- Open access
- Published: 05 September 2019

Efficacy of a compulsory homework programme for increasing physical activity and improving nutrition in children: a cluster randomised controlled trial
- Scott Duncan ORCID: orcid.org/0000-0002-8402-2930 1 ,
- Tom Stewart 1 ,
- Julia McPhee 1 ,
- Robert Borotkanics 1 ,
- Kate Prendergast 1 ,
- Caryn Zinn 1 ,
- Kim Meredith-Jones 2 ,
- Rachael Taylor 2 ,
- Claire McLachlan 3 &
- Grant Schofield 1
International Journal of Behavioral Nutrition and Physical Activity volume 16 , Article number: 80 ( 2019 ) Cite this article
5746 Accesses
20 Citations
24 Altmetric
Metrics details
Most physical activity interventions in children focus on the school setting; however, children typically engage in more sedentary activities and spend more time eating when at home. The primary aim of this cluster randomised controlled trial was to investigate the effects of a compulsory, health-related homework programme on physical activity, dietary patterns, and body size in primary school-aged children.
A total of 675 children aged 7–10 years from 16 New Zealand primary schools participated in the Healthy Homework study. Schools were randomised into intervention and control groups (1:1 allocation). Intervention schools implemented an 8-week applied homework and in-class teaching module designed to increase physical activity and improve dietary patterns. Physical activity was the primary outcome measure, and was assessed using two sealed pedometers that monitored school- and home-based activity separately. Secondary outcome measures included screen-based sedentary time and selected dietary patterns assessed via parental proxy questionnaire. In addition, height, weight, and waist circumference were measured to obtain body mass index (BMI) and waist-to-height ratio (WHtR). All measurements were taken at baseline (T 0 ), immediately post-intervention (T 1 ), and 6-months post-intervention (T 2 ). Changes in outcome measures over time were estimated using generalised linear mixed models (GLMMs) that adjusted for fixed (group, age, sex, group x time) and random (subjects nested within schools) effects. Intervention effects were also quantified using GLMMs adjusted for baseline values.
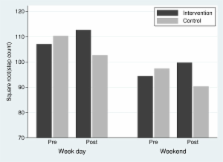
Significant intervention effects were observed for weekday physical activity at home (T 1 [ P < 0.001] and T 2 [ P = 0.019]), weekend physical activity (T 1 [P < 0.001] and T 2 [P < 0.001]), BMI (T 2 only [ P = 0.020]) and fruit consumption (T 1 only [ P = 0.036]). Additional analyses revealed that the greatest improvements in physical activity occurred in children from the most socioeconomically deprived schools. No consistent effects on sedentary time, WHtR, or other dietary patterns were observed.
Conclusions
A compulsory health-related homework programme resulted in substantial and consistent increases in children’s physical activity – particularly outside of school and on weekends – with limited effects on body size and fruit consumption. Overall, our findings support the integration of compulsory home-focused strategies for improving health behaviours into primary education curricula.
Trial registration
Australian New Zealand Clinical Trials Registry, ACTRN12618000590268 . Registered 17 April 2018.
Physical activity and healthy nutrition practices are essential for many aspects of child health and development [ 1 ], including the prevention of chronic health conditions in adolescence and adulthood [ 2 , 3 ]. However, evidence indicates that many children do not meet international physical activity and dietary guidelines [ 4 , 5 , 6 , 7 ], contributing to a rise in obesity and related comorbidities in later life [ 8 ]. The development, implementation, and evaluation of effective and sustainable initiatives that equip children to lead healthy and active lives has become a key public health priority in many countries [ 1 ]. Despite parents having a significant influence on children’s activity and eating patterns, exclusively home-based interventions are logistically impractical. The school setting may provide a unique opportunity for intervention delivery: intervention material can be wide-reaching, especially if made compulsory as part of the curriculum or integrated into school policy [ 9 , 10 , 11 ].
Several systematic reviews indicate that delivering interventions within school can improve several physical activity and diet behaviours in children [ 12 , 13 , 14 ]; however, these effects are often modest at best. Quality of evidence from past randomised controlled trials (RCTs) was criticised in a 2013 Cochrane Review and judged at moderate risk of bias—a reliance on self-reported outcomes, absence of longer term follow-up, lack of blinding, and failing to account for clustering during analyses being common problems [ 12 ]. Additional reviews have concluded that physical activity interventions have had only small to negligible measured effects on total and moderate-to-vigorous physical activity, whether assessed immediately post intervention or at six-month follow-up [ 15 , 16 ]. Nonetheless, evidence indicates that school-based physical activity and dietary interventions can be successful in improving indicators related to obesity in children [ 17 ].
To date, the majority of school-based physical activity/nutrition interventions have focused solely on the school environment [ 12 , 18 ], despite reviews indicating that multicomponent interventions involving the family or community in addition to the school are likely to be most effective [ 17 , 19 , 20 ]. Family support and parental restrictions can influence out-of-school physical activity [ 21 ], and the majority of food that children consume originates from the home [ 22 , 23 ]. Therefore, it is unlikely that long-term behaviour change is possible when the influences of the home environment are not addressed. The concept of curriculum-based physical activity or nutrition ‘homework’ is relatively under-utilised. Active for Life Year 5 (AFLY5) aimed to improve in-school and out-of-school physical activity and diet behaviours through professional learning and development for teachers coupled with in-class lessons and homework plans [ 24 ]. While positive effects on screen time and high energy drinks and snacks were observed, there were no significant effects on physical activity, fruit and vegetable consumption, or body size [ 25 , 26 ].
This paper presents the main findings from the Healthy Homework programme, an eight-week (approximately one school term) intervention designed to improve the physical activity and dietary behaviours of primary-aged children through a compulsory health-related homework schedule, supplemented with curriculum resources for teachers. This approach differs from many previous school-based interventions because the homework component was designed to maximise family engagement, theoretically improving the likelihood of success. Healthy Homework was developed in 2008 with oversight from New Zealand education and health professionals, and underwent extensive piloting in two primary schools [ 27 ]. Despite a small sample size, significant benefits were observed in physical activity and some dietary behaviours. Perhaps most importantly, focus groups revealed that the programme was highly valued by the children, their parents, and participating teachers [ 27 ]. We found that the level of family engagement exceeded expectations, and that the usability and utility of Healthy Homework for teachers was high [ 27 ].
Despite these encouraging results, several limitations were noted: the sample size was small limiting generalisability, the programme required updating to align with the New Zealand Curriculum, body size was not assessed, and the cluster unit was classroom (raising the possibility of between-group contamination). Therefore, the aim of this study was to determine the effects of an updated Healthy Homework programme on physical activity, nutrition, and body size in a large sample of New Zealand children randomised at the school level.
Participants
Due to the nature of the intervention, individual participants were accessed via primary (elementary) schools, which acted as the cluster unit in all subsequent analyses. Eligibility criteria for the schools were as follows: enrolment of over 100 students, location within Auckland or Dunedin cities, and a contributing, full primary, or composite structure that included at least one class each of students in school years 3–5. A total of 16 primary schools from Auckland ( n = 10) and Dunedin ( n = 6) were randomly selected to participate in the study from a sampling frame of all eligible schools. Socioeconomic decile ratings of participating schools (determined by the NZ Ministry of Education) ranged from 1 to 10 (where 1 indicates ‘low’ and 10 indicates ‘high’; median [IQR] = 8 [ 6 , 7 , 8 , 9 ]). After stratification by decile group (1–7 and 8–10), each school was randomly assigned into the intervention group ( n = 8) or the waitlisted control group (n = 8) by the lead researcher using a random number generator (concealed from participants; 1:1 allocation ratio). This stratification was implemented as only one Decile 1 school was recruited. Schools assigned to the control group were offered the intervention (including all resources) following the final assessment period. One Year 3, Year 4, and Year 5 class from each school were then selected to participate; simple random sampling was used in instances where there were two or more classes per year. Year 6 classes were excluded to permit final follow-up measurements. Enrolment occurred between 01/07/11 and 24/07/12, with measurements staggered across every calendar month (excluding January and December) and school term (1–4); the last follow-up measure occurred at 07/04/13. At the intervention schools, all children in the selected classes received the Healthy Homework programme as part of the schools’ curricula; however, parental consent was required before children were included in the intervention evaluation. All children in each participating class were invited to take part in the evaluation (i.e., no formal inclusion or exclusion criteria aside from consent/assent), which took place in school grounds. Parent information and consent forms were sent home with the children for completion and return. Ethical approval was obtained from the Auckland University of Technology (10/159) and University of Otago (11/084) Ethics Committees.
