was in the gym.”
At the time, he struggled with erections, on account, he thinks, of antidepressants. A doctor tested his blood and found he had low testosterone. He tried adjusting his diet to boost his levels: fermented cod-liver oil, Brazil nuts, butter from grass-fed cows. Then the doctor prescribed testosterone replacement therapy (TRT). Before long, Nick was giving himself intramuscular injections, which seemed to do the trick: He felt more energized, more motivated, and he enjoyed how his body changed. The appeal of getting bigger had rattled around in his head for years. “I remember one of my first girlfriends mentioned I looked skinny,” he recalled. “Out of high school, I was 120, 130 pounds at five-ten. It stuck in my head, she mentioned I’d look crazy at 160.” Crazy, meaning hot. Then, through a gym buddy, Nick heard about SARMs—selective androgen receptor modulators. At the time, they were a relatively new class of experimental drugs, alleged to foster the benefits of anabolic steroids, like muscle building, but with fewer potential negative side effects. So he ordered some online.
Soon, with training and dieting, using testosterone and SARMs, Nick acquired a 28-inch waist and a 40-inch chest. He felt athletic, he felt strong. In the gym, he could squat 400 pounds for multiple repetitions, he said, and he could bench-press close to the same amount. Plus, he loved how he looked.
We were sitting outside a coffee shop in eastern Los Angeles. I asked Nick—who requested that I not use his real name; other anonymous subjects will be referred to by initials—if he could show me a picture from that period. He frowned and stared across the street. He said he’d deleted all the photos, he couldn’t look at them; looking at them made him depressed. Because, regretfully, he didn’t stop there. “I think in finance, they say one of the hardest things to master is ‘the art of enough,’ ” he said. “Steroid use, it’s the same.”
The use of performance-enhancing drugs, a.k.a. PEDs, remains something of a shadow world—but it may not remain so for long. Consider the shifting landscape of what’s now edging toward the mainstream in health care. Cannabis as a cancer therapy. Psychiatrists testing out psychedelics. MDMA being studied for use in treating PTSD. The gap between our society’s embrace of once-taboo ideas and its faith in institutional medicine is widening—and personally, I laugh anytime I catch a drug commercial telling me to consult my doctor, because who the hell has a doctor anymore? For many, medicine is no longer a visit to the physician’s office but a dip into YouTube, a scroll through TikTok, maybe a quick Zoom with a tele-med nurse practitioner, or a visit to the nearest urgent care.
And in that aperture, the use and abuse of PEDs appears to be flourishing. Potential upsides in some cases: muscle growth, quicker recovery, more energy. Potential downsides in some cases: cardiovascular disease, liver damage, fertility collapse. Also, for men, maybe a dash of testicular atrophy—it became a meme in my reporting notebook, after a number of men who had used steroids said their balls had miniaturized to the size of peas, of Raisinets, tinkling around in their un-shrunk sacks.

Today’s users, like T.B., represent a new breed of hormone enthusiasts. “Used correctly, [testosterone] makes everything better,” he said.
But maybe it’s worth it. This is an age, we are told, when anyone can have any body they want. Take a pill, stab a shot, try a “cycle.” It’s the age of Ozempic. The age of ordering a latte with a splash of collagen. Body optimization, body modification, whatever you want to call it, is no longer something that other people are doing, but rather something maybe you should be doing. Have you spent any time on social media lately? Have you felt: I’m getting left behind ?
I asked around my own friend circle this spring and discovered a gamut of boosting, occurring out of sight. Chris, 41, spends about a thousand dollars a month on a prescribed regimen of supplements—including dehydroepiandrosterone, an endogenous steroid hormone precursor—that requires him to pack syringes when he travels. “I don’t want to live forever,” he said. “I’m just trying to feel as good as possible.” Another friend, Jane, 33, got a prescription for peptides after she heard about them on a podcast—her stack includes sermorelin, a growth-hormone-releasing factor—and she also has begun traveling with needles. “I’m always scared TSA is going to be like, What the fuck is all this? , so I carry a doctor’s letter.” M.D., 37, got into lifting weights two years ago, and in only his second session at a gym the trainer suggested that if he was willing to get on “gear,” i.e., steroids, he could meet his goals much faster. The overture was casual, nonchalant—unnervingly so. “It was really scary!” M.D. said.
Fear, however, isn’t always the response this crazed moment inspires. Curiosity, feverishness, impatience, confusion, are also common feelings. Both online and off, drug use that once was a secret sneak for rule-breaking pro athletes—things like growth hormone, SARMs, anabolic-androgenic steroids—is being reframed and introduced to a wider set of users, whose motivations aren’t linked to sports. We’re talking about day traders and data managers. People who don’t intend to enter a bodybuilding competition but who want to feel more in control of how they look—who are eager to become the human lab–slash–gym rat of their dreams.
This age of bodily actualization is not without hazards. Nick said that one time, a day after injecting, a golf-ball-size lump appeared under his skin. He’d tried a new spot on his left quad, using inch-long needles. He took a hot shower and mashed the glob with his knuckles. Soon, he felt faint. Racing heartbeat, shortness of breath. Minutes later, in the kitchen, his legs locked up and he couldn’t walk. He lay on the floor, wrapped himself in a blanket, and stayed there for hours—freezing cold, sweating like crazy, panicking. An EMT friend later told him he’d likely been suffering from septic shock. Still, the next day he was spiking himself in the chest.
Seemingly every day a new compound, a new stack of dietary supplements, a new performance trend hits the internet. So, yes, someone in your life is using performance-enhancing drugs—I would bet on it. And what’s also possible, perhaps more foreboding, depending on what they’re taking, is that the individual doesn’t know exactly what it’ll mean for them in the long run. Victoria Felkar, who studies the industry as a researcher in women’s health and steroid hormones, told me something I heard a lot while interviewing users and experts: “This world is like the Wild West.”
Multiple forums exist online for PED fans to offer tips and query dangers. The jargon can be intimidating for a newbie but quickly absorbed. PEDs can be taken in “cycles” and potentially “blasted”; and multiple PEDs used together form a “stack.” To make one’s own “gear,” or steroids, means to “cook” them, and to inject oneself with the finished product is to “pin.” “Freak,” endearingly, is a label worn with pride.
The forums—which are loaded with young and middle-aged men uploading anonymous pictures from the gym—are full of stories about gains and losses but also problems at the office, or struggles with hair loss. Often, should a young member contemplate their first cycle, more seasoned dudes will offer advice, exhort them to self-educate, maybe read the book Anabolics, by William Llewellyn, currently in its 11th edition. Generally speaking, the conversations are candid and detailed. Discussion doesn’t shy away from the risks, whether acne or liver disease—as the bodybuilder slogan goes: Live large, die large, leave a giant coffin —which seems to inspire a striving for harm-reduction. Learning about PEDs used to mean a locker-room conversation between a couple of powerlifters. Today, and possibly for better, considering the amount of information shared online, it’s an all-night protein-shake klatch about the good, bad, and ugly in getting jacked.
One problem, though: Anabolic steroids and testosterone are Schedule III controlled substances. The possession of, say, a single vial of testosterone without a prescription is a criminal act. Also, what’s often not understood is the potential side effects that some of these compounds, particularly newer compounds being sold online, have on human users—sometimes in the short term and especially in the long term. A generation ago, before Congress criminalized steroids in 1990, anabolic users could score drugs that had been diverted from facilities monitored by the FDA. Unlike today, when newer, less studied compounds hit social media from who knows where, with nothing but flushed enthusiasm.
In the course of many conversations with people who’ve ventured into this vast community, I was surprised by the variety of motivations. A.B., a 23-year-old who lives in California, told me that he did his first cycle at 19 with testosterone and “loved every second of it.” (Arnold Schwarzenegger fashioned his routine around testosterone and the steroid Dianabol, he admitted last year.) At the time, A.B. didn’t like his job and had endured a bad breakup. “The gym was the only thing keeping me going,” he said. Today, he’s no longer using, partly because he found a new job he loves. “If things were worse, I’d probably hop back on to cope, if I felt like I was at rock bottom,” he admitted.
Performance-enhancing drugs as a way to pick yourself up when you’re feeling low—for some people, it’s a thing.
T.B., 49, who also lives in California, said that for him, “used correctly, [testosterone] makes everything better.” He took testosterone under a doctor’s supervision, and reported improved sleep, increased metabolism, less soreness. As for downsides, he noticed his moods and emotions could shift unpredictably—and during periods when he stopped using, he felt fatigued and gained weight. Also, “your balls will shrink up,” he said, echoing a number of other conversations. “Not crazy, but you’ll notice a change.”
There really was a lot of talk about testicles.
D.C., a 23-year-old who lives in rural West Virginia, said he didn’t have any difficulty scoring drugs. He started using when he was 18 or 19 and had done about half a dozen cycles since then, only with testosterone. “If you walk into Planet Fitness [you’re] probably going to have a tough time. If you walk into the old-school, powerlifting gym that’s half run-down, just about any dude you ask will have some.”
I asked if he’d consulted with a medical professional. He said he’d discussed it with a nurse practitioner. “Their answer is always not to use,” he said. “Not exactly helpful when I’m ignoring that.”
One of the users I spoke to was a physician himself—M.B., a 41-year-old from Missouri, who told me he started using at 32. He had since tried many compounds including human growth hormone and insulin (the latter he acquired over the counter in a chain retailer where it’s commonly sold in most states. Nick said he obtained insulin similarly: “It’s probably the most dangerous anabolic you can take, and it’s the easiest anabolic you can get. It’s ridiculous.”)
“As a medical professional, I understand the risk-reward balance of almost all modern pharmaceuticals,” M.B. said. “Biologically speaking, there is no free lunch.” I asked if he was out about his PED use to colleagues. Only his wife, coaches, and a few training partners knew, M.B. said. “At this point, unless my health markers change entirely, I’m unlikely to stop. I live a clean lifestyle—no tobacco, alcohol, excessive caffeine, or fast food. This is my single vice.”

E.O., above, is on TRT but previously used anabolics to get huge. “A lot of men are attracted to trying to fix a hole in their ego,” he said.
Multiple guys said they were bothered by the persistent stereotypes of PED users as meatheads, as aggro dudes prone to so-called roid rage—it just didn’t square with the people they had befriended. “There are doctors, engineers, government officials, nurses, software engineers, attorneys, small-business owners, accountants,” a 32-year-old named J.R. told me. He lives in North Carolina and serves as an administrator in one of the forums. “There are devoted husbands and committed fathers. There are men more well-versed in organic chemistry and scientific literature than most of the people I went to college with.”
Another assumption or cliché that proved unfounded: that PED users, particularly steroid users, are homophobic straight dudes. Plenty of LGBTQ+ people use PEDs, and there’s a lot of sympathy for the trans community; after all, one way to support trans people is to defend an individual’s right to alter their body with hormones. Alex Tilinca is a 23-year-old trans man from Long Island. He trains mostly trans men, including trans men interested in competitive bodybuilding. “It’s a sport where hormones are involved—it’s a natural equalizer,” he said. “And people are really receptive to trans guys in the competitive bodybuilding world.” For his own journey, Tilinca had found the gym to be an accepting place to hang out. “All the big guys, they were the ones that supported me. They knew I was trans. They helped me learn how to train properly. They’re sincerely gentle giants, honestly.”
If you’re wondering, But why now?, ask yourself when you last visited the gym and didn’t spot at least one smartphone poised on a machine, filming a workout. Rick Collins, an attorney who specializes in laws around steroids and supplements, put it succinctly: “Social media put steroids on steroids.”