Based on reference data from the HH feasibility phase [ 27 ], we calculated that a target sample size of 800 children would enable us to detect the following differences in our outcome measures (α = 0.05, 1-β = 0.80): 1000 pedometer steps/day, 30 min.day − 1 of TV/computer time, 0.5 daily servings of fruit and vegetables, 0.5 daily servings of takeaway food, and a BMI z-score of 0.2. These calculations allow for school clustering effects (cluster size = 16; ICC = 0.04), correlation between repeated measures (0.4 for all behavioural variables and 0.8 for BMI z-score), and 25% dropout at each follow-up point.
Intervention design
The design and theoretical basis of the Healthy Homework programme is described in detail elsewhere [ 27 ] and only a brief summary is outlined here. Healthy Homework was an eight-week curriculum-based homework schedule, complemented by an in-class teaching resource, designed to promote physical activity and healthy eating in children (curriculum resources may be provided upon request). The programme was developed under the guidance of an advisory committee comprising experienced health and education professionals (including classroom teachers) with regular input from children and parents. Healthy Homework was based on several established behaviour change theories (including the theory of reasoned action, the theory of planned behaviour, and social-cognitive theory [ 28 ]), and was designed to support the achievement objectives associated with the Health and Physical Education strand of the New Zealand Curriculum [ 29 ]. The research team provided professional learning for the teachers of the three intervention classes at each intervention school, and to one lead teacher in each of the control schools (who were permitted to implement the programme at the conclusion of the final follow-up point). The professional learning protocol was standardised across all schools, and necessitated one half-day release per teacher. Approximately 90 min was spent providing information about the benefits of physical activity and a healthy diet for children’s overall health and development, and the results of previous strategies to integrate these topics into the primary school curriculum. An additional 90 min was spent introducing the teachers to the in-class and homework modules, discussing examples of how to complete tasks, and fielding questions about the programme delivery and evaluation.
At the start of the intervention, all children in participating classes received a homework booklet organised into weekly topics that each contained one physical activity and one nutrition component (e.g., walking and fruit/vegetables, screen time and breakfast, fitness and cooking). Three practical homework options were provided for each topic, and the children were directed by their teacher to complete at least one physical activity and one nutrition task per topic each week (e.g., organising family walks, walking to and from school, limiting screen time, testing the fitness of the family, eating 5+ fruit and vegetables each day, comparing food labels at the supermarket, helping with dinner, preparing a healthy lunch box). Blue or purple rubber wristbands were provided each week for children who completed their homework obligations, with a black colour reserved for those who completed all six tasks on a given week. The intention of the wristbands were to encourage the children to complete more than the minimum number of required tasks. The Healthy Homework classroom curriculum resource was designed to provide the teachers with sufficient educational content and in-class exercises for three 1.5-h sessions delivered on different days throughout each week (including one session reviewing the previous week’s homework). Furthermore, an online portal was developed and monitored to allow teachers to access resources and record student compliance, and to enable children to share homework-related updates with other participants (including those in other schools). Student and teacher modules can be downloaded as Additional files 2 and 3 .
Baseline measurements were taken prior to intervention delivery (T 0 ), and repeated immediately post-intervention (T 1 ) and six-months post-intervention (T 2 ), between August 2011 and April 2013. The team of research assistants responsible for data collection were not blinded to group allocation. Each research assistant was provided with an appropriate level of anthropometric training by experienced researchers prior to data collection.
Physical activity
Weekday physical activity at school, weekday physical activity at home, and weekend physical activity – treated as the primary outcome measures – were assessed using sealed NL-1000 pedometers (New Lifestyles Inc., Lee’s Summit, MO) over five consecutive days (three weekdays, two weekend days). These pedometers have a multiday memory function that automatically stores step counts by day of week for up to 7 days. Our previous research has established the validity of these pedometers for measuring steps in children, with mean percent bias less than 5% for typical walking speeds [ 30 ]. Two pedometers were assigned to each child: one clearly labelled ‘School’ and the other ‘Home’. The ‘School’ pedometer was worn during school hours, while the ‘Home’ pedometer was left inside a collection tray in the classroom. At the conclusion of the school day (approx. 3 pm), each child placed their ‘School’ pedometer in the tray and attached their ‘Home’ pedometer. At the beginning of the next weekday (approximately 9 am), the teacher reminded the children to switch over their pedometers again. Thus, before school and after school activities that were outside of the classroom were captured on the ‘Home’ pedometer. This approach was taken as it removed the need for teachers to coordinate a lengthy collection and handout process, and allowed the differentiation of in-school and out-of-school physical activity, while using a cost-effective but objective measurement device.
Dietary patterns
Key dietary patterns were estimated as secondary outcome measures using items extracted from the Children’s Dietary Questionnaire (CDQ), a parental proxy report that has been validated in children aged 4–16 years [ 31 ]. The CDQ focuses on patterns of food intake over the previous 24 h and/or 7 days rather than actual amounts and types of foods consumed. The questionnaire contained 33 items, 30 of which utilised categorical response options, and three of which utilised open-ended response options. A total of 20 questions referred to dietary patterns over the previous seven-days, 11 questions referred to dietary patterns over the previous 24-h, and two referred to specific meal questions (breakfast and lunch). The four dietary items selected for analyses in this study were: (1) daily fruit consumption, (2) daily vegetable consumption, (3) weekly fast food consumption, and (4) weekly soft drink consumption. These items were selected given their alignment with the New Zealand Food and Nutrition Guidelines, and the high prevalence of soft drink consumption in New Zealand youth [ 32 ]. A copy of the questionnaire may be provided upon request.
Television and computer usage
Two questions pertaining to the frequency and duration of television, computer and gaming console use were also amended to the questionnaire as additional secondary outcome measures. These questions asked parents to recall the amount of time each day (Monday to Sunday) their child spent (1) watching TV, DVDs, or videos, or (2) on the computer or games console (not including school-related work) in the previous week. The total time provided for Monday to Friday was averaged to provide a weekday TV/computer estimate, whereas Saturday and Sunday totals were averaged to provide a weekend estimate.
Standing height was measured to the nearest millimetre with a portable stadiometer (SECA 213, Hamberg, Germany) and weight was measured to the nearest 0.1 kg on a digital scale (SECA 813, Hamberg, Germany). Waist circumference was measured midway between the iliac crest (highest point of the pelvis at the side) and the lowest rib margin. Participants were asked to remove their shoes and any bulky external clothing (i.e. jackets, coats) prior to assessment. For all anthropometric measures, estimates were taken three times, with the average value used in subsequent analysis. Body mass index (BMI; secondary outcome measure) was calculated as weight (kg) divided by squared height (m 2 ), and waist-to-height ratio (WHtR; secondary outcome measure) was calculated as waist circumference (cm) divided by height (cm).
Statistical analysis
In the first instance, baseline characteristics of the sample were calculated and presented as mean ± standard deviation (SD), or median and interquartile range (IQR) in cases where the data were not normally distributed. Intention-to-treat analyses were used to test the efficacy of the intervention, regardless of adherence to homework tasks. To simplify analysis and interpretation of the dietary data, categorical CDQ subscales were converted into binary variables using thresholds that approximately balanced the number of responses in each category.
Changes in outcome variables were compared between intervention and control groups using generalised linear mixed models (GLMMs) that adjusted for fixed and random (subjects nested in schools) effects. This approach was taken to account for the intra-school correlations and intra-person correlations between the repeated measures. Outcomes were controlled for baseline measures and age. A gamma probability distribution and an log link function was applied for most outcome variables, the exception being weekday TV, which were evaluated using a Gaussian distribution and identity link function. Models predicted outcomes at completion of the intervention (T 1 ). Additional models predicted outcomes at 6 months post intervention (T 2 ). Marginal effects were evaluated on select variables. Descriptive analyses were conducted in IBM SPSS Statistics v23 (IBM Cooperation, USA) and GLMM’s were carried out using Stata V14 (Stata Corporation, USA).
The Healthy Homework intervention was conducted between August 2011 and August 2012. Figure 1 depicts participant allocation and retention across each phase of the study in the form of a CONSORT flow diagram. A total of 675 children (intervention = 171 boys and 175 girls; control = 155 boys and 174 girls) aged 7–10 years provided written parental consent and assent to participate in the evaluation (consent rate = 56.3%). Cluster size (i.e., the number of children from each school) ranged from 14 to 53 (median [IQR] = 47.5 [36.5, 50]). Absent days, changing school, and withdrawals resulted in 46 children that did not participate in the first follow up (T 1 ), and 67 children that did not participate in the second follow-up 6-months post intervention (T 2 ). However, 29 of the 46 children absent from T 1 returned for T 2 . The completed CONSORT checklist can be accessed as an Additional file 1 .