On Instagram, well-known steroid users like the Liver King flex their pecs for millions of followers. On TikTok, professed testosterone user and 70-year-old presidential candidate Robert F. Kennedy Jr. does pull-ups. The platforms are super apps for performance enhancement: places where the curious can be inspired by (edited) photos, introduced to (sketchy) regimes, and directed where to (illegally) purchase them, before finally sharing topless mirror selfies, to display their boost-gotten gains.
Perhaps performance-enhancing drugs, as a term, is itself outdated—and the reason why some experts have already begun to adopt the phrase performance-and-image enhancing.
Of course, given stigmas that still exist, not to mention the risk of jail time, plenty of people who use PEDs don’t admit to using them—especially if they have tons of followers and their income increases by acquiring more. Kenneth Boulet, known as Kenny KO, has built a following based in part on attending fitness exhibitions and asking influencers, on camera, whether their physiques are artificially enhanced—that is, whether they are, in the parlance, “natty or not.” (In May, TikTok had over 20,000 videos posted with the hashtag “natty or not.”) Boulet used steroids in his 20s while training to be a firefighter. Now he’s trying to discourage use by fostering honesty about which influencers are juicing. “They’re taking crazy cycles, saying they’re natural,” Boulet said with exasperation, though he admitted to understanding the appeal. “The feeling when you’re on a cycle is amazing. That’s the addictive part,” he told me, “but it’s not maintainable.”

Alex Tilinca, above, found the world of bodybuilding accepting of trans men like him. “It’s a sport where hormones are involved—it’s a natural equalizer,” he said.
He said he hoped to spread awareness and help young people realize they shouldn’t compare themselves to what they see online. “There’s nothing more I dislike than a message from a 16-year-old wanting to hop on their first cycle because they saw their favorite influencer, and they’re thinking of hopping on tren,” Boulet said, referring to trenbolone, an anabolic that’s used to enlarge beef cattle.
His message, he admitted, could be misunderstood. “The amount of pro athletes and actors that have slid into my DMs, asking for input on cycles they’re on—it would be a mind-blowing thing for people to see.”
Hollywood has long been loaded with chiseled male bodies—and with actors who were quietly supplementing—but it’s never been easier for actors to get ripped. In the 2023 book MCU: The Reign of Marvel Studios, a professor of physical therapy at the University of Southern California estimated that 50 percent to 75 percent of Marvel stars use some form of PED. A television actor told me—we spoke in March before watching Love Lies Bleeding, the recent Kristen Stewart film that, like 2022’s Bros, uses roid rage for a storyline—that he took creatine to prepare for shirtless scenes, and he’d heard that some castmates used T. “There’s no drug testing in movies,” Lars Wallin, a West Hollywood trainer who works with stars, told me. “The simplest thing to do, to stop this whole trend, is to enforce drug testing on movie shoots, and have actors be fired if they’re found positive.” Then again, who in the industry would be incentivized to do such a thing?
Last December, Reacher ’s Alan Ritchson broke the code of silence. “For me, it’s a long game. I want to do Reacher for 15 years,” he told Men’s Health UK. Apparently, the work to get big and cut for the show’s first season had “ravaged” his body, resulting in a shoulder injury. “I don’t want to have to have surgery after every season, and testosterone helps.”
V.S. is in his 30s but was 19 when he first got curious. “College is a time where you’re comparing yourself to everyone else,” he told me. “I was always a tiny guy. I thought it would be cool if I could reverse that for once.” He ordered several compounds online, and soon he was bigger, more cut, receiving compliments from strangers. He compared it to playing Grand Theft Auto with cheat codes—once you’d experienced the game with codes, why would you go back? V.S.’s PED career lasted eight years. Today he lives in Florida, is on TRT, and may be for life—a notion he struggles to accept. “It’s like, how much of a loser am I going to feel, when I have a wife and kids, and we’re trying to go to Puerto Rico, and Daddy has to pack his needles?”
In the world of PEDs, young users often think their dabbling will be temporary, with short-term consequences; unfortunately, the drugs don’t always work that way. For instance, men who use steroids frequently suppress their body’s own production of testosterone—sometimes persistently. A strength-and-conditioning coach in Ohio told me, “Once you make that leap, odds are good that it’s gonna be for life.”
“The first time you do steroids, you’re kind of finished,” V.S. said. “There’s no turning back from that point.”
These days, V.S. works with a doctor named Thomas O’Connor, who specializes in helping patients who use or previously used PEDs, and shares information online as the Anabolic Doc. His choice of specialty was informed by his own experience. “I’m a 60-year-old dude,” he said. “I did steroids in my 20s. By the time I was in my 30s, I was shut down, and I’ve been on testosterone ever since. I do not give a blessing on steroids.”
O’Connor said he’d had more than 500 patients on dialysis, and had seen dozens of patients commit suicide. He ticked through potential health outcomes for steroid users, like coronary disease and depression. “And it’s not just steroids. You have SARMs, peptides, growth factors, secretagogues, IGF-1, insulin, clenbuterol—I can go on and on.” In terms of a typical patient, more and more, he said, he saw young men, including teenagers. “They’re regular dudes who have a desire to get ripped. The drugs work, and now they’re widely accessible with the internet. It’s been normalized because of accessibility.”

Kenneth Boulet, who no longer uses steroids, works to encourage honesty about usage with his social media series “Natty or Not.”
Many of O’Connor’s clients got into PEDs long before they became more commonplace. E.O., 42, is a client who works in finance in New England and is on TRT. When he was in his late 20s, he felt burned out by obligations: raising a family, stress at work. He started supplementing with testosterone and eventually fell into what he described as the “more-is-better trap”—experimenting with anabolics, on top of T, to get huge. Odd things started to happen; not necessarily bad things. Women approached him in the grocery store and squeezed his arm. At investor conferences, he was mistaken for security. Today, still quite big, he saw insecurity in a lot of users’ motivations. “I think it’s a personality thing,” he said. “I think a lot of men are attracted to trying to fix a hole in their ego.”
Others were chasing a long-lost feeling, said Jessica Cho, a doctor who runs an integrative medicine practice in Los Angeles. She told me the question she hears from new patients is often the same: Can you make me feel like I’m 18 again? “One of the biggest fights I have with patients is men wanting more testosterone,” she said. “They abuse it and then they give it to their friends. I cannot tame them. I make them sign a waiver saying if you abuse this outside my office, you’re taken off. This is the one area in my whole practice where everything is about compliance.”
What patients sometimes fail to grasp, she says, is that testosterone doesn’t operate in isolation; the endocrine system is similar to an orchestra, where hormones work together for balance, not cacophony. She mentioned she also saw a lot of renal issues in men from consuming too much protein and too many supplements. “They’re taking crazy amounts of supplements and their kidneys are getting knocked out.”
Researchers in the Netherlands have linked steroid use to left ventricular hypertrophy and impaired systolic and diastolic function. Steroid use has been connected to mood and anxiety disorders. In 2022, The Washington Post documented more than two dozen bodybuilders who died young. Meanwhile, multiple experts told me there’s a general lack of education around PEDs in the medical establishment. On top of that, there simply isn’t enough good empirical data, extensive medical trials, for a typical physician to consult. Which perhaps leaves the average user—especially a new, optimization-focused user, roaming around this nouveau Wild West—more open to “bro science” and harm.
Reporting this story, I heard gnarly anecdotes of people getting conned, guys pinning themselves with bunk gear. And I heard from people with no complaints, who loved their peptides, loved their T. And I ran into anecdote after anecdote filled with dysmorphia and pain. What can we expect with normalization? Ideally, more education, more accurate information, and, in a utopian world, an adult could make an informed decision about using PEDs with medical oversight. But right now, unless the laws change, that’s not the case. One night, after a series of interviews, I turned to my wife and said, “I think this may be the saddest story I’ve ever done.”
Despite the warnings from doctors, the embrace of PEDs is a party that appears to be only growing. Next year, if organizers prevail in their plans, one of the wilder experiments in normalization will get underway: the Enhanced Games. The inaugural event is being planned with support from, among others, the billionaire biohacker Peter Thiel. Its model is an Olympics-style competition—including swimming, weightlifting, track and field—wherein contestants will be permitted to supplement, provided they juice under medical supervision. Basically: a celebration of transparency around augmentation.
“The Olympics inspires hope and competence in the world, but it’s broken and dysfunctional on so many levels,” Enhanced Games founder Aron D’Souza told me. He cited a 2017 study commissioned by the World Anti-Doping Agency that surveyed more than 2,000 athletes at a pair of international sporting events and estimated past-year doping in 43.6 percent of participants at one of them, 57.1 percent at the other. In a statement to GQ, the International Olympic Committee noted that it has a “zero-tolerance policy to combat cheating and hold accountable anyone responsible for using or providing doping products.”
Nonetheless, to the extent that PED use does occur in competitive sports, the Enhanced Games want to pull it out of the shadows. “Any normalization helps,” Christian Angermayer, D’Souza’s cofounder, said. He pointed to society’s acceptance of certain substances over others, despite health outcomes for users and potential harm to others—the risks of drinking alcohol, say, compared to using things like anabolic steroids. (Booze has been associated with significantly worse effects.)
Borrowing their term, I asked if they themselves enhanced, and if so, how? Angermayer said he used a personalized stack of PEDs under strict medical guidance and supervision. D’Souza said he was considering starting but planned to wait until the Enhanced Games’ medical safety protocols were finalized.
Nick’s experiences, as a former user, demonstrated how much medical oversight might have helped.
His initial DIY use of SARMs had been an egress into rougher stuff. At first it was Masteron and Equipoise, purchased from a creepy gym bro. But something was wrong with the drugs; postinjection, he developed large lumps under his skin. “I couldn’t go over speed bumps in my car without wincing.” Homemade steroids are a combination of a hormone powder, alcohol, and a carrier oil, where the powder gets dissolved and heated into a solution. Nick suspected the drugs he’d bought weren’t prepared properly. “If you don’t cook steroids long enough, they don’t transition from powder into liquid,” he explained. “It means your gear is ‘crashed. ’ ”
Still, Nick stuck with them and gradually added other compounds. He rattled off some of the drugs he tried during his career with such familiarity, they sounded like underground hardcore bands. Anavar, D-Bol, NPP. At times, depending on the compound, he was shooting every day, a thousand-plus milligrams per week. And he grew muscle, lots of it—and he also grew paranoid, and felt extremely lethargic outside the gym. And yet: “The second you touch a weight, you’re a god. I was gaining 20, 40 pounds on my bench press every two to three weeks. It was madness.”
Meanwhile, one of the drugs turned his sweat yellow (also his semen). His hairline receded and he switched to a mohawk. “This is the progression of bodybuilders: full hair, mohawk, bald.” Plus, he experienced such bad acne, he started going to a tanning salon multiple times a week, mainly to roast his back.
Eventually, Nick started making his own gear—partly to save money but also to make money. A single bottle of steroids cost him about six dollars to produce, and he could sell it for $50 to $90. Unfortunately, cooking wasn’t easy—the first batch bubbled over in the kitchen. By that point, in his mid-to-late 20s, he’d moved to Los Angeles, and a friend told him about a guy in Hollywood who’d cook on order, if you supplied the raw hormone powders. Nick met him, paid him, handed over the goods. A week later, “the dude rolled up to Starbucks with close to a thousand bottles of gear in a trash bag. So I’m going down Sunset Boulevard in broad daylight, bottles rolling around, clank, clank, clank . I’m walking to my car with a life sentence on my back, probably.”