Participant allocation and retention
Table 1 shows the descriptive characteristics of the study sample. There were no meaningful differences in age, gender distribution, or physical activity between the intervention and control groups at baseline. However, the intervention group contained notably more participants from schools in lower SES areas, had a higher proportion of children from Maori and Pacific backgrounds, as well as slightly higher BMI, WHtR, and daily servings of vegetables. Overall, the sample averaged 5090 ± 2200 steps/day (mean ± SD) at home on weekdays, 5410 ± 2200 steps/day at school, and 7440 ± 4100 steps/day on weekends, with boys more active than girls. No systematic pattern emerged with regard to the missingness of the data. For outcomes reported by proxy questionnaire, the response rate at T3 averaged between 54 and 60%. We removed weekend activity from our secondary analyses because the response rates were below 50%. All other outcomes evaluated – BMI, weekday activity – had a response rate in excess of 70%.
Table 2 presents the results for the GLMMs. In general, the intervention group did not experience a statistically significant reduction in BMI immediately after the completion of the intervention (p: 0.755), but did demonstrate a statistically significant reduction in BMI at 6 months post intervention (p: 0.020). The predicted marginal mean of BMI in the control group at 6 months was 17.451; the intervention group, 17.274. However, marginal analyses revealed that those subjects that are likely to benefit most are students that have a baseline BMI of 17 or higher (Fig. 2 ), with a statistically significant difference between the intervention and control groups emerging at this point (β: − 0.267, z: − 2.19, p: 0.028, CI: − 0.017 − 0.001).

Predicted difference in BMI between study groups (univariate model)
Overall activity increased at T 1 and T 2 time points. This increase was statistically significant for weekday home and weekend activity (Table 2 ). School decile had exhibited a statistically significant impact on weekday home activity at T 1 , with the greatest improvements in weekday home activity occurring in the most socioeconomically deprived schools (Table 3 ). This increase persisted into T 2 , albeit attenuating to just outside of statistical significance (Table 3 ). Weekend television watching increased relative to baseline in those subjects from the most socioeconomically deprived schools at T 2 , and this difference was statistically significant (Table 3 ).
The adjusted model evaluating covariate effect on BMI at T 2 revealed that weekday home activity was the most significant covariate (Table 4 and Fig. 3 ). For each increase in 1000 steps, an almost 0.6 point decrease in BMI was realized. This model was adjusted for school decile. These decreases were most pronounced in the socioeconomically most deprived schools, where subject BMI decreased 0.476 points per 1000 steps, when controlling for other covariates. Proxy-reported vegetable consumption at T 2 was the second most important predictor of BMI reduction at T 2 , where each meal of vegetable consumed resulted in a 0.036 point decrease in BMI. It should be noted that weekend steps could not be evaluated with respect to school decile or BMI at T 2 , because only 39 and 47% matching observations were available (respectively).

Predicted difference in BMI between study groups (adjusted model)
In this study, we evaluated the efficacy of the Healthy Homework programme for improving physical activity, dietary patterns, and body size in primary-aged children. Despite being a school-based intervention, a key strength of this study was the design of a homework syllabus that maximised family participation and engagement, thereby targeting out-of-school behaviours. Our results demonstrate significant and sustained increases in physical activity 6-months post-intervention. Of particular note were the large effects on out-of-school physical activity, approximate to hypothetical increases of 15.6 and 29.7% (i.e., intervention effects compared to baseline values) each weekday and weekend day, respectively. This degree of improvement, should it persist over the long term, would likely have a meaningful impact on children’s health and wellbeing: reviews have identified favourable effects on a wide range of physical, psychosocial, and cognitive outcomes of even modest increases in physical activity [ 33 , 34 ]. Furthermore, the relatively larger effects observed in children from the most socioeconomically-deprived schools suggest that this intervention approach may be an effective way of engaging at-risk populations.
Significant intervention effects on BMI and fruit consumption were also observed, although the effects were smaller and inconsistent across time points. Intervention effects on BMI, in particular, were limited. No difference was observed at the end of the intervention, and although a statistically significant difference was observed between groups at T2, such a difference would not be deemed clinically relevant. It is possible that the follow-up time was insufficient to allow any improvements in physical activity to influence body size. Nonetheless, our findings provide some support for the development and implementation of resources that enhance family involvement in health-related curriculum areas.
Despite the positive effects for physical activity, we did not observe any meaningful changes in screen time or dietary patterns. The lack of effect on screen time may be explained by the relatively minor emphasis placed on this topic (only one session); however, half the module featured advice and activities relating to nutrition and diet. We did note via anecdotal feedback that the children appeared to prefer the physical activity topics over the nutrition topics, and perhaps this played a role in the lack of consistent dietary effects. It is possible that physical activity is a more malleable and less complex behaviour than diet in children [ 35 ], or that our questionnaire-based assessment of dietary intake was not sensitive enough to quantify meaningful changes in this sample. In any case, this study suggests that nutrition initiatives in primary schools may not achieve the same level of benefits as similar physical activity programmes.
One of the distinctive aspects of the intervention was its compulsory nature, with a number of key health messages grounded in the national school curriculum [ 29 ]. Although there is promising evidence that purely family-based intervention approaches can improve children’s physical activity and diet [ 36 , 37 ], teaching nutrition and physical activity within the primary-school curriculum provides a cost-effective method of reaching large numbers of children without the requirement of children or families to ‘opt-in’. Given the significant effects on physical activity, body size, and fruit consumption in this study, it appears that curriculum-based, health-related programmes in primary schools can have an impact on the behaviours of children, at least over the short-medium term.
The significant improvements observed in the present study are in contrast to the lack of effects reported by the AFLY5 study [ 25 , 26 ], which featured an intervention design very similar to the present study (both studies targeted similar lifestyle behaviours via compulsory in-class lesson plans and homework tasks). The AFLY5 authors offered several explanations as to why AFLY5 may not have had a significant impact, such as the delay in time between intervention development and implementation, and the potential need for more intensive behavioural change and/or upstream societal or environmental approaches. None of these possibilities, however, explain the difference in outcomes between AFLY5 and Healthy Homework. One clear distinction was that Healthy Homework included a minimum of 14 and a maximum of 42 homework tasks over the 8-week period, whereas AFLY5 provided 10 parent-child interaction activities. Furthermore, AFLY5 researchers reported difficulties motivating some teachers, who felt the need to prioritise literacy and numeracy above health-promoting lessons [ 26 ]. Another similar intervention – the Eat Well and Keep Moving Program – was conducted over a two-year period, and integrated materials designed to increase physical activity, improve dietary patterns, and reduce television viewing within the grade 4 and 5 school curriculum (including homework components) [ 11 ]. The evaluation of the intervention revealed significant improvements in dietary patterns and a marginal decrease in television viewing via 24-h recall questionnaires. The present findings add to this body of evidence by demonstrating the potential for positive physical activity outcomes when using objective measurement techniques; however, the effects of embedding health-related lessons and homework within school curricula appear to be variable, and may depend on the specific population and/or context.
There were several limitations present in this study that should be acknowledged. While we were able to collect data about the overall amount of physical activity, we were not able to clarify with any detail the within-day patterns and intensity of activity. Pedometers were primarily chosen for financial reasons; however, the use of omnidirectional accelerometers would have enabled another level of analysis. Related to this point, we were not able to determine the effects on sedentary behaviour, which cannot be effectively isolated via pedometry. As mentioned earlier, a more comprehensive dietary assessment may have revealed some effect on nutrition, although the substantial response burden may have resulted in participant bias. The four items from the CDQ, selected due to their alignment with NZ policy, may not exhibit the same levels of validity and reliability as the full scales. In addition, generalisability of conclusions based on the data in this study is limited by the selection of participants from only two regions of New Zealand; the study design clearly requires replication in larger and more diverse populations. Socioeconomic decile ratings were not evenly matched by intervention and control group; there was one Decile 1 intervention school, whereas the lowest decile rating in the control group was Decile 3. Another limitation was that the research assistants collecting data were not blinded to the school allocation, which may have introduced accidental or deliberate bias during anthropometric assessment. Finally, intervention fidelity, which would have enabled per protocol analysis, was not assessed.
In summary, we have shown that a curriculum-based health programme can result in consistent improvements to physical activity levels in primary school-aged children, with significant but limited effects on body size and fruit consumption. The next step is to see if such programmes are sustainable within the school environment over a long term, and without input from researchers. The effects of such programmes on academic and neurocognitive outcomes development is also of interest and should be explored in future.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available due to a confidentiality agreement with participating schools. Enquiries should be addressed to the principal author.
Abbreviations
Active for life year 5
Body mass index
Children’s dietary questionnaire
Generalised linear mixed model
Randomised controlled trial
Baseline, first follow-up, and second follow-up time points
Waist-to-height ratio
World Health Organization. WHO recommendations on child health. Geneva: World Health Organization; 2017.
Google Scholar
Lipsky LM, Haynie DL, Liu D, Chaurasia A, Gee B, Li K, et al. Trajectories of eating behaviors in a nationally representative cohort of U.S. adolescents during the transition to young adulthood. Int J Behav Nutr Phys Act. 2015;12:138.