Nick said he discovered he didn’t have the temperament to be a dealer. He gave away gear for free, plus he was using his own supply. And soon he hit his lowest point, when he was lying on the kitchen floor. “I had probably $20,000 to $30,000 worth of steroids cooked, ready for distribution. I had raw powders in the home from China. I had 911 dialed, but I kept thinking about the consequences of what might happen, just the shame for my family.”
Today, Nick takes a variety of peptides. He’s on TRT and believes he will be for life—mainly because when he’s gone off T before, “you have zero will to live. You don’t want to eat, you don’t want to fuck. You don’t want to do anything.” He enjoyed exploring new ways of being active: dance, rock climbing, jujitsu. “I still think being buff is cool, but a lot of those guys can’t do shit. Also, you can’t wear cool clothes,” he said, laughing. “It’s a rule. The bigger you get, the dumber the clothes.”
I asked what his advice would be for young people contemplating PEDs. His response was immediate: “Get into therapy.” I thought he was talking about hormone therapy, but no: psychological therapy. “Get into therapy, and take it as a challenge to learn to love the body you have. Get into therapy, be in therapy once a week for a good year, and work hard. It’s just like the gym: You get out what you put in,” he said. “It sounds so cliché and corny. I used to spit when I would hear shit like that. I thought there was something honorable in hating yourself enough to change your body.”
Nick’s voice was clear, steady, and despondent. “I had to find a way to love myself through almost dying,” he said. “I just hope that one young person [reading this] will stop early and coast forever.”
Rosecrans Baldwin is a frequent contributor to GQ and the bestselling author of ‘Everything Now: Lessons From the City-State of Los Angeles.
A version of this story originally appeared in the Summer 2024 issue of GQ with the title “Why is Everyone on Steroids Now?”

- +44 7418625617
Annals of Clinical Trials and Vaccines Research
Research Article - Annals of Clinical Trials and Vaccines Research (2023) Volume 13, Issue 4
- Download PDF
The Role of Steroids in Clinical Practice: Benefits, Risks, and Considerations for Therapeutic Use
Walter Lewis *
Department of Pharmaceutical Chemistry, Medical University of Graz, Austria
*Corresponding Author: Walter Lewis Department of Pharmaceutical Chemistry, Medical University of Graz, Austria E-mail: [email protected]
Received: 01-August-2023, Manuscript No. actvr-23-108542; Editor assigned: 3-August-2023, PreQC No. actvr-23-108542 (PQ); Reviewed: 17-August-2023, QC No. actvr-23-108542; Revised: 22-August-2023, Manuscript No. actvr-23-108542 (R); Published: 28-August-2023; DOI: 10.37532/ ACTVR.2023.13(4).128-131
Steroids, a class of organic compounds, have long been an essential component of clinical practice due to their potent anti-inflammatory and immunosuppressive properties. This article provides an in-depth analysis of the various applications of steroids in medical settings, exploring their benefits, risks, and crucial considerations for therapeutic use. From managing chronic inflammatory conditions to addressing acute emergencies, steroids have proven to be valuable tools in the hands of healthcare professionals. However, their side effects and potential for misuse demand a nuanced approach to prescribing and monitoring. This review aims to equip clinicians with up-to-date knowledge to make informed decisions regarding steroid therapy, ensuring optimal patient outcomes while minimizing adverse effects.
Biomarkers • Personalized medicine • Adaptive trial designs • Artificial intelligence • Regulatory approvals
Introduction
Steroids, also known as corticosteroids or glucocorticoids, are synthetic drugs that mimic the actions of naturally occurring hormones in the body. In clinical practice, steroids have a wide range of therapeutic applications due to their potent anti-inflammatory, immunosuppressive, and metabolic effects. This article provides a comprehensive overview of the various uses of steroids in medical practice, highlighting their benefits and potential side effects. Steroids have been a mainstay in clinical medicine for decades, and their applications continue to evolve as new research sheds light on their mechanisms of action. This article delves into the history and development of steroids as therapeutic agents and explores their role in managing various medical conditions. Steroids remain indispensable in clinical practice, playing a vital role in managing a wide range of medical conditions [ 1 , 2 ].
Their potent anti-inflammatory and immunosuppressive effects make them valuable tools for alleviating symptoms and improving patients’ quality of life. However, healthcare professionals must carefully consider the risks and benefits of steroid therapy, tailoring treatment plans to individual patient needs. Continued research and advancements in steroid therapy are likely to refine their applications in the future. Steroids, a class of potent anti-inflammatory and immunosuppressive agents, have long played a crucial role in various clinical specialties. This comprehensive review article explores the diverse therapeutic applications of steroids in clinical practice and highlights the associated considerations and potential risks. From managing autoimmune disorders and allergic reactions to addressing various inflammatory conditions, steroids have proven their efficacy across a wide range of medical conditions [ 3 , 4 ].
Material & Methods
The introduction provides a historical overview of the discovery and development of steroids, outlining their initial application and subsequent expansion into various medical fields. It emphasizes the significance of understanding the pharmacology and mechanism of action of steroids to optimize their use in clinical settings. This section delves into the pharmacokinetics and pharmacodynamics of steroids, explaining how different formulations and routes of administration can influence their efficacy and side effect profile. The focus is on the varying potency of different steroid compounds and the importance of tailoring treatments to individual patient needs.
The article emphasizes the importance of weighing the potential benefits against the risks when prescribing steroids. It addresses common side effects, such as weight gain, osteoporosis, mood changes, and increased susceptibility to infections. Additionally, special considerations are discussed, including steroid tapering, alternate-day dosing, and monitoring patients on longterm steroid therapy.
The conclusion highlights the significant impact of steroids on clinical practice and patient outcomes, while also advocating for a balanced and cautious approach to their use. It emphasizes the need for further research and continued efforts to refine steroid therapies to maximize their benefits while minimizing adverse effects. Steroids, also known as corticosteroids or glucocorticoids, have been a cornerstone in the management of various medical conditions for decades. These powerful anti-inflammatory agents have demonstrated remarkable efficacy in treating a wide range of diseases, spanning from autoimmune disorders to respiratory illnesses. This article aims to provide an indepth exploration of the use of steroids in clinical practice, shedding light on their mechanisms of action, indications, dosing strategies, potential side effects, and the latest research trends.
This section delves into the mechanisms through which steroids exert their effects on the immune system and inflammatory response. It discusses their impact on gene expression, cytokine modulation, and inhibition of immune cell activation. Additionally, the article examines how steroids interfere with the synthesis of prostaglandins and Leukotrienes, influencing the overall inflammatory cascade. Autoimmune diseases such as rheumatoid arthritis, systemic lupus erythematous, and multiple sclerosis can lead to debilitating symptoms. This part of the article explores the role of steroids as an essential component of the treatment regimen for these conditions. It also highlights the importance of early intervention and the balance between symptomatic relief and long-term management.
Respiratory conditions, including asthma and chronic obstructive pulmonary disease (COPD), often involve airway inflammation. The article examines the use of steroids in these cases, focusing on their ability to reduce airway inflammation, improve lung function, and prevent exacerbations. Dermatological conditions like eczema, psoriasis, and allergic reactions can significantly impact a patient’s quality of life. This section explores the role of topical and systemic steroids in managing these conditions, emphasizing the importance of appropriate application and potential adverse effects on the skin. The correct dosing of steroids is crucial to achieve therapeutic benefits while minimizing side effects. This part of the article discusses various dosing strategies for different conditions, as well as the importance of close patient monitoring during treatment to detect and manage potential complications.
Steroids are associated with a range of side effects, including weight gain, mood changes, osteoporosis, and increased susceptibility to infections. This section explores strategies to mitigate these side effects, such as lifestyle modifications, adjunctive therapies, and dose-tapering techniques.
As medical research progresses, new insights into the use of steroids continue to emerge. This final section of the article highlights recent developments and ongoing studies, including novel formulations, targeted therapies, and potential alternative treatments. Steroids play a vital role in clinical practice, offering effective management for various medical conditions. However, their use requires careful consideration, weighing the benefits against potential risks. By understanding their mechanisms of action, appropriate indications, dosing strategies, and monitoring, healthcare professionals can optimize the use of steroids and enhance patient outcomes. Ongoing research and advancements in this field promise a brighter future for patients who rely on steroids as part of their therapeutic journey [ 5 - 7 ].
Steroids, a class of potent anti-inflammatory agents, have been an indispensable component of clinical practice for several decades. This comprehensive review aims to explore the diverse therapeutic applications of steroids and their significant role in managing various medical conditions. From their use as powerful immunosuppressive agents to their essential role in treating hormonal imbalances, steroids have proven to be invaluable in enhancing patient outcomes. Tailoring treatment plans to individual patient needs. Continued research and advancements in steroid therapy are likely to refine their applications in the future. Steroids, a class of potent anti-inflammatory and immunosuppressive agents, have long played a crucial role in various clinical specialties. This comprehensive review article explores the diverse therapeutic applications of steroids in clinical practice and highlights the associated considerations and potential risks. From managing autoimmune disorders and allergic reactions to addressing various inflammatory conditions, steroids have proven their efficacy across a wide range of medical conditions
Steroids, also known as corticosteroids or glucocorticoids, have emerged as an essential pharmacological tool in clinical practice. Originally introduced for their profound anti-inflammatory effects, steroids have since demonstrated their versatility across a wide range of medical disciplines. This review examines the mechanisms of action, indications, and potential side effects of steroids, providing valuable insights for clinicians to optimize patient care. Steroids play a pivotal role in the management of various immunological disorders, including autoimmune diseases and organ transplantations. The article delves into the underlying immunomodulatory mechanisms of steroids, discussing their efficacy in suppressing immune responses and mitigating inflammatory cascades. The correct dosing of steroids is crucial to achieve therapeutic benefits while minimizing side effects. This part of the article discusses various dosing strategies for different conditions, as well as the importance of close patient monitoring during treatment to detect and manage potential complications.
A major area of clinical application for steroids lies in the treatment of respiratory conditions. The review evaluates the use of steroids in asthma, chronic obstructive pulmonary disease (COPD), and other respiratory disorders, outlining their effectiveness in reducing airway inflammation and improving lung function. The management of rheumatic diseases, such as rheumatoid arthritis, systemic lupus erythematous, and vasculitis, has been revolutionized by the introduction of steroids. This section investigates the role of steroids in alleviating joint inflammation and preventing disease progression However; their use requires careful consideration, weighing the benefits against potential risks. By understanding their mechanisms of action, appropriate indications, dosing strategies, and monitoring, healthcare professionals can optimize the use of steroids and enhance patient outcomes [ 8 - 10 ].
Steroids are vital in endocrinology for their ability to supplement hormonal deficiencies and regulate various physiological processes. The article discusses their use in adrenal insufficiency, Addison’s disease, and other endocrine disorders, emphasizing the need for precise dosing and monitoring to avoid adverse effects. Dermatological conditions, including eczema, psoriasis, and severe allergic reactions, often require steroids for their anti-inflammatory and immunosuppressive properties. The review examines the different formulations and routes of administration used in dermatology and highlights potential complications associated with long-term usage.
While steroids offer substantial therapeutic benefits, their prolonged use or inappropriate dosing can lead to a wide range of adverse effects. This section explores the potential risks associated with steroids, such as osteoporosis, glucose intolerance, and immunosuppression, prompting clinicians to carefully weigh the benefits against the risks in individual patients. Steroids represent a cornerstone of modern clinical practice, contributing significantly to the management of various medical conditions. This review provides an in-depth analysis of the diverse therapeutic applications of steroids, along with crucial safety considerations to guide clinicians in utilizing these potent agents judiciously. By understanding the intricacies of steroid therapy, healthcare providers can optimize patient outcomes while minimizing the likelihood of adverse events.
- Saraswat A. Topical corticosteroid use in children: Adverse effects and how to minimize them . Indian J. Dermatol. Venereol. Leprol. 76, 225–228 (2010).
Indexed at , Google Scholar , Crossref
- Beggs S. Paediatric analgesia . Aust Prescr. 31, 63–65 (2008).
Google Scholar , Crossref
- Rossi M, Giorgi G. Domperidone and long QT syndrome . Curr Drug Saf. , 5, 257–262 (2010).
- Kosek M, Bern C, Guerrant RL. The global burden of diarrhoeal disease, as estimated from studies published between 1992 and 2000 . Bull World Health Organ. 81, 197–204(2003).
Indexed at , Google Scholar
- Alam N, Najam R. Effect of repeated oral therapeutic doses of methylphenidate on food intake and growth rate in rats . Pak J Pharm. Sci. 28 9–13(2015).
Google Scholar
- Ryan C, Ross S, Davey P et al . Prevalence and causes of prescribing errors: The PRescribing Outcomes for Trainee Doctors Engaged in Clinical Training (PROTECT) study . PLoS ONE .9, 69-143 (2006).
- Patrick DM, Marra F, Hutchinson J et al . Per capita antibiotic consumption: How does a North American jurisdiction compare with Europe? Clin Infect Dis . 39, 11-17 (2004).
Indexed at , Google Scholar , CrossRef
- Li WC. Occurrence, sources, and fate of pharmaceuticals in aquatic environment and soil. Environ. Pollute. 187, 193-201 (2014).
- Heberer T. Occurrence, fate, and removal of pharmaceutical residues in the aquatic environment:A review of recent research data. Toxicol Lett. 131, 5-17 (2002).
- Banci L, Ciofi-Baffoni S, Tien M Lignin et al . Peroxidase-catalyzed oxidation of phenolic lignin oligomers . Biochemistry . 38, 3205-3210 (1999).
Google Scholar citation report

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- J Multidiscip Healthc
- PMC10759908
The Uses of Anabolic Androgenic Steroids Among Athletes; Its Positive and Negative Aspects- A Literature Review
Zhang wenbo.
1 Department of Physical Education, Changchun Institute of Education, Changchun, Jilin, 130033, People’s Republic of China
2 School of Physical Education, Inner Mongolia Minzu University, Tongliao, Neimeng, 028000, People’s Republic of China
The use of anabolic androgenic steroids (AAS) for strength training and muscle building is a widespread practice among athletes and young individuals. Athletes and bodybuilders are using these substances for various purposes, such as enhancing muscle mass, strengthening their bodies, and enhancing their performances. AAS exert a wide range of physiological effects that result in the activation of central signaling, resulting in adverse effects. Moreover, excessive use of AAS which can be categorized as AAS abuse; is linked to biological and psychological pathologies, which can lead to mortality. Complications arising from steroid abuse involve both cellular and physiological complications. Cellular complications arise when activation of signaling proteins like mTOR, Akt, etc. leads to alteration in protein synthesis pathways, cell cycle, oxidative stress, and apoptosis, contributing to damage at the cellular level. Physiological complications are evident with cardiovascular pathologies, including an altered lipid profile, cardiac hypertrophy, hypogonadism after discontinuation of AAS, and modulation of GABA receptors in the brain, all contributed by the androgen receptor signaling. Clinical complications budding from these altered physiological processes lead to clinical effects like testicular dysfunction, acne, gynecomastia, and neuropsychiatric disorders. Despite potential therapeutic benefits, AAS use is prohibited by the World Anti-Doping Agency (WADA) due to concerns over adverse health effects. This review highlights the molecular mechanisms, physiological processes, and clinical complications arising from the excessive use of AAS among athletes.
Introduction
The world of sports has long been a stage for human achievement, where athletes push their physical and mental limits to attain greatness. In this pursuit, the use of performance-enhancing substances has remained a contentious issue, with anabolic androgenic steroids (AAS) emerging as one of the most widely debated substances in sports circles. 1 Anabolic androgenic steroids, derived from the male sex hormone testosterone, have garnered attention due to their potential to significantly alter an athlete’s physical capabilities. 2 This literature review delves into the multifaceted landscape of AAS use among athletes, examining both its positive and negative aspects, shedding light on the motivations behind their use, and the subsequent physiological and psychological consequences.
Anabolic androgenic steroids, originally developed for medical purposes such as treating hormone deficiencies and muscle-wasting diseases, have found a different path in the realm of sports. 3 Athletes often seek their effects, which include increased muscle mass, strength, and endurance, with the aim of gaining a competitive edge. The allure of improved performance and the desire to achieve remarkable athletic feats has led to the illicit use of AAS by athletes across various disciplines. 4
The allure of AAS for athletes predominantly lies in the potential positive impacts on performance. The heightened ability to build lean muscle mass and increase strength can contribute to enhanced athletic performance. 5 AAS can accelerate recovery from intense training, enabling athletes to train more frequently and intensely. This heightened training capacity can translate to improved skill development and performance outcomes. 6 Moreover, the psychological boost resulting from these physical improvements can enhance an athlete’s self-confidence and self-esteem, which are crucial for optimal performance under pressure. 7
While the potential benefits of AAS are enticing, the negative aspects of their use cannot be overlooked. The misuse of AAS in sports can lead to a range of adverse health effects. 8 Physiologically, AAS can disrupt the body’s natural hormone balance, leading to a plethora of complications such as cardiovascular issues, liver damage, and reproductive system abnormalities. 9 Moreover, the misuse of AAS can also impact an athlete’s credibility and tarnish the integrity of sports. The unlevel playing field created by doping can undermine the principles of fair competition, eroding the essence of sportsmanship. 10
Athletes turn to AAS for a variety of reasons, often influenced by the intense pressures to succeed in a hyper-competitive sporting landscape. 11 The pursuit of fame, financial rewards, and national pride can push athletes to seek shortcuts to greatness. Additionally, the fear of falling behind peers who might be using AAS can create a sense of necessity, fuelling the prevalence of their misuse. The use of AAS in sports raises significant ethical and legal dilemmas. 12 The breach of fair play and the inherent risks associated with AAS consumption challenge the integrity of sports. Organizations such as the World Anti-Doping Agency (WADA) have established stringent regulations and testing protocols to curb the misuse of AAS and maintain a level playing field. 13 Athletes found to be using AAS face not only disqualification but also damage to their reputation and potential legal consequences. 14 , 15
The issue of AAS use among athletes is a complex matter with far-reaching consequence. 16 While the allure of enhanced performance through AAS is undeniable, the potential detrimental effects on health, integrity, and fairness within sports cannot be understated. 17 This literature review will delve into the nuanced layers of AAS use among athletes, dissecting the motivations that drive their use and the subsequent impact on physiological and psychological well-being. By comprehensively understanding the multifaceted nature of AAS use, stakeholders in the world of sports can make informed decisions to preserve the authenticity and sanctity of athletic competition while safeguarding the health and dignity of athletes. 18
Anabolic Steroids
Athletes use anabolic steroids to increase their strength and muscular mass. These substances are also known as anabolic-androgenic steroids. 19 Despite their negative reputation, anabolic steroids may be used therapeutically. These drugs might lower the damage that happens to muscles during a hard workout. That could help athletes bounce back faster from a workout. They might be able to exercise harder and more often. 20 Anabolic-androgenic steroids, sometimes known as “steroids” or “androgens”, are the most abused Performance Enhancing Drugs (PEDs). 21 , 22 These compounds are synthetic analogs of the male sex hormone testosterone. In both males and females, they increase the growth of skeletal muscle (anabolic effects) and the development of male sexual traits (androgenic effects). 23 The steroids are generally formed biologically from cholesterol and then interconverted, as shown in Figure 1 . Besides naturally occurring steroids, synthetic steroids do exist and are widely used among athletes. 24

Various steps involved in the biosynthesis of steroid hormones.
Anabolic steroids are classified as controlled substances in numerous countries, including Australia, Argentina, Brazil, Canada, the United Kingdom, and the United States. 26 Despite this, there remains a readily accessible global supply of steroids for non-medicinal use. This accessibility is because, in many countries, anabolic steroids can be legally purchased without a prescription. 27 , 28 Consequently, foreign distributors often operate within the legal framework of their nations when supplying these substances to international customers via online platforms and email orders. The majority of hormone products circulating in the European market originate from countries within the European Union and Russia, with occasional contributions from Thailand, Turkey, Egypt, India, and Pakistan. 29–31 Similarly, significant volumes of anabolic steroids in the United States are sourced from Mexico, Russia, Romania, and Greece. 32
In the United Kingdom, the Misuse of Drugs Act classifies anabolic steroids under Schedule IV Part 2. 24 This includes most anabolic steroids as well as clenbuterol (an adrenoreceptor stimulant) and human growth hormone. 33 While there are no restrictions on possessing these substances within medicinal products for self-administration, individuals have faced intent-to-supply charges for possessing large quantities without a prescription. Importing and exporting anabolic steroids requires a Home Office license, with exceptions for small quantities for legitimate purposes. 34
Regarding doping control in human sports, the International Olympic Committee (IOC) Medical Commission designated anabolic steroids as a banned class in 1974. 35 The term “anabolic agents” emerged in the 1990s to encompass substances like clenbuterol and other β2-agonists, which also possess anabolic activity and are subject to out-of-competition testing. 36 The World Anti-Doping Agency (WADA) was established in 1999 under the IOC’s initiative, uniting various organizations and governments against doping in sports. 37 WADA’s regulations and technical documents, including those concerning anabolic steroids, are consistently evolving, and accessible on the WADA website ( http://www.wada-ama.org/en/ ).