Article PubMed PubMed Central Google Scholar
Telama R. Tracking of physical activity from childhood to adulthood: a review. Obes Facts. 2009;2:187–95.
Cooper AR, Goodman A, Page AS, Sherar LB, Esliger DW, van Sluijs EM, et al. Objectively measured physical activity and sedentary time in youth: the International children’s accelerometry database (ICAD). Int J Behav Nutr Phys Act. 2015;12:113.
Vereecken C, Pedersen TP, Ojala K, Krølner R, Dzielska A, Ahluwalia N, et al. Fruit and vegetable consumption trends among adolescents from 2002 to 2010 in 33 countries. Eur J Public Health. 2015;25:16–9.
Article PubMed Google Scholar
Lynch C, Kristjansdottir AG, Te Velde SJ, Lien N, Roos E, Thorsdottir I, et al. Fruit and vegetable consumption in a sample of 11-year-old children in ten European countries–the PRO GREENS cross-sectional survey. Public Health Nutr. 2014;17:2436–44.
Tremblay MS, Barnes JD, Gonzalez SA, Katzmarzyk PT, Onywera VO, Reilly JJ, et al. Global matrix 2.0: report card grades on the physical activity of children and youth comparing 38 countries. J Phys Act Health. 2016;13:S343–S66.
Reilly JJ, Kelly J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. Int J Obes. 2011;35:891–8.
Article CAS Google Scholar
Erwin H, Beighle A, Carson RL, Castelli DM. Comprehensive school-based physical activity promotion: a review. Quest. 2013;65:412–28.
Article Google Scholar
Williams AJ, Henley WE, Williams CA, Hurst AJ, Logan S, Wyatt KM. Systematic review and meta-analysis of the association between childhood overweight and obesity and primary school diet and physical activity policies. Int J Behav Nutr Phys Act. 2013;10:101.
Gortmaker SL, Cheung LW, Peterson KE, Chomitz G, Cradle JH, Dart H, et al. Impact of a school-based interdisciplinary intervention on diet and physical activity among urban primary school children: eat well and keep moving. Arch Pediatr Adolesc Med. 1999;153:975–83.
Article CAS PubMed Google Scholar
Dobbins M, Husson H, DeCorby K, LaRocca RL. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst Rev. 2013;(2):CD007651. https://doi.org/10.1002/14651858.CD007651.pub2 .
Delgado-Noguera M, Tort S, Martínez-Zapata MJ, Bonfill X. Primary school interventions to promote fruit and vegetable consumption: a systematic review and meta-analysis. Prev Med. 2011;53:3–9.
Evans CE, Christian MS, Cleghorn CL, Greenwood DC, Cade JE. Systematic review and meta-analysis of school-based interventions to improve daily fruit and vegetable intake in children aged 5 to 12 y. Am J Clin Nutr. 2012;96:889–901.
Metcalf B, Henley W, Wilkin T. Effectiveness of intervention on physical activity of children: systematic review and meta-analysis of controlled trials with objectively measured outcomes (EarlyBird 54); 2012.
Sims J, Scarborough P, Foster C. The effectiveness of interventions on sustained childhood physical activity: a systematic review and meta-analysis of controlled studies. PLoS One. 2015;10:e0132935.
Wang Y, Cai L, Wu Y, Wilson RF, Weston C, Fawole O, et al. What childhood obesity prevention programmes work? A systematic review and meta-analysis. Obes Rev. 2015;16:547–65.
Article CAS PubMed PubMed Central Google Scholar
Kriemler S, Meyer U, Martin E, van Sluijs EM, Andersen LB, Martin BW. Effect of school-based interventions on physical activity and fitness in children and adolescents: a review of reviews and systematic update. Br J Sports Med. 2011;45:923–30.
Van Sluijs EM, McMinn AM, Griffin SJ. Effectiveness of interventions to promote physical activity in children and adolescents: systematic review of controlled trials. BMJ. 2007;335:703.
Brown HE, Atkin AJ, Panter J, Wong G, Chinapaw MJ, van Sluijs EM. Family-based interventions to increase physical activity in children: a systematic review, meta-analysis and realist synthesis. Obes Rev. 2016;17:345–60.
McMinn AM, Griffin SJ, Jones AP, van Sluijs EM. Family and home influences on children’s after-school and weekend physical activity. Eur J Public Health. 2013;23(5):805–1.
Rockell JE, Parnell WR, Wilson NC, Skidmore PM, Regan A. Nutrients and foods consumed by New Zealand children on schooldays and non-schooldays. Public Health Nutr. 2011;14:203–8.
Regan A, Parnell W, Gray A, Wilson N. New Zealand children's dietary intakes during school hours. Nutr Dietetics. 2008;65:205–10.
Lawlor DA, Jago R, Noble SM, Chittleborough CR, Campbell R, Mytton J, et al. The active for life year 5 (AFLY5) school based cluster randomised controlled trial: study protocol for a randomized controlled trial. Trials. 2011;12:181.
Kipping RR, Howe LD, Jago R, Campbell R, Wells S, Chittleborough CR, et al. Effect of intervention aimed at increasing physical activity, reducing sedentary behaviour, and increasing fruit and vegetable consumption in children: active for life year 5 (AFLY5) school based cluster randomised controlled trial. Bmj. 2014;348:g3256.
Anderson EL, Howe LD, Kipping RR, Campbell R, Jago R, Noble SM, et al. Long-term effects of the active for life year 5 (AFLY5) school-based cluster-randomised controlled trial. BMJ Open. 2016;6:e010957.
Duncan S, McPhee JC, Schluter PJ, Zinn C, Smith R, Schofield G. Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: the healthy homework pilot study. Int J Behav Nutr Phys Act. 2011;8:127.
Abraham C, Michie S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008;27:379–87.
Ministry of Education. The New Zealand curriculum. Wellington: Ministry of Education; 2007.
Duncan S, Schofield G, Duncan EK, Hinckson EA. Effects of age, walking speed, and body composition on pedometer accuracy in children. Res Q Exerc Sport. 2007;78:420–8.
Magarey A, Golley R, Spurrier N, Goodwin E, Ong F. Reliability and validity of the Children's dietary questionnaire; a new tool to measure children's dietary patterns. Int J Ped Obes. 2009;4:257–65.
Sundborn G, Utter J, Teevale T, Metcalf P, Jackson R. Carbonated beverages consumption among New Zealand youth and associations with BMI and waist circumference. Pac Health Dialog. 2014;20(1):81–6.
CAS PubMed Google Scholar
Janssen I, Leblanc AG. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int J Behav Nutr Phys Act. 2010;7:40.
Poitras VJ, Gray CE, Borghese MM, Carson V, Chaput JP, Janssen I, et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl Physiol Nutr Metab. 2016;41:S197–239.
World Health Organization. Interventions on diet and physical activity: what works. Geneva: World Health Organization; 2009.
Viitasalo A, Eloranta AM, Lintu N, Vaisto J, Venalainen T, Kiiskinen S, et al. The effects of a 2-year individualized and family-based lifestyle intervention on physical activity, sedentary behavior and diet in children. Prev Med. 2016;87:81–8.
Taylor RW, Cox A, Knight L, Brown DA, Meredith-Jones K, Haszard JJ, et al. A tailored family-based obesity intervention: a randomized trial. Pediatrics. 2015;136:281–9.
Download references
Acknowledgements
The authors would like to thank all participating schools, children, and parents for contributing their time and effort to this study.
Funding for the Healthy Homework study was provided by a Health Research Council of New Zealand Project Grant (10–207).
Author information
Authors and affiliations.
School of Sport and Recreation, Auckland University of Technology, Private Bag 92006, Auckland, New Zealand
Scott Duncan, Tom Stewart, Julia McPhee, Robert Borotkanics, Kate Prendergast, Caryn Zinn & Grant Schofield
Edgar Diabetes and Obesity Research Centre, University of Otago, PO Box 56, Dunedin, New Zealand
Kim Meredith-Jones & Rachael Taylor
School of Education, Federation University Australia, PO Box 663, Ballarat, VIC 3353, Victoria, Australia
Claire McLachlan
You can also search for this author in PubMed Google Scholar
Contributions
SD and GS conceptualised the study, and SD was the principal investigator for the Health Research Council Project Grant. SD, CZ, RT designed the evaluation protocol, and SD, JM, KP, CZ, and CM contributed to the development of intervention resources. JM, KP, and KM recruited all participants and collected the data. KP and KM collated and processed the data, and RB and SD analysed the data. SD and TS drafted the manuscript. All authors provided critical feedback throughout the writing process. All authors read and approved the final manuscript.
Corresponding author
Correspondence to Scott Duncan .
Ethics declarations
Ethics approval and consent to participate.
Written informed parental consent and personal assent was obtained from each participant for the collection and use of the data in future publication. Ethical approval for the study was obtained from the Auckland University of Technology (10/159) and University of Otago (11/084) Ethics Committees.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:.
CONSORT 2010 checklist of information to include when reporting a randomised trial. (DOC 218 kb)
Additional file 2:
Teachers Manual. (PDF 11980 kb)
Additional file 3:
Students Manual. (PDF 10554 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License ( http://creativecommons.org/licenses/by/4.0/ ), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated.
Reprints and permissions
About this article
Cite this article.
Duncan, S., Stewart, T., McPhee, J. et al. Efficacy of a compulsory homework programme for increasing physical activity and improving nutrition in children: a cluster randomised controlled trial. Int J Behav Nutr Phys Act 16 , 80 (2019). https://doi.org/10.1186/s12966-019-0840-3
Download citation
Received : 08 May 2018
Accepted : 16 August 2019
Published : 05 September 2019
DOI : https://doi.org/10.1186/s12966-019-0840-3
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Child health
- Intervention
- Dietary assessment
- Child obesity
International Journal of Behavioral Nutrition and Physical Activity
ISSN: 1479-5868
- Submission enquiries: Access here and click Contact Us
- General enquiries: [email protected]
- Help & FAQ
Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: the healthy homework pilot study
Research output : Contribution to journal › Article › Research › peer-review
| Original language | English |
|---|---|
| Pages (from-to) | 127 - 136 |
| Number of pages | 10 |
| Journal | |
| Volume | 8 |
| DOIs | |
| Publication status | Published - 2011 |
| Externally published | Yes |
Access to Document
- 10.1186/1479-5868-8-127
Other files and links
- RM sElocation
T1 - Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: the healthy homework pilot study
AU - Duncan, Scott
AU - McPhee, Julia C
AU - Schluter, Philip
AU - Zinn, Caryn
AU - Smith, Richard John McKenzie
AU - Schofield, Grant
UR - http://www.ijbnpa.org/content/8/1/127
U2 - 10.1186/1479-5868-8-127
DO - 10.1186/1479-5868-8-127
M3 - Article
SN - 1479-5868
JO - International Journal of Behavioral Nutrition and Physical Activity
JF - International Journal of Behavioral Nutrition and Physical Activity
- Advanced search
- Peer review
- Record : found
- Abstract : found
- Article : found
Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: the healthy homework pilot study
Read this article at
- Download PDF
- Review article
- Invite someone to review
Most physical activity and nutrition interventions in children focus on the school setting; however, evidence suggests that children are less active and have greater access to unhealthy food at home. The aim of this pilot study was to examine the efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children.
The six-week 'Healthy Homework' programme and complementary teaching resource was developed under the guidance of an intersectoral steering group. Eight senior classes (year levels 5-6) from two diverse Auckland primary schools were randomly assigned into intervention and control groups. A total of 97 children (57 intervention, 40 control) aged 9-11 years participated in the evaluation of the intervention. Daily step counts were monitored immediately before and after the intervention using sealed multiday memory pedometers. Screen time, sports participation, active transport to and from school, and the consumption of fruits, vegetables, unhealthy foods and drinks were recorded concurrently in a 4-day food and activity diary.
Healthy Homework resulted in a significant intervention effect of 2,830 steps.day -1 (95% CI: 560, 5,300, P = 0.013). This effect was consistent between sexes, schools, and day types (weekdays and weekend days). In addition, significant intervention effects were observed for vegetable consumption (0.83 servings.day -1 , 95% CI: 0.24, 1.43, P = 0.007) and unhealthy food consumption (-0.56 servings.day -1 , 95% CI: -1.05, -0.07, P = 0.027) on weekends but not weekdays, with no interactions with sex or school. Effects for all other variables were not statistically significant regardless of day type.
Conclusions
Compulsory health-related homework appears to be an effective approach for increasing physical activity and improving vegetable and unhealthy food consumption in children. Further research in a larger study is required to confirm these initial results.
Related collections
Karger: Nutrition and Dietetics
Most cited references 40
- Article : not found
Physical activity from childhood to adulthood: a 21-year tracking study.
Family correlates of fruit and vegetable consumption in children and adolescents: a systematic review.

Effect of school based physical activity programme (KISS) on fitness and adiposity in primary schoolchildren: cluster randomised controlled trial
Author and article information , affiliations.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License ( http://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Comment on this article
Similar content 464 .
- Reflecting on homework in psychotherapy: what can we conclude from research and experience? Authors: Nikolaos Kazantzis , Georgios K Lampropoulos
- Music Therapy for Depression Enhanced With Listening Homework and Slow Paced Breathing: A Randomised Controlled Trial Authors: Jaakko Erkkilä , Olivier Brabant , Martin Hartmann …
- Relationship Between Students’ Prior Academic Achievement and Homework Behavioral Engagement: The Mediating/Moderating Role of Learning Motivation Authors: Susana Rodriguez , José C. Núñez , Antonio Valle …
Cited by 23
- Understanding differences between summer vs. school obesogenic behaviors of children: the structured days hypothesis Authors: Keith Brazendale , Michael Beets , R Weaver …
- Family‐based interventions to increase physical activity in children: a systematic review, meta‐analysis and realist synthesis Authors: H. E. Brown , A. Atkin , J. Panter …
- Environmental interventions to reduce the consumption of sugar‐sweetened beverages and their effects on health Authors: Peter von Philipsborn , Jan Stratil , Jacob Burns …
Most referenced authors 589
Efficacy of a Compulsory Homework Programme for Increasing Physical Activity and Healthy Eating in Children: The Healthy Homework Pilot Study
Degree name, journal title, journal issn, volume title.
Background: Most physical activity and nutrition interventions in children focus on the school setting; however, evidence suggests that children are less active and have greater access to unhealthy food at home. The aim of this pilot study was to examine the efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children.
Methods: The six-week ‘Healthy Homework’ programme and complementary teaching resource was developed under the guidance of an intersectoral steering group. Eight senior classes (year levels 5-6) from two diverse Auckland primary schools were randomly assigned into intervention and control groups. A total of 97 children (57 intervention, 40 control) aged 9-11 years participated in the evaluation of the intervention. Daily step counts were monitored immediately before and after the intervention using sealed multiday memory pedometers. Screen time, sports participation, active transport to and from school, and the consumption of fruits, vegetables, unhealthy foods and drinks were recorded concurrently in a 4-day food and activity diary.
Results: Healthy Homework resulted in a significant intervention effect of 2,830 steps.day-1 (95% CI: 560, 5,300, P = 0.013). This effect was consistent between sexes, schools, and day types (weekdays and weekend days). In addition, significant intervention effects were observed for vegetable consumption (0.83 servings.day-1, 95% CI: 0.24, 1.43, P = 0.007) and unhealthy food consumption (-0.56 servings.day-1, 95% CI: -1.05, -0.07, P = 0.027) on weekends but not weekdays, with no interactions with sex or school. Effects for all other variables were not statistically significant regardless of day type.
Conclusions: Compulsory health-related homework appears to be an effective approach for increasing physical activity and improving vegetable and unhealthy food consumption in children. Further research in a larger study is required to confirm these initial results.
Description
Publisher's version, rights statement, permanent link, collections.
Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: the healthy homework pilot study.
Most physical activity and nutrition interventions in children focus on the school setting; however, evidence suggests that children are less active and have greater access to unhealthy food at home. The aim of this pilot study was to examine the efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children. The six-week Healthy Homework programme and complementary teaching resource was developed under the guidance of an intersectoral steering group. Eight senior classes (year levels 5-6) from two diverse Auckland primary schools were randomly assigned into intervention and control groups. A total of 97 children (57 intervention, 40 control) aged 9-11 years participated in the evaluation of the intervention. Daily step counts were monitored immediately before and after the intervention using sealed multiday memory pedometers. Screen time, sports participation, active transport to and from school, and the consumption of fruits, vegetables, unhealthy foods and drinks were recorded concurrently in a 4-day food and activity diary. Healthy Homework resulted in a significant intervention effect of 2,830 steps.day-1 (95% CI: 560, 5,300, P = 0.013). This effect was consistent between sexes, schools, and day types (weekdays and weekend days). In addition, significant intervention effects were observed for vegetable consumption (0.83 servings.day-1, 95% CI: 0.24, 1.43, P = 0.007) and unhealthy food consumption (-0.56 servings.day-1, 95% CI: -1.05, -0.07, P = 0.027) on weekends but not weekdays, with no interactions with sex or school. Effects for all other variables were not statistically significant regardless of day type. Compulsory health-related homework appears to be an effective approach for increasing physical activity and improving vegetable and unhealthy food consumption in children. Further research in a larger study is required to confirm these initial results.