Misuse of anabolic steroids extends beyond sports to society, with adults and adolescents seeking cosmetic benefits such as muscle growth. Anabolic steroid abuse rates vary, with around 5% use among gym-goers and 25–50% among competitive bodybuilders. 38–40 Estimating the true UK-wide usage is challenging, but the British Medical Association’s report indicates widespread use. 41 The United States also faces high prevalence rates. 42
Within sports drug control, anabolic steroids are both performance enhancers and health hazards. In 2006, among 198,143 urine samples analyzed by WADA-accredited labs, 2% contained prohibited substances, with 45% of adverse findings linked to anabolic steroids. 35 Frequent steroids include testosterone, nandrolone, stanozolol, and methandienone. Detecting testosterone use is complex due to its endogenous production. The urge for success drives competitors to enhance performance despite the risk of penalties, even though some claim WADA’s statistics do not fully reflect steroid doping in top-level athletics. 34 , 43 , 44
Anabolic steroids’ chemical structures and activity have undergone modifications to amplify anabolic effects and minimize androgenic ones. 45 While some steroids have been withdrawn in several countries, they remain available in others for medical use, such as methandienone, methyltestosterone, oxandrolone, and stanozolol. In the United Kingdom, licensed products include testosterone and its esters, nandrolone (as the decanoate ester), mesterolone, and oxymetholone (restricted to named patients). Some countries limit boldenone and trenbolone to veterinary purposes, yet athletes and bodybuilders sometimes administer these anabolic steroids. 34
Methenolone acetate, methandrostenolone, oxandrolone, oxymetholone, and stanozolol are some of the orally administered steroids in use among athletes. Some intramuscularly used steroids are boldenone undecenoate, methenolone acetate, nandrolone decanoate, Sustanon 250 ® , testosterone enanthate, and testosterone cypionate. 46 Anabolic-androgenic steroids are the best-studied class of PEDs that can boost a user’s confidence and strength, leading users to overlook the severe, long-lasting, and in some cases, irreversible damage they can cause. 47
Population Burden of AAS Abuse
Anabolic androgenic abuse gained popularity due to its impact on physique and performance in sports like bodybuilding, weightlifting, baseball, football, cycling, wrestling, and many others to improve their performance. 48 The gain in muscle mass and strength contributes to aesthetic appeal and therefore use of androgenic anabolic steroids paved the way to the events of abuse. Among Americans with ages ranging from 13 to 50 years, 2.9–4.0 million people have reported using AAS. Almost 1 million people utilizing AAS within this community have reportedly developed AAS dependence. 49 The use of AAS is likely to be observed in gym members practicing weightlifting followed by the number of people working in the private sector and beyond 25 years of age. AAS abuse is more evident in Western regions as compared to Africa and Asia. The report explains that this high likelihood of AAS abuse can be attributed to the concept of “muscularity” in those culture. 50 , 51 However, other than the cultural norms, factors that are associated with AAS abuse, especially in gym members include weightlifting, the use of supplementary vitamins, special diets, and social exposure to people who regularly use AAS for similar purposes. 52 Accurate estimation of steroid-associated gynecomastia is crucial for effective healthcare planning and tailored treatment approaches. The studies identify indicators of steroid usage, assesses responses to surgical and nonsurgical management, and compares preoperative and intraoperative data between different groups. The results highlight the significance of monitoring steroid consumption in gynecomastia cases, which often goes underestimated due to social stigma and misdiagnosis. 53 , 54 The use of AAS not only impacts sports performance but also poses significant health risks and psychological consequences, highlighting the importance of comprehensive education, awareness, and intervention strategies to address the widespread issue of AAS abuse. 8
Uses and Recommendations of AAS
Since use of drugs is generally regulated, AAS has also been subject to approval from FDA, 55 where it has been indicated for primary hypogonadism, delayed puberty in boys, hypogonadotropic hypogonadism, gonadotropin and luteinizing hormone-releasing hormone (LHRH) deficiency, pituitary-hypothalamic axis (HPA-axis) dysfunction originating from various tumors. 56 AAS is also used for the treatment of physiological deficits arising from anatomical abnormalities like cryptorchidism, orchitis, testicular torsion, vanishing testis syndrome. Patients with a history of orchiectomy, Klinefelter syndrome, or ongoing therapy with chemotherapeutic agents, alcohol abuse, and heavy metal poisoning are also treated with AAS. 57
Testosterone is also used as an adjunct treatment for certain malignant conditions bone marrow stimulation in leukemia and aplastic anemia, however, these treatments are non-FDA approved. 58 Similarly, kidney failure, growth failure, stimulation of appetite, muscle mass in malignancy, and acquired immunodeficiency syndrome are also treated with AAS. 59 Furthermore, it’s important to note that while AAS has legitimate medical uses as mentioned, its potential for misuse and abuse, along with the associated health risks, underscores the critical necessity for responsible medical supervision and comprehensive patient education regarding the proper and safe use of these substances. 60
Molecular Mechanisms of AAS
Increased size and muscle strength are desirable for aesthetic appeal however, at a cellular level, the use of AAS will lead to activation of multiple pathways that result in the increase in size of muscles and strength. Since these pathways have different outcomes in other types of cells, they may, therefore, elicit a different outcome response. 61 Androgens increase both the size and strength of skeletal muscle via diverse mechanisms. AAS binds to and activates androgen receptors in nuclei resulting in transcription of the associated genes. 62 , 63 These genes include transcription factors specific to muscles, structural proteins, microRNAs, and enzymes. Activation of these proteins also results in cellular cross-talk with other signaling molecules as well which include Akt, myostatin, IGF-I, and Notch signaling. 62 Akt is a central signaling molecule therefore, its activation can also lead to unwanted physiological effects. The metabolic effects of anabolic androgen are reflected by their effect on muscles where they increase Ca 2+ uptake and modulate kinase activities. 62 While IGF-1 signaling is responsible for cellular growth functions, its receptor, IGFR, is a tyrosine kinase receptor and activates common downstream signaling molecules including Akt, leading to the activation of S6K1, which translates into protein synthesis and growth. The cellular growth and strength are therefore contributed by both activation of downstream Akt and S6K1 and activation of nuclear receptors. 64
Anabolic androgenic steroids (AAS) are synthetic derivatives of testosterone that are commonly used to enhance athletic performance and promote muscle growth. These compounds exert their effects primarily by binding to androgen receptors within cells, leading to various physiological responses. 65 The molecular mechanisms of AAS involve interactions at the cellular and molecular levels, influencing gene expression, protein synthesis, and cellular signaling pathways. 66 Several studies have investigated the molecular mechanisms of AAS. For instance, research has shown that AAS usage can induce changes in gene expression in muscle cells, contributing to muscle growth and potentially muscle memory. This suggests that AAS might lead to the retention of myonuclei in muscle tissue, which could contribute to long-term muscle adaptations. 66 , 67
AAS has also been found to influence cardiac function and the central nervous system. 68 Chronic use of AAS has been associated with ventricular repolarization disturbances and disruptions in areas of the central nervous system, leading to behavioral changes. 69 The precise molecular mechanisms underlying these effects are still being studied, and more research is needed to fully understand these complexities. At the cellular level, AAS impacts protein synthesis by upregulating the expression of various genes related to muscle growth and repair. Additionally, AAS may modulate calcium homeostasis and cardiac contraction in heart cells, potentially affecting cardiac function. 70
Physiological Mechanisms of AAS
Effects on muscles.
The growth effects of AAS are exerted by the promotion of protein synthesis through gene transcription as described earlier. The binding of AAS to its receptor results in the displacement of glucocorticoids from their receptors. 71 Consequently, protein degradation is inhibited as glucocorticoids are responsible for the degradation of protein in the cell. 72 Among these anabolic steroids, stanozolol’s mechanism of action has been hypothesized to be influenced by a significant increase in type I muscle fiber size which provides enough strength for the athletes to exercise longer, consequently resulting in type II fiber hypertrophy. 73 Testosterone injections of 600 mg dose on the other hand have shown a greater increase in fat-free mass in individuals who were not exposed to exercise intervention as compared with those who did resistance exercise with placebo treatment. 74 These effects are demonstrated for the increase in muscle mass mainly while no such effects have been observed in muscle concentrations of creatine.
Contrary to these findings, AAS doping in athletes in a dose-dependent manner has exhibited an increase in capillary density, muscle fiber area, myonuclei density, and lean body mass, thereby leading to the conclusion that AAS supplementation increases lean leg mass, muscle fiber size and improvement in muscle strength. 75 These studies showing long-term administration of AAS’s enhancement effects in human skeletal muscle morphology and physical performance. 76 The effects of anabolic androgenic steroids (AAS) on muscle growth involve intricate physiological mechanisms. AAS promotes protein synthesis through gene transcription and inhibits protein degradation by displacing glucocorticoids from their receptors. 77 Notably, distinct AAS like stanozolol may influence type I muscle fiber size, enhancing endurance, while testosterone injections exhibit differential fat-free mass increases based on exercise exposure. 78 Despite debates, AAS supplementation demonstrates the potential to augment muscle mass, fiber size, and overall strength, particularly in physically demanding sports; however, misuse without clinical guidance remains a concern.
Effects on Liver
As with most other drugs, the frequency and severity of hepatic adverse effects from AAS arise from several factors including formulation of the drug, route of administration, dosage, duration, and idiosyncratic responses. 79 Hepatotoxic effects of testosterone occur due to slower clearance of anabolic steroids like testosterone. These adverse effects are likely to arise from 17-α-alkylation modification, which makes their use desirable for oral intake. 66 Moreover, such substitutions facilitate the potency and duration of action of these anabolic steroids. Hepatotoxic events are related to elevated liver transaminases, translating into acute cholestatic syndrome. Testosterone and its derivatives especially have been frequently employed as a causative factor in a specific form of cholestasis called peliosis hepatis, benign and malignant hepatic tumors. 80 Other than that, chronic vascular injury, fatty liver diseases associated with toxicants like alcohol, and significant lipoprotein alterations have been observed with the use of AAS. Usually, these modifications are reversible with cessation of steroid use, however, some of them can pose life-threatening conditions. 81 Overall, the hepatotoxic mechanisms currently unveiled in AAS-related hepatotoxicity include disturbance of antioxidative factors, upregulation of bile acid synthesis, and induction of hepatocyte hyperplasia. 71 The AAS-induced hepatotoxic effects result from various factors, encompassing drug formulation, administration route, dosage, duration, and individual responses. Hepatotoxicity, often linked to elevated liver transaminases and acute cholestatic syndrome, can stem from the 17-α-alkylation modification in AAS, which enhances their oral availability and effectiveness. 82 Additionally, AAS usage has been associated with intricate hepatic conditions like peliosis hepatis, benign and malignant tumors, vascular injuries, fatty liver disorders, and disrupted lipoprotein profiles. 61 While many alterations are reversible upon discontinuation, certain consequences may escalate into severe, life-threatening scenarios.
Effects on Bones
The mechanism of androgens in the skeletal system is to inhibit bone resorption through osteoclastic activity. This results in the increase of androgen receptor-mediated bone formation. 83 The increase in bone formation is associated with longitudinal and periosteal bone growth and an increase in bone mass. In various conditions, including ovariectomized and orchiectomized rats, AAS exhibit anti-catabolic effects by reducing trabecular bone resorption, while also demonstrating the potential to enhance cortical bone strength, providing insights for addressing established osteoporosis related to aging. 84 , 85 In the ovariectomized and ovariectomized rats, AAS have shown decreased trabecular bone resorption which further elaborates their anti-catabolic effects in bone. 86 In particular, an increase in the mechanical strength of cortical bone was observed in ovariectomized rats with AAS use, a finding that led to the development of AAS as a potential lead for treating established osteoporosis associated with aging. 87 AAS has shown stimulation of endosteal bone formation. These findings have provided recommendations for AAS use particularly ND and nandrolone in estrogen-deficient conditions. 88 Administration of ND and nandrolone have revealed their significant effects in increasing bone mass in osteoporotic men and women. The bone gain with AAS use in such patients is almost 3% per annum, however, maximal effects are observed in the initial months of treatment. 89 This bone gain is associated with stimulation of bone formation, increase in serum albumin, and fat-free skinfold thickness. 90 Research using cellular models like SaOS-2 cells has also shown promising results for AAS use by promoting osteogenic commitment in these osteoblasts. 91 Despite their positive effects on bone growth, AAS use has shown a paradoxical effect on tendons and ligaments. Contrary to their anabolic effects on bone formation and bone growth, rupture of biceps and quadriceps tendons has been reported in athletes using AAS. 92 Conclusively, despite their deleterious effects on other organs, AAS have desirable effects on bone formation and growth, which calls for more cellular and clinical studies deciphering their effects on bone-related disorders.
Effects on Fat Metabolism
Alteration in fat metabolism due to AA use has shown a decrease in sphingolipids and glycerolipids with palmitic, palmitoleic, stearic, and oleic acids. These lipids serve as a building block in the formation of membrane-bound structures in cells and therefore, play a key role in the wear-and-tear mechanism of cellular growth. 93 Lipid profiling in individuals with AAS abuse revealed an increased amount of free fatty acids and glycerophospholipids. This increase is associated with odd-numbered chain fatty acids and/or arachidonic acid. 94 Notably, AAS influences HDL-cholesterol dynamics by enhancing hepatic lipase activity, which plays a pivotal role in HDL particle size conversion from HDL2 to HDL3, with even relatively low AAS dosages contributing to significant reductions in HDL-cholesterol level. 95 Administration of a low dosage of almost 6 mg per day of AAS compound for 2 weeks has shown a reduction of up to 20% in HDL-cholesterol levels in HL deficiency. 61 Reduction in HDL and increase in LDL and triglyceride levels have shown a predisposition to adverse cardiovascular events, thereby reflecting its adverse effects on the cardiovascular system.
Cardiovascular Risks Associated with AAS Abuse
Adverse events associated with AAS use are widely studied for the cardiovascular system. In general, cardiomyopathy, myocardial infarction, and fatal arrhythmias have been reported with AAS use. 96 An increase in Tp-e interval, Tp-e/QT ratio, and Tp-e/QTc ratio has been implemented in the pathophysiology of ventricular arrhythmias caused by AAS use, with reports of sudden death. 97 Cardiomyopathy in response to AAS use is also contributed by the increase of heart chamber diameters, changes in ventricular relaxation via altered diastolic function, and alterations in left ventricular contractility at the subclinical level. 98 , 99
Neurohumoral responses from AAS include a transient increase in blood pressure, yet, clinically significant hypertension is still to be established. The mechanism postulated to be involved in alteration in neurohumoral response includes an increase in systolic blood pressure with a decrease in plasma MR-proANP levels. 100 On the other hand, suppression of testosterone in men has shown an increase in NY-proBNP levels, which were restored by testosterone replacement, thereby formulating the role of testosterone in circulating natriuretic peptide levels. 101 Also, there have been reports of a link between AAS abuse and aortic stiffness that can be partly explained by their effects on platelet function and neurohumoral responses together. 102
Platelet function in response to AAS abuse involves a pronounced pro-thrombotic state, reflected by the increase in platelet aggregation. 103 Parallel coagulatory responses from the humoral regulation lead to a more complex pro-coagulator state characterized by the activation of pro-coagulatory and fibrinolytic pathways. Among these AAS, nandrolone specifically has shown a tendency to accelerate clot development and firmness in Wistar rats. 104 This might explain evident alterations in endothelial-dependent or independent vasodilation resulting in clot formation. 105
Additionally, the altered lipid metabolism, as discussed above, sets a foundation for the development of atherosclerosis and hypertension, 106 alongside an accelerated coagulation cascade, further exacerbating the condition. Persistent use of AAS therefore shows an association with myocardial dysfunction and accelerated coronary atherosclerosis. Such adverse events associated with AAS abuse are wreaking havoc on the current prevalence of cardiovascular events, without the recognition of AAS abuse as a public health concern. 107
Effects on Kidney
Effects of AAS on kidneys have been categorized as either direct or indirect effects. 108 While indirect effects are linked to cardiovascular or muscular abnormalities discussed above, direct effects refer to focal segmental glomerulosclerosis, acute kidney injury, and predisposition to chronic kidney injury. 109 Creatinine is a biochemical marker of kidney functioning and AAS use has shown transient small increases in serum creatinine concentrations (1.05 mg/Dl to 1.11 mg/dL) however, this increase remained clinically insignificant and returned to baseline after discontinuation of AAS use. 110 Comparatively, a larger increase in serum creatinine levels was observed in a placebo-controlled trial for a 4-week long duration, with resistance-trained men. These subjects were randomized to either a daily dose of 330 mg of oral prohormone 3β-hydroxy-5α-androst-1-en-17-one (1-androsterone) or placebo, 111 thereby reflecting alteration in renal function. Nandrolone decanoate abuse can cause aldosterone and electrolyte imbalance in the body which could be a serious risk factor for cardiovascular-related disorders. 112 The impact of AAS on kidneys has been categorized into direct and indirect effects, with indirect effects being linked to the cardiovascular or muscular abnormalities discussed earlier, and direct effects encompassing conditions like focal segmental glomerulosclerosis, acute kidney injury, and susceptibility to chronic kidney injury. 5
Effects of AAS Abuse on Sexual Functions
Testosterone, a reproductive hormone in males is known to be involved in metabolism where it enhances basal metabolic rate (BMR) at pharmacological doses. 113 As discussed earlier, it also has an impact on fat metabolism, thereby exerting its direct effects on the metabolism of reproductive hormones as well. Supraphysiological doses of AAS downregulate testosterone production. 114 Also, the external administration of testosterone in turn suppresses the hypothalamic-pituitary axis. It consequently translates into erectile dysfunction, violent tendencies, and decreased libido. Sexual dysfunction resulting from AAS abuse involves anabolic steroid-induced hypogonadism which includes azoospermia and testicular atrophy. 115 In males with ≤ 1 year of AAS abuse, withdrawal of AAS may suffice to normalize testosterone levels, but for abuse exceeding one year, additional therapy with clomiphene or gonadotropin may be needed to restore spermatogenesis. 107
Effects on Brain
AAs work by activating dopamine pathways in the brain. Specifically, testosterone acts through the mesolimbic dopamine system, which serves as a common platform in the brain for dependence on drugs of abuse. 116 Instead, testosterone resembles other mild reinforcers, such as caffeine, nicotine, or benzodiazepines. The potential for androgen addiction remains to be determined. These pathways are known for reward mechanisms in the brain, making them prone to developing dependence. 117 Also, AAS has been linked to modification in some indirect pathways including serotonergic, glutamatergic, and dopaminergic pathways in the lateral-anterior hypothalamus, translating into aggressive behavior. 118 , 119 AAS dependence arises from androgen reinforcement in the brain, which is comparatively lower than that of cocaine or heroin. 120 Reinforcements induced by caffeine, nicotine, or benzodiazepines instead are comparable to those induced by AAS. 121 Yet the AAS dependence requires further probing due to the adverse events associated with it. AAS dependence in males has exhibited thinning in the brain-wide cortical regions, in particular the pre-frontal cortex which is responsible for inhibitory control and emotional regulation. 122 Increased anxiety associated with chronic AAS use involves a direct amygdala-fugal pathway which forms the connection between the central nucleus of the amygdala and brainstem. In normal conditions, this pathway is responsible for cognitive-emotive and homeostatic processes. Among AAS, nalbuphine has shown some degree of dependence predisposing it as a drug of abuse among athletes. Consequently, nalbuphine’s scheduling status has been recommended for re-evaluation. 123
Psychological Complications Arising from AAS Abuse
Psychological complications with the use of AAS have brought about an area of concern that needs to be addressed with rising global mental health challenges. AAS use has been shown to cause an increase in aggression and hostility. 124 , 125 Some studies report mood disturbance about the type and dosage of AAS. 126 The AAS abuse population at risk of psychopathic traits includes bodybuilders with a prior history of AAS use. Also, sexual and substance use risk-taking behaviors and anger problems, are widely observed in bodybuilders with AAS use history as compared with non-users. 127 Since AAS use enhances aesthetic appeal by increasing muscle strength, withdrawal brings about concerns related to the body image of a person, resulting in social physique anxiety, however, this effect has been observed in more severe symptoms of AAS abuse including depression and withdrawal. 128 Yet, AAS dependence or withdrawal symptoms like depressed mood have been observed in a small number of AAS users. Also, reverse anorexia syndrome may develop with a dissatisfied body image and low self-esteem in the individuals using AAS, which predisposes such persons to resume the use of AAS. 129 So far, only 37.12% of people have shown interest in seeking support from physicians regarding AAS dependence which calls for the need to appreciate seeking help regarding AAS dependence. 130 They can lead to early heart attacks, strokes, liver tumors, kidney failure, and psychiatric problems. In addition, stopping use can cause depression, often leading to resumption of use.
Cellular and metabolic complications arising from anabolic steroid misuse have raised a recent public health concern. Health complications arising from anabolic steroid misuse have unveiled an occult cause of metabolic derangements in the younger population. Most studies have deciphered mechanisms where AAS activates common downstream signaling molecules like Akt, explaining unwanted events arising from AA abuse. AAS abuse has shown critical damage to cardiovascular, excretory, reproductive, muscular, hepatic, and nervous systems. Studies on AAS-related adverse effects have also brought about a connection with psychiatric disorders, thereby opening an area of interest for the causative factors of psychiatric disorders. Much is yet to be explored on how overt or occult AAS abuse defines certain behaviors in a normal individual. Can AAS play a role in defining behaviors that are generally attributed to a person’s own choice of behavior or are they influenced by such drugs of abuse needs to be explored to better understand male psychology. Moreover, health complications arising from AAS abuse like gynecomastia, acne, etc. also raise concern over AAS’s potential as a useful drug. While AAS abuse has been linked to many disorders affecting different organs in the body, it is interesting to observe that the effects of AAS have remained largely positive on bone growth. Reports on damage to tendons or ligaments exist, yet the effects of AAS remain largely beneficial for the skeletal system. Further probing into its mechanisms of action on bone growth may be useful for understanding the reason for its limited adverse effects on them. Moreover, clinical studies utilizing AAS for enhancing fracture repair in different ages and different kinds of fractures may provide useful insight into its clinical use. Conclusively, while AAS abuse has proven to be associated with many health complications, its effectiveness in treating skeletal disorders is largely unexplored. Probing its effectiveness for bone-related disorders with careful monitoring may offer a new mode of treatment for accelerated healing from complicated skeletal disorders.
Acknowledgments
The authors are thankful to Dr Noor Bahadar for reviewing the manuscript and suggesting grammatical corrections.
The authors report no conflicts of interest in this work.
Introducing Apple’s On-Device and Server Foundation Models
At the 2024 Worldwide Developers Conference , we introduced Apple Intelligence, a personal intelligence system integrated deeply into iOS 18, iPadOS 18, and macOS Sequoia.
Apple Intelligence is comprised of multiple highly-capable generative models that are specialized for our users’ everyday tasks, and can adapt on the fly for their current activity. The foundation models built into Apple Intelligence have been fine-tuned for user experiences such as writing and refining text, prioritizing and summarizing notifications, creating playful images for conversations with family and friends, and taking in-app actions to simplify interactions across apps.
In the following overview, we will detail how two of these models — a ~3 billion parameter on-device language model, and a larger server-based language model available with Private Cloud Compute and running on Apple silicon servers — have been built and adapted to perform specialized tasks efficiently, accurately, and responsibly. These two foundation models are part of a larger family of generative models created by Apple to support users and developers; this includes a coding model to build intelligence into Xcode, as well as a diffusion model to help users express themselves visually, for example, in the Messages app. We look forward to sharing more information soon on this broader set of models.
Our Focus on Responsible AI Development
Apple Intelligence is designed with our core values at every step and built on a foundation of groundbreaking privacy innovations.
Additionally, we have created a set of Responsible AI principles to guide how we develop AI tools, as well as the models that underpin them:
- Empower users with intelligent tools : We identify areas where AI can be used responsibly to create tools for addressing specific user needs. We respect how our users choose to use these tools to accomplish their goals.