- DOI: 10.1186/1479-5868-8-127
- Corpus ID: 17153748
Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: the healthy homework pilot study
- S. Duncan , J. McPhee , +3 authors G. Schofield
- Published in International Journal of… 15 November 2011
- Education, Medicine
55 Citations
Efficacy of a compulsory homework programme for increasing physical activity and improving nutrition in children: a cluster randomised controlled trial, evaluation of school-based interventions including homework to promote healthy lifestyles: a systematic review with meta-analysis, promoting healthy weight in primary school children through physical activity and nutrition education: a pragmatic evaluation of the change randomised intervention study, active homework: an under-researched element of the active schools concept.
- Highly Influenced
- 10 Excerpts
Teaching approaches and strategies that promote healthy eating in primary school children: a systematic review and meta-analysis
Exploring the feasibility of a cluster pilot randomised control trial to improve children’s 24-hour movement behaviours and dietary intake: happy homework, the effects of the change intervention on children's physical activity and health, application of an online combination exercise intervention to improve physical and mental health in obese children: a single arm longitudinal study, effects of a recreational physical activity and healthy habits orientation program, using an illustrated diary, on the cardiovascular risk profile of overweight and obese schoolchildren: a pilot study in a public school in brasilia, federal district, brazil, fitness promotion in a jump rope-based homework intervention for middle school students: a randomized controlled trial, 60 references, evaluation of a pilot school programme aimed at the prevention of obesity in children., evaluation of the nutrition education at primary school (neaps) programme, promoting physical activity participation among children and adolescents., effect of school based physical activity programme (kiss) on fitness and adiposity in primary schoolchildren: cluster randomised controlled trial, evaluation of a community-based intervention to promote physical activity in youth: lessons from active winners, attitudes towards exercise and physical activity behaviours in greek schoolchildren after a year long health education intervention, school physical education: effect of the child and adolescent trial for cardiovascular health., outcomes of a field trial to improve children's dietary patterns and physical activity. the child and adolescent trial for cardiovascular health. catch collaborative group., the effects of a family fitness program on the physical activity and nutrition behaviors of third-grade children, a 4-year, cluster-randomized, controlled childhood obesity prevention study: stopp, related papers.
Showing 1 through 3 of 0 Related Papers
Europe PMC requires Javascript to function effectively.
Either your web browser doesn't support Javascript or it is currently turned off. In the latter case, please turn on Javascript support in your web browser and reload this page.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Diabetes Metab Syndr Obes
Effects of a recreational physical activity and healthy habits orientation program, using an illustrated diary, on the cardiovascular risk profile of overweight and obese schoolchildren: a pilot study in a public school in Brasilia, Federal District, Brazil
Angeliete garcez militão.
1 Department of Physical Education, Federal University of Rondonia, Brazil
2 Post-Graduate Program in Physical Education, Catholic University of Brasilia, Brazil
Margô Gomes de Oliveira Karnikowski
3 University of Brasilia, Brazil
Fernanda Rodrigues da Silva
4 Laboratory of Physical Evaluation and Training, Catholic University of Brasilia, Brazil
Elba Sancho Garcez Militão
Raiane maiara dos santos pereira.
5 Laboratory of Physical Education and Health Studies, Catholic University of Brasilia, Brazil
Carmen Silvia Grubert Campbell
Introduction.
Educative strategies need to be adopted to encourage the consumption of healthy foods and to promote physical activity in childhood and adolescence. The effects of recreational physical activity and a health-habit orientation program using an illustrated diary on the cardiovascular risk profile of overweight and obese children was investigated.
The weight and height of 314 schoolchildren aged between 9 and 11 years old, in a public school in Brasilia, Federal District, Brazil, were recorded. According to the body mass index (BMI) classification proposed by the World Health Organization, 84 were overweight or obese for their age and sex. Of these children, 34 (40%) participated in the study. Students were divided into two groups matched for sex, age, BMI, percent body fat (%BF): the intervention group (IG, n = 17) and the control group (CG, n = 17). The IG underwent a program of 10 weeks of exercise with recreational activities and health-habit orientation using an illustrated diary of habits, while no such interventions were used with the CG during the study period. Before and after the intervention, the children’s weight, height, BMI, %BF, waist circumference (WC), maximum oxygen intake (VO 2max ), total cholesterol (TC), high density lipoprotein (HDL), low density lipoprotein (LDL), triglycerides, glucose, eating habits, and physical activity level (PAL) were assessed. In analyzing the data, we used descriptive statistics and paired and unpaired t -tests, using a significance level of 0.05. For assessment of dietary habits, a questionnaire, contingency tables, and the chi-squared test were used, with <0.05 set as the significance level.
After 10 weeks of intervention, the IG showed a reduction in BMI (pre: 22.2 ± 2.1 kg/m 2 versus [vs] post: 21.6 ± 2.1 kg/m 2 , P < 0.01); WC (pre: 70.1 ± 6.1 cm vs post: 69.1 ± 5.8 cm, P < 0.01); %BF (pre: 29.2% ± 4.6% vs post: 28.0% ± 4.8%, P < 0.01); systolic blood pressure ( P < 0.01); VO 2max ( P = 0.014); TC ( P < 0.01); LDL ( P < 0.01); triglycerides ( P < 0.01); and intake of candy ( P < 0.01) and soda drinks ( P < 0.01), while an increase in the consumption of fruit ( P < 0.01) and PAL ( P < 0.01) were observed. The CG did not show any change in the health parameters assessed.
The program was effective in reducing risk factors for cardiovascular disease and the use of an illustrative diary may have been the key to this result, since students were motivated to change their poor eating habits and to increase their physical activity level.
Worldwide, obesity is considered to be the epidemic of twenty-first century, and is related to the development of insulin resistance and diabetes, as well as to the predisposition to increases in serum levels of cholesterol and systolic blood pressure (SBP) and diastolic blood pressure, which are risk factors for cardiovascular disease (CVD). 1
An analysis of Korean teenagers found that levels of total cholesterol (TC) increased significantly with increasing body mass index (BMI). 2 Furthermore, Reinehr et al 3 in Germany and May et al 4 in the USA found that obese children, when compared with those of normal weight, had higher concentrations of low density lipoprotein (LDL) and lower concentrations of high density lipoprotein (HDL). In Brazil, a positive correlation of waist circumference (WC) and BMI, with blood pressure was observed in schoolchildren in Taguatinga, Federal District. 5
Data from the VIGITEL Brasil 2011: Vigilância de Fatores de Risco e Proteção para Doenças Crônicas por Inquérito Telefônico [Surveillance of risk and protective factors for chronic diseases by telephone survey] 6 revealed that the proportion of overweight persons in Brazil had increased, from 42.7% in 2006 to 48.5% in 2011, while the percentage of obese persons increased from 11.4% to 15.8%. In the Federal District, in the same period, the percentage of the population that was overweight or obese increased from 39.8% to 49.2% and from 10% to 15%, respectively. 6 These data show that strategies should be implemented to curb and reduce weight gain in this population.
A way to prevent obesity in adulthood is to treat childhood overweight and obesity. Once excess weight is present in childhood and adolescence it tends to persist in older ages. 7 Further, atherosclerosis and arterial hypertension, pathological processes that start in childhood; life phase; eating habits; physical activity level (PAL); and environmental factors are determining the increase in obesity prevalence. 8
Educative strategies should be adopted to encourage the consumption of healthy foods and to promote physical activity in childhood and adolescence. The school environment is a good place to promote a healthy lifestyle, because this is a place of intense social interaction and is appropriate for educative activities. 9 In particular, school physical education classes represent particularly suitable venues for dissemination of information, discussion, and reflection on healthy habits.
In this regard, our group has created a learning tool for use in physical education classes called an “illustrative diary” that aims to promote knowledge that will motivate students to adopt a healthy diet and to reduce sedentary behavior (watching television, playing video games, and computer use). 10 The instrument consists of a paper pad with blank squares representing each day of the week, which the students fill with figures representing their activities during the day concerning nutrition, physical activities, and sedentary behaviors. Thus, the aim of the study reported here was to evaluate the effects of a program of recreational physical activities, associated with the use of the illustrative diary, on the cardiovascular risk profile of overweight and obese schoolchildren.
Study design and sample selection
This was a pilot study with experimental delimitation conducted in Classe 46 School in Ceilândia, Federal District, Brazil. Students born between 2001 and 2003 enrolled in that school were invited to have their height and weight assessed to identify those overweight and obese for inclusion in the study. A total of 314 students attended the evaluations, of whom 84 were classified as overweight (≥85th and <95th percentile) and obese (>95th percentile) for their age and sex according to the World Health Organization’s BMI classification. 11
From the 84 children classified as overweight and obese, 34 (40%) consented to participate in the study and they were organized into two homogeneous and internally heterogeneous groups, between them, with the same number of participants, and number of males and females in each. The intervention group (IG), which comprised eight male and nine female participants, submitted to a program of recreational physical activity and orientation to healthy lifestyle using the illustrative diary, while the control group (CG), again comprising eight male and nine female participants, continued with their daily normal activities.