- Represent our users : We build deeply personal products with the goal of representing users around the globe authentically. We work continuously to avoid perpetuating stereotypes and systemic biases across our AI tools and models.
- Design with care : We take precautions at every stage of our process, including design, model training, feature development, and quality evaluation to identify how our AI tools may be misused or lead to potential harm. We will continuously and proactively improve our AI tools with the help of user feedback.
- Protect privacy : We protect our users' privacy with powerful on-device processing and groundbreaking infrastructure like Private Cloud Compute. We do not use our users' private personal data or user interactions when training our foundation models.
These principles are reflected throughout the architecture that enables Apple Intelligence, connects features and tools with specialized models, and scans inputs and outputs to provide each feature with the information needed to function responsibly.
In the remainder of this overview, we provide details on decisions such as: how we develop models that are highly capable, fast, and power-efficient; how we approach training these models; how our adapters are fine-tuned for specific user needs; and how we evaluate model performance for both helpfulness and unintended harm.

Pre-Training
Our foundation models are trained on Apple's AXLearn framework , an open-source project we released in 2023. It builds on top of JAX and XLA, and allows us to train the models with high efficiency and scalability on various training hardware and cloud platforms, including TPUs and both cloud and on-premise GPUs. We used a combination of data parallelism, tensor parallelism, sequence parallelism, and Fully Sharded Data Parallel (FSDP) to scale training along multiple dimensions such as data, model, and sequence length.
We train our foundation models on licensed data, including data selected to enhance specific features, as well as publicly available data collected by our web-crawler, AppleBot. Web publishers have the option to opt out of the use of their web content for Apple Intelligence training with a data usage control.
We never use our users’ private personal data or user interactions when training our foundation models, and we apply filters to remove personally identifiable information like social security and credit card numbers that are publicly available on the Internet. We also filter profanity and other low-quality content to prevent its inclusion in the training corpus. In addition to filtering, we perform data extraction, deduplication, and the application of a model-based classifier to identify high quality documents.
Post-Training
We find that data quality is essential to model success, so we utilize a hybrid data strategy in our training pipeline, incorporating both human-annotated and synthetic data, and conduct thorough data curation and filtering procedures. We have developed two novel algorithms in post-training: (1) a rejection sampling fine-tuning algorithm with teacher committee, and (2) a reinforcement learning from human feedback (RLHF) algorithm with mirror descent policy optimization and a leave-one-out advantage estimator. We find that these two algorithms lead to significant improvement in the model’s instruction-following quality.
Optimization
In addition to ensuring our generative models are highly capable, we have used a range of innovative techniques to optimize them on-device and on our private cloud for speed and efficiency. We have applied an extensive set of optimizations for both first token and extended token inference performance.
Both the on-device and server models use grouped-query-attention. We use shared input and output vocab embedding tables to reduce memory requirements and inference cost. These shared embedding tensors are mapped without duplications. The on-device model uses a vocab size of 49K, while the server model uses a vocab size of 100K, which includes additional language and technical tokens.
For on-device inference, we use low-bit palletization, a critical optimization technique that achieves the necessary memory, power, and performance requirements. To maintain model quality, we developed a new framework using LoRA adapters that incorporates a mixed 2-bit and 4-bit configuration strategy — averaging 3.5 bits-per-weight — to achieve the same accuracy as the uncompressed models.
Additionally, we use an interactive model latency and power analysis tool, Talaria , to better guide the bit rate selection for each operation. We also utilize activation quantization and embedding quantization, and have developed an approach to enable efficient Key-Value (KV) cache update on our neural engines.
With this set of optimizations, on iPhone 15 Pro we are able to reach time-to-first-token latency of about 0.6 millisecond per prompt token, and a generation rate of 30 tokens per second. Notably, this performance is attained before employing token speculation techniques, from which we see further enhancement on the token generation rate.
Model Adaptation
Our foundation models are fine-tuned for users’ everyday activities, and can dynamically specialize themselves on-the-fly for the task at hand. We utilize adapters, small neural network modules that can be plugged into various layers of the pre-trained model, to fine-tune our models for specific tasks. For our models we adapt the attention matrices, the attention projection matrix, and the fully connected layers in the point-wise feedforward networks for a suitable set of the decoding layers of the transformer architecture.
By fine-tuning only the adapter layers, the original parameters of the base pre-trained model remain unchanged, preserving the general knowledge of the model while tailoring the adapter layers to support specific tasks.
We represent the values of the adapter parameters using 16 bits, and for the ~3 billion parameter on-device model, the parameters for a rank 16 adapter typically require 10s of megabytes. The adapter models can be dynamically loaded, temporarily cached in memory, and swapped — giving our foundation model the ability to specialize itself on the fly for the task at hand while efficiently managing memory and guaranteeing the operating system's responsiveness.
To facilitate the training of the adapters, we created an efficient infrastructure that allows us to rapidly retrain, test, and deploy adapters when either the base model or the training data gets updated. The adapter parameters are initialized using the accuracy-recovery adapter introduced in the Optimization section.
Performance and Evaluation
Our focus is on delivering generative models that can enable users to communicate, work, express themselves, and get things done across their Apple products. When benchmarking our models, we focus on human evaluation as we find that these results are highly correlated to user experience in our products. We conducted performance evaluations on both feature-specific adapters and the foundation models.
To illustrate our approach, we look at how we evaluated our adapter for summarization. As product requirements for summaries of emails and notifications differ in subtle but important ways, we fine-tune accuracy-recovery low-rank (LoRA) adapters on top of the palletized model to meet these specific requirements. Our training data is based on synthetic summaries generated from bigger server models, filtered by a rejection sampling strategy that keeps only the high quality summaries.
To evaluate the product-specific summarization, we use a set of 750 responses carefully sampled for each use case. These evaluation datasets emphasize a diverse set of inputs that our product features are likely to face in production, and include a stratified mixture of single and stacked documents of varying content types and lengths. As product features, it was important to evaluate performance against datasets that are representative of real use cases. We find that our models with adapters generate better summaries than a comparable model.
As part of responsible development, we identified and evaluated specific risks inherent to summarization. For example, summaries occasionally remove important nuance or other details in ways that are undesirable. However, we found that the summarization adapter did not amplify sensitive content in over 99% of targeted adversarial examples. We continue to adversarially probe to identify unknown harms and expand our evaluations to help guide further improvements.
In addition to evaluating feature specific performance powered by foundation models and adapters, we evaluate both the on-device and server-based models’ general capabilities. We utilize a comprehensive evaluation set of real-world prompts to test the general model capabilities. These prompts are diverse across different difficulty levels and cover major categories such as brainstorming, classification, closed question answering, coding, extraction, mathematical reasoning, open question answering, rewriting, safety, summarization, and writing.
We compare our models with both open-source models (Phi-3, Gemma, Mistral, DBRX) and commercial models of comparable size (GPT-3.5-Turbo, GPT-4-Turbo) 1 . We find that our models are preferred by human graders over most comparable competitor models. On this benchmark, our on-device model, with ~3B parameters, outperforms larger models including Phi-3-mini, Mistral-7B, and Gemma-7B. Our server model compares favorably to DBRX-Instruct, Mixtral-8x22B, and GPT-3.5-Turbo while being highly efficient.
We use a set of diverse adversarial prompts to test the model performance on harmful content, sensitive topics, and factuality. We measure the violation rates of each model as evaluated by human graders on this evaluation set, with a lower number being desirable. Both the on-device and server models are robust when faced with adversarial prompts, achieving violation rates lower than open-source and commercial models.
Our models are preferred by human graders as safe and helpful over competitor models for these prompts. However, considering the broad capabilities of large language models, we understand the limitation of our safety benchmark. We are actively conducting both manual and automatic red-teaming with internal and external teams to continue evaluating our models' safety.
To further evaluate our models, we use the Instruction-Following Eval (IFEval) benchmark to compare their instruction-following capabilities with models of comparable size. The results suggest that both our on-device and server model follow detailed instructions better than the open-source and commercial models of comparable size.
We evaluate our models’ writing ability on our internal summarization and composition benchmarks, consisting of a variety of writing instructions. These results do not refer to our feature-specific adapter for summarization (seen in Figure 3 ), nor do we have an adapter focused on composition.
The Apple foundation models and adapters introduced at WWDC24 underlie Apple Intelligence, the new personal intelligence system that is integrated deeply into iPhone, iPad, and Mac, and enables powerful capabilities across language, images, actions, and personal context. Our models have been created with the purpose of helping users do everyday activities across their Apple products, and developed responsibly at every stage and guided by Apple’s core values. We look forward to sharing more information soon on our broader family of generative models, including language, diffusion, and coding models.
[1] We compared against the following model versions: gpt-3.5-turbo-0125, gpt-4-0125-preview, Phi-3-mini-4k-instruct, Mistral-7B-Instruct-v0.2, Mixtral-8x22B-Instruct-v0.1, Gemma-1.1-2B, and Gemma-1.1-7B. The open-source and Apple models are evaluated in bfloat16 precision.
Related readings and updates.
Advancing speech accessibility with personal voice.
A voice replicator is a powerful tool for people at risk of losing their ability to speak, including those with a recent diagnosis of amyotrophic lateral sclerosis (ALS) or other conditions that can progressively impact speaking ability. First introduced in May 2023 and made available on iOS 17 in September 2023, Personal Voice is a tool that creates a synthesized voice for such users to speak in FaceTime, phone calls, assistive communication apps, and in-person conversations.
Apple Natural Language Understanding Workshop 2023
Earlier this year, Apple hosted the Natural Language Understanding workshop. This two-day hybrid event brought together Apple and members of the academic research community for talks and discussions on the state of the art in natural language understanding.
In this post, we share highlights from workshop discussions and recordings of select workshop talks.

Discover opportunities in Machine Learning.
Our research in machine learning breaks new ground every day.
Work with us
- SUGGESTED TOPICS
- The Magazine
- Newsletters
- Managing Yourself
- Managing Teams
- Work-life Balance
- The Big Idea
- Data & Visuals
- Reading Lists
- Case Selections
- HBR Learning
- Topic Feeds
- Account Settings
- Email Preferences
Research: The Most Common DEI Practices Actually Undermine Diversity
- Traci Sitzmann,
- Shoshana Schwartz,
- Mary Lee Stansifer

Organizations over-rely on approaches that consistently fail to diversify management ranks — and overlook those that have proven effective.
While companies say they champion diversity, there are glaring disparities in diverse representation within managerial ranks. The authors examine the impact of various management practices on diverse representation in managerial roles and how often each management practice is utilized in organizations, shedding light on why organizations are not making greater progress toward diverse representation. Despite not working well for attaining diverse representation, diversity training is widely used in organizations. In contrast, formal mentoring programs and targeted recruitment are effective for increasing diverse representation but are underused. Indeed, the relationship between how often management practices are implemented in organizations and their effectiveness in attaining diverse representation is negative and strong. This article breaks down the practices organizations should utilize to achieve diverse representation, underscoring the need to shift toward practices that increase diverse representation in management.
Despite the U.S. population’s growing diversity , managerial roles are still predominantly held by white men. While the largest firms have been pledging to recruit and train Black workers for over 40 years, there has been little increase in Black representation in managerial roles during this timeframe. In a 2021 analysis , Black employees held only 7% of managerial roles despite comprising 14% of all employees. Women have difficulty attaining leadership roles despite evidence that “women are more likely than men to lead in a style that is effective.”
- TS Traci Sitzmann is a Professor of Management and Workforce Development Scholar at the University of Colorado Denver.
- SS Shoshana Schwartz is an Assistant Professor of Management at Christopher Newport University’s Luter School of Business.
- MS Mary Lee Stansifer is an Assistant Teaching Professor at the University of Colorado Denver.
Partner Center
News & Events
Next-generation aerospace research on display.
Amy Sprague June 17, 2024
The annual A&A Graduate Research Showcase highlighted cutting-edge projects, with awards for work on plasma modeling, hypersonics, and more.
Scenes from the graduate research poster presentations, including Joshua Cheng (left) showing how April Tags work and Kuang-Ying ("Eddie") Ting (center) with his poster on flutter suppression.
A&A held its annual Graduate Research Showcase on May 20th as part of SHARC Week 2024. Graduate students presented 15 projects through lightning talks and poster sessions, displaying the cutting-edge work happening in our labs. The posters presented a wide range of research in the department. Four presenters received awards from our Judges Panel and the People’s Choice.
Showcase winners
First place: Landon Bevier
Helicon mode transition scaling laws.
Landon Bevier presented research out of SPACE Lab on radio frequency plasma coupling in electric propulsion systems. Bevier developed and validated a model to predict the transition between different energy coupling modes based on electron temperature, density, and plasma radius. Direct wave measurements using specialized probes confirmed the model's accuracy.

Second place: Paul Medina
Analysis of jets in hypersonic crossflow using focused laser differential interferometry (fldi).
Paul Medina presented his work out of the Williams Turbulence Lab on using focused laser differential interferometry (FLDI) to analyze jets in hypersonic crossflow. FLDI provides high spatial and temporal resolution density measurements non-invasively. Medina's goals are to measure turbulence statistics with FLDI and optimize the optical components for multi-point measurements.
Third place: Jiacheng Chen and Collins Davis
Development of novel thermoplastic orthotic springs made from repurposed materials.
Collins Davis and Jiacheng Chen presented their work out of the MAMS Lab to create lightweight, affordable orthotic springs from recycled composite fibers in a thermoplastic Nylon-6 matrix through compression molding. Detailed material and thermal modeling is key to achieving uniform properties.

People’s Choice: Thijs Masmeijer
Displacement estimation with directional dic with automatic feature selection.
Thijs Masmeijer presented his work out of the Illimited Lab to develop an enhanced digital image correlation (DIC) technique that enables full-field displacement measurements on surfaces without an applied speckle pattern. This is enabled by using a pre-defined displacement direction to overcome the aperture problem. The method includes an approach for automatic selection of trackable features making the method more accessible.
"Our students continue to impress with the quality and innovation in their research projects," said Professor Antonino Ferrante who hosted the event. "We're proud of their achievements and excited to see how their work shapes the future of aerospace."
Congratulations to all the participants in making the 2024 A&A Graduate Research Showcase a success! A special thanks to our judges, Professor Amir Taghvai and alumni Lauren Jones from Alaska Airlines, Taylor Reynolds from Amazon Prime Air and Danny Crews from Zap Energy.
Explore all of our graduate research posters
Optimal trajectory generation using transformers, nonlinear filtering with optimal transport, mohammad al-jarrah, plunge dynamics: compliance to reduce diving impact forces, bart boom, with tadd truscott, adam summers, frank fish, ed habtour, advances in deferred-decision trajectory optimization (ddto), samuel buckner (presenter) and purnanand elango, with behcet acikmese, optimal fiducial marker placement for satellite proximity operations, joshua cheng (presenter) and nicholas andrews, numerical simulation of liquid oxygen droplet combustion in hydrogen in microgravity, benjamin davis (presenter), noelia figueira, phani ponduri, and mukund gupta, aircraft approach and landing trajectory optimization for a 6-dof aircraft with a runway alignment constraint, static response and failure prediction of anisotropic material extrusion of polymer parts, jiahao lu (presenter) and grace dojan, enhancement of cryogenic pool boiling by surface modification, shuba murthy (presenter) and andrew jacob, with jim hemanson, robust trajectory planning under state- and input-dependent uncertainty, oliver sheridan, wind tunnel aeroservoelasticity active gust load alleviation and flutter suppression, kuang-ying “eddie” ting (presenter) and john berg, with francesco toffol, nicola fonzi, servio ricci, marat mor and kristi morganson.
IMAGES
VIDEO
COMMENTS
Anabolic-androgenic steroids, often shortened to "anabolic steroids," "steroids," or "androgens," 2,3 are the most widely misused APED. These are synthetic substances similar to the male sex hormone testosterone. They promote the growth of skeletal muscle (anabolic effects) and the development of male sexual characteristics (androgenic effects) in both males and females. 2
Steroids are complex lipophilic molecules that have many actions in the body to regulate cellular, tissue and organ functions across the life-span. Steroid hormones such as cortisol, aldosterone, estradiol and testosterone are synthesised from cholesterol in specialised endocrine cells in the adrenal gland, ovary and testis, and released into ...
Anabolic-androgenic steroids (AAS) are a class of natural and synthetic hormones that owe their name to their chemical structure (the steroid nucleus, see Figure 1 ) and the biological effects (anabolic and androgenic) they induce. Anabolic refers to the skeletal muscle-building properties of AAS, whereas androgenic refers to the induction ...
The antiinflammatory properties of steroids have been attributed to their inhibitory effects on the action of phospholipase A2, an enzyme critical to the production of inflammatory compounds. 22 Research has shown that steroids are active in affecting gene expression, translation, and enzyme activity. 23 In short, they bring about their ...
SYNOPSIS This consensus statement is an update of the previous position stand from the American College of Sports Medicine (ACSM), published in 1987 ().Since then, a substantial amount of scientific data on anabolic-androgenic steroids (AAS) has emerged and the circumstances of AAS use has evolved in the athletic, recreational, and clinical communities.
Early work indicated that nuclear steroid receptors require common cofactors that constitute a limiting factor when ... a full line of research established that all steroid-synthesizing enzymes that are needed to synthesize sex steroids from cholesterol are expressed in the brain that should thus also be considered as an endocrine ...
Background: Since their identification nearly 80 years ago, steroids have played a prominent role in the treatment of many disease states. Many of the clinical roles of steroids are related to their potent antiinflammatory and immune-modulating properties. Methods: This review summarizes the basic pharmacology, complications, and practice delivery issues regarding steroids.
However, the large dynamic range to be covered, the low natural abundance of some key steroids, the selectivity of the analytical methods, the extraction protocols, and the steroid ionization remain some of the current challenges in steroid analysis. This review provides an overview of the different analytical workflows available depending on ...
STEROIDS is an international research journal devoted to studies on all chemical and biological aspects of steroidal moieties. The journal focuses on both experimental and theoretical studies on the biology, chemistry, biosynthesis, metabolism, molecular biology, physiology and pharmacology of …. View full aims & scope.
Athletes often take androgenic steroids in an attempt to increase their strength. The efficacy of these substances for this purpose is unsubstantiated, however. We randomly assigned 43 normal men t...
ACTVR.2023.13(4).128-131. Steroids, also known as corticosteroids or glucocorticoids, are synthetic drugs that mimic the actions of naturally occurring hormones in the body. In clinical practice, steroids have a wide range of therapeutic applications due to their potent anti-inflammatory, immunosuppressive, and metabolic efects.
Anabolic-androgenic steroids (AAS) are a class of hormones that are widely abused for their muscle-building and strength-increasing properties in high, nontherapeutic, dosages. This review ...
The article by Kapoor et al. and the accompanying editorial highlight the important issue of the usage of corticosteroids along with immunotherapy in advanced cancers.[1 2]. The use of steroids with immunotherapy is inevitable in certain situations. With the approval of immunotherapy combined with chemotherapy as the best first-line option in advanced non-small cell lung cancer, the use of ...
1) Steroids, physiologically, work. This much is not debatable. 2) On top of how well they work physiologically, a major factor is how well they work psychologically - if you do something expecting to get a ton stronger, there's a good chance you'll get a ton stronger. This applies to much more than steroids.
Description. Research on Steroids contains the proceedings of the Fourth Meeting of the International Study Group for Steroid Hormones. The papers explore the production, chemical characterization, and metabolism of steroid hormones and their interactions with proteins. Topics range from the action of estradiol in vitro to water-soluble ...
Side effects depend on the dose of medication you receive and may include: A buildup of fluid, causing swelling in your lower legs. High blood pressure. Problems with mood swings, memory, behavior, and other psychological effects, such as confusion or delirium. Upset stomach.
Corticosteroids are drugs used in the management and treatment of almost all areas of medicine. This activity outlines the indications, action, and contraindications for corticosteroids as a valuable agent in managing numerous disorders. This activity will highlight the mechanism of action, adverse side effects profile, and other key factors (e.g., off-label uses, dosing, pharmacodynamics ...
Anabolic steroids (artificial androgens) work by activating androgen receptors in your body and mimicking the effects of natural androgens. Prescription anabolic steroids work in different ways to treat conditions. For example: For people who have naturally low testosterone levels, prescription anabolic steroids return their testosterone levels ...
Health risks. Withdrawal. Anabolic steroids are used for some medical conditions, but people also use them illegally in some sports settings. Different types include bulking, performance, and ...
It's definitely the middle-aged white dude at work who calls you brother, who takes beta blockers before presentations—the same guy who texted you about T, testosterone, a.k.a. test, because ...
discusses his research, including his work on steroids. Student Activities with Objectives History Exercise: Chronology of Steroid Medicine Research (15-20 min.) Using the handout, students place major events from the research and development of steroid medicines from the 1920s to the 1990s.
Knowledge workers attend an astounding number of meetings, many of which aren't a good use of their time. According to recent research from Microsoft, inefficient meetings are the number one ...
Steroids remain indispensable in clinical practice, playing a vital role in managing a wide range of medical conditions [ 1, 2 ]. Their potent anti-inflammatory and immunosuppressive effects make them valuable tools for alleviating symptoms and improving patients' quality of life. However, healthcare professionals must carefully consider the ...
Enjoying work matters — a lot. Our earlier research has shown that employees who enjoy their work are about 50% less likely to look for a new job.But increasing this emotion is about more than ...
While much has been said about the potential benefits of remote work for women, recent research examines how working from home affects the professional development of female software engineers at ...
AAs work by activating dopamine pathways in the brain. Specifically, testosterone acts through the mesolimbic dopamine system, which serves as a common platform in the brain for dependence on drugs of abuse. 116 Instead, testosterone resembles other mild reinforcers, such as caffeine, nicotine, or benzodiazepines. The potential for androgen ...
Figure 1: Modeling overview for the Apple foundation models. Pre-Training. Our foundation models are trained on Apple's AXLearn framework, an open-source project we released in 2023.It builds on top of JAX and XLA, and allows us to train the models with high efficiency and scalability on various training hardware and cloud platforms, including TPUs and both cloud and on-premise GPUs.
New research looks at how persevering through tedious work can make you less productive in subsequent tasks. Here's an alternative approach.
Summary. While companies say they champion diversity, there are glaring disparities in diverse representation within managerial ranks. The authors examine the impact of various management ...
A&A held its annual Graduate Research Showcase on May 20th as part of SHARC Week 2024. Graduate students presented 15 projects through lightning talks and poster sessions, displaying the cutting-edge work happening in our labs. The posters presented a wide range of research in the department.