The parents of the schoolchildren signed informed consent in accordance with Brazilian Resolution 196/96. The research was approved by the Ethics Committee of the Catholic University of Brasilia (protocol CAAE07297412.4.0000.0029).
Evaluations
Pubertal development, weight, height, WC, cardiorespiratory fitness, blood pressure, and biochemical parameters (fasting glucose [FG], TC, LDL, HDL, and triglyceride [TG] levels) were assessed and skinfold measurements taken. In addition, the level of physical activity and eating habits were measured before and after intervention.
To measure body weight, the adolescents, wearing school uniform and barefoot, were positioned standing on a Wiso scale, model W721 (Wiso, Sportive Technology, Florianopolis, Brazil) with digital display and 100 g of precision while being asked to keep still and stand erect in the middle of the scale, with their arms along their body. For evaluation of stature, a Sanny compact stadiometer, model ES:2040 (Sanny – American Medical do Brasil, Ltda, São Bernardo do Campo, Brazil) fixed on a wall without a gap, accurate to 1 mm, was used with the teenagers barefoot and leaning against the wall, heels together, hands relaxed along the body, and head adjusted in the Frankfurt plane. BMI was determined using the formula: weight in kg/m 2 ). The cutoff points proposed by the World Health Organization classification were used. 11
For evaluation of WC, a Sanny fiberglass tape with a precision of 1 mm was used. The measurement was taken from the lower circumference, located midpoint between the last rib and iliac crest. Tricipital (TR) and subscapular (SB) skinfolds were measured with a Lange Skinfold Caliper skinfold compass (Santa Cruz, CA, USA) with resolution of 5 mm. For measurement of the triciptal, the compass was placed on the back of the right arm of the adolescent, at the midpoint between the lateral projection of the acromion process and inferior margin of the olecranon. The subscapular was measured 1 cm below the inferior angle of the scapula. The %BF was estimated from the results of the sum of the TR and SB using Boileau et al’s equation. 12
Cardiorespiratory fitness, expressed as maximum oxygen uptake (VO 2max [mL·kg −1 ·min −1 ]), was obtained from a 20 m shuttle run test according to the procedure and equations outlined by Léger and Lambert. 13 This test consists of a running in a limited space of 20 m, where the students were submitted to a run in the rhythm of a sound signal. In each signal, they should reach one end marked. The signal is based on the speed (km/h), which starts with 8.5 km/h, increasing by 0.5 km/h each time, until the evaluated student can’t reach one of the extremities after two consecutive signals. The test was conducted in the same school to which they belonged. The track was marked in a span of 20 m and two students took the test at a time, each one supervised by a physical education professional. Leger et al’s formula was used to estimate the VO 2max , using the age and average speed (km/h) data. To identify the extent of pubertal development, the self-assessment method proposed by Tanner 14 was employed. This method allows the student to identify their own maturity stage by observing the development of pubic hair. Individually, each student reported to a researcher of the same sex as themselves, which image presented to them they most identified with. From their responses, each was classified as either prepubescent (stage 1), pubescent (stages 2–4), or postpubescent (stage 5).
Blood pressure was measured three times at intervals of 2 minutes. Before the first measurement, the student sat for 5 minutes. An automatic digital monitor (Omron Hem 705 CP, Omron, Tokyo, Japan) was used with clamps of suitable size with a width of approximately 40% of the arm circumference. The measurements were performed on the right arm and the mean of the three assessments was considered.
For biochemical evaluations, a technician from the Clinical Laboratory of the University of Brasilia went to Classe 46 School between 7.30 and 8.30 am to collect blood by venipuncture. The children were required to fast for 12 hours prior to having their blood collected. Blood (10 mL) was collected in a tube with a gel separator and under vacuum without anticoagulant and transported in a Styrofoam box with dry ice to the analytical laboratory of the University Hospital of Brasilia. For determination of FG, TC, HDL, LDL, and TG, the following methods were used: serum/hexokinase automated and serum/esterase-oxidase, oxidase-peroxidase and Friedewald formula. Dosage of FG was performed with an automated method (colorimetric enzymatic glucose-hexoxidase) in an ARCHITECT C8000 Analyzer (Abbott, Illinois, USA), using 5 mL of serum after being centrifuged at 3,000 rpm for 5 minutes. TC, TG and HDL were analyzed using the enzymatic colorimetric method utilising esterase-oxidase and oxidase-peroxidase, using 5 mL of serum after being centrifuged at 3,000 rpm for 5 minutes. The LDL fraction was obtained using the formula proposed by Friedewald et al. 15 The measurements were performed with the automated method on device ARCHITECT C8000 Analyzer (Abbott, Illinois, USA).
The metabolic equivalent (MET) is defined as the oxygen uptake equivalent to a sitting quietly position (3.5 mL·kg −1 ·min −1 ). The PAL was obtained in MET/week by using the Level of Physical Activity and Sedentary Behavior in Teenager Students questionnaire, created and validated by our group. 16 In this questionnaire students were classified into the following categories: sedentary (PAL less than 600 MET/week), irregularly active (PAL greater than 600 and less than 1,500 MET/week), active (PAL greater than 1,500 and less than 3,000 MET/week) and very active (PAL greater than 3,000 MET/week). Dietary habits were assessed by the questionnaire Risk Behaviors of Adolescents Catarinenses – COMPAC 17 in which students were asked about the weekly frequency of consumption of fruit juice, vegetables, fruits, sodas, chips, pasta, sweets, meat, rice and beans.
Intervention program
Students in the IG performed recreational physical activities and received guidance on healthy habits, in a different timetable than they normally study, during 10 weeks, with 20 sessions of 60 minutes each. Each session comprised 5 minutes of stretching, 40 minutes of basic motor recreational activities (running, jumping, and throwing), and 15 minutes recovery time, which included guidance on healthy habits and use of the illustrative diary.
Recreational activities were planned and directed by a physical education teacher to ensure that the children would be active throughout the period doing activities at a moderate to vigorous intensity (65% to 85% of maximum heart rate obtained in the described 20 m shuttle run test). During the activities, students’ heart rate was monitored using a monitor Polar F1TM (Polar Electro Oy, FIN-90440 Kempele, Finland) to ensure the group was exercising within the recommended range.
In terms of the guidance on healthy habits, on the first day of the intervention, each student received a journal made of A4 paper containing pictures representing each weekday, and pages displaying various images of food (fruit, vegetables, candy, fried foods, soft drinks, fruit juice, etc), sedentary activities (watching TV, using a computer, playing video games), and active behavior (jumping rope, jogging, playing soccer, cycling, etc). Colorful pictures were used to represent healthy habits, while black and white pictures were used to represent unhealthy habits. Children were asked to paste pictures into their diary to represent the activities done and foods eaten and to write down the amount of times that they consumed each particular food and the time spent doing each activity. The parents of the students received a note explaining the diary completion activity and recommending that children should take it to school each day that a study recreational activity session was scheduled.
At the end of each recreational activity session, students showed the diary pages that they had filled in daily at home to the teacher and proper habits and inadequate health care were discussed, with the intention of motivating students to improve their lifestyle and making their diaries more colorful as a result.
Statistical analysis
Means and standard deviations were initially used for variables with parametric distribution. The Shapiro–Wilk test was performed to evaluate the variables’ adherence to a normal curve, where all showed normality ( P < 0.05). Paired and non-paired t -tests were used to compare data between variables. For data analysis of the questionnaire assessment of dietary habits, we used contingency tables and chi-square tests. All statistical analyses were performed using SPSS Statistics (version 17.0, IBM Corporation, Armonk, NY, USA), using a significance level of P < 0.05.
The sample included 34 children (nine girls and eight boys in each group). The mean age of children in the IG and CG was 9.9 years and 10.1 years, respectively. Students were prepubescent and pubescent. All the girls were pubertal and 25% of the boys were prepubertal. The students were divided evenly between both groups to avoid interference of biological age in the research results.
There were no significant differences between the IG and CG in terms of anthropometric parameters, biochemical parameters, blood pressure, or VO 2max , both before and after the intervention. However, when comparing results within the same group, it was observed that unlike the CG, the IG showed significant differences in almost all variables, showing positive reductions in risk factors for CVD ( Table 1 ).
Characteristics of intervention group and control group pre- and post-intervention
| Variable | Intervention (n = 17) | -value | Control (n = 17) | -value | ||
|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | |||
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |||
| Age (years) | 9.94 ± 0.83 | 10.00 ± 0.93 | – | 10.12 ± 0.86 | 10.12 ± 0.86 | – |
| Weight (kg) | 46.75 ± 7.49 | 46.25 ± 7.46 | 0.012 | 48.05 ± 7.15 | 48.95 ± 8.43 | 0.28 |
| Height (cm) | 1.45 ± 0.9 | 1.46 ± 0.9 | 0.000 | 1.48 ± 0.8 | 1.49 ± 0.08 | 0.00 |
| BMI (kg/m ) | 22.21 ± 2.15 | 21.6 ± 2.08 | 0.000 | 22.17 ± 1.08 | 21.89 ± 2.24 | 0.18 |
| WC (cm) | 70.16 ± 6.15 | 69.15 ± 5.84 | 0.001 | 71.4 ± 4.93 | 71.14 ± 5.99 | 0.60 |
| %BF | 29.25 ± 4.57 | 28.05 ± 4.77 | 0.003 | 29.69 ± 4.88 | 29.53 ± 0.61 | 0.61 |
| SBP (mmHg) | 106.02 ± 9.57 | 101.72 ± 10.37 | 0.000 | 108.25 ± 8.8 | 104.74 ± 8.65 | 0.22 |
| DBP (mmHg) | 65.12 ± 8.25 | 62.92 ± 9.06 | 0.308 | 70.58 ± 11.8 | 65.5 ± 5.22 | 0.10 |
| VO (mL·kg ·min ) | 43.35 ± 2.01 | 44.3 ± 2.37 | 0.014 | 42.95 ± 3.24 | 43.5 ± 3.51 | 0.10 |
| FG (mg/dL) | 84.29 ± 4.01 | 82.12 ± 5.38 | 0.153 | 83.71 ± 8.47 | 84.71 ± 8.44 | 0.45 |
| TC (mg/dL) | 168.82 ± 29.03 | 154.0 ± 26.72 | 0.000 | 158.94 ± 32.59 | 153.88 ± 29.59 | 0.15 |
| HDL (mg/dL) | 43.29 ± 8.08 | 41.88 ± 7.36 | 0.152 | 40.71 ± 7.69 | 38.29 ± 9.02 | 0.09 |
| LDL (mg/dL) | 107.53 ± 28.38 | 99.76 ± 26.8 | 0.000 | 101.41 ± 28.54 | 95.88 ± 23.92 | 0.17 |
| TG (mg/dL) | 90.24 ± 28.02 | 70.76 ± 24.85 | 0.002 | 83.82 ± 33.46 | 99.0 ± 58.46 | 0.18 |
Abbreviations: %BF, percent body fat; BMI, body mass index; DBP, diastolic blood pressure; FG, fasting glucose; HDL, high density lipoprotein; LDL, low density lipoprotein; SBP, systolic blood pressure; SD, standard deviation; TC, total cholesterol; TG, triglycerides; VO 2max , maximum oxygen intake; WC, waist circumference.
The healthy lifestyle guidance offered through the illustrative diary motivated the students to include recreational physical activities in their daily routine. Before the intervention, children were classified as “irregularly active,” with no significant differences between groups at pre-test ( P = 0.73). However, after the intervention, the groups differed significantly ( P < 0.01), with most students in the IG becoming active while those in the CG remained irregularly active ( Table 2 ).
Comparatives test of total physical activity level intra-and inter-group
| Group | METs | SD | n | Paired -test | IG/CG, independent -test | |
|---|---|---|---|---|---|---|
| -value | -value (pre) | -value (post) | ||||
| IG | ||||||
| Pre | 669.79 | 366.71 | 17 | <0.01 | 0.73 | <0.01 |
| Post | 1,601.38 | 529.67 | 17 | |||
| CG | ||||||
| Pre | 713.12 | 357.66 | 17 | 0.23 | ||
| Post | 847.43 | 340.27 | 17 | |||
Notes: Physical activity level classification: sedentary <600 MET/week, irregularly active >600 and <1,500 MET/week, active >1,500 and <3,000 MET/week, and very active >3,000 MET/week.
Abbreviations: CG, control group; IG, intervention group; MET, work metabolic equivalent; SD, standard deviation.
Analysis of the questionnaire assessing the eating habits of students in the IG and CG revealed no significant differences between them before the intervention. However, after the intervention, there were significant differences in intake of fruit juice, fruit, soft drinks, and candy ( Table 3 ).
Comparative analysis of the eating habits of schoolchildren in the intervention group (IG) and control group (CG), pre- and post-intervention
| Weekly intake | Pre | -value | Post | -value |
|---|---|---|---|---|
| Fruit juice | IG | 0.203 | IG | 0.006 |
| CG | CG | |||
| Fruit | IG | 0.488 | IG | 0.004 |
| CG | CG | |||
| Legumes | IG | 0.203 | IG | 0.139 |
| GC | GC | |||
| Soda drinks | IG | 0.729 | IG | 0.002 |
| CG | CG | |||
| Fries | IG | 0.331 | IG | 0.122 |
| CG | CG | |||
| Pasta | IG | 0.465 | IG | 0.319 |
| CG | CG | |||
| Candy | IG | 0.396 | IG | 0.070 |
| CG | CG | |||
| Rice and beans | IG | 0.382 | IG | 0.587 |
| CG | CG | |||
| Meat | IG | 0.048 | IG | 0.151 |
| CG | CG |
In analysis of the questionnaires assessing eating habits, we observed a significant increase in weekly intake of fruit juice and fresh fruit and this was associated with an equally significant decrease in intake of sodas, fries, and pasta. In addition, there was a decrease in the frequency of the weekly consumption of meat ( Table 4 ).
Eating habits of schoolchildren in the intervention group (IG), pre- and post-intervention (%)
| Weekly intake | Situation | 0 times | 1–3 times | 4–6 times | Every day | Twice every day | -value |
|---|---|---|---|---|---|---|---|
| Fruit juice | Pre | 58.8 | 41.2 | 0.0 | 0.0 | 0.0 | <0.01 |
| Post | 17.6 | 11.8 | 70.6 | 0.0 | 0.0 | ||
| Fruit | Pre | 23.5 | 70.6 | 5.9 | 0.0 | 0.0 | <0.01 |
| Post | 0.0 | 11.8 | 29.4 | 58.8 | 0.0 | ||
| Legumes | Pre | 35.3 | 29.4 | 11.8 | 23.5 | 0.0 | 0.14 |
| Post | 11.8 | 17.6 | 41.2 | 29.4 | 0.0 | ||
| Soda drinks | Pre | 5.9 | 29.4 | 17.6 | 47.1 | 0.0 | <0.01 |
| Post | 58.8 | 29.4 | 11.8 | 0.0 | 0.0 | ||
| Fries | Pre | 17.6 | 35.3 | 35.3 | 11.8 | 0.0 | <0.05 |
| Post | 64.7 | 11.8 | 17.6 | 5.9 | 0.0 | ||
| Pasta | Pre | 29.4 | 58.8 | 5.9 | 5.9 | 0.0 | <0.05 |
| Post | 70.6 | 17.6 | 11.8 | 0.0 | 0.0 | ||
| Candy | Pre | 5.9 | 17.6 | 17.6 | 47.1 | 0.0 | <0.01 |
| Post | 5.9 | 47.1 | 47.1 | 0.0 | 0.0 | ||
| Rice and beans | Pre | 0.0 | 0.0 | 5.9 | 23.5 | 70.6 | 0.15 |
| Post | 0.0 | 0.0 | 0.0 | 52.9 | 47.1 | ||
| Meat | Pre | 0.0 | 41.2 | 23.5 | 35.3 | 0.0 | 0.01 |
| Post | 0.0 | 5.9 | 76.5 | 17.6 | 0.0 |
In this research, a program of recreational physical activity and orientation to healthy habits using an illustrative diary showed positive effects on the cardiovascular risk profile of overweight and obese schoolchildren aged 9 to 11 years old, reducing their BMI, WC, %BF, TC, LDL, TG, and SBP, and increasing their VO 2max . These results, despite the relatively short duration of the intervention, probably occurred because, aside from the 20 hours of recreational activities in school, the orientation toward healthy habits through the use of the illustrative diary encouraged them to practice physical activity every day and to adopt a healthy diet.
No child discontinued the program, which may be due to the fact that the activities were carried out at school as well as the active participation of students in discussions about healthy lifestyles generated through the illustrative diary. Another reason for this may have been that the physical activities were all recreational. Students in the CG were encouraged to conduct the pre- and post-intervention, with the idea of their participating in the program the following year. At the beginning of the program, students were not engaged in regular physical activity programs and had inadequate diets that included the consumption of fried foods, candy, pasta, and soda drinks, and a low intake of vegetables, fruit and fruit juice. The orientation toward healthy habits through an illustrative diary motivated students in the IG to perform physical activities every day, increasing their activity level from irregular to active, as well as encouraged students to consume more fruit juice and fresh fruit and less soda drinks, fried foods, pasta and candy.
These findings corroborate Duncan et al’s results. 18 In their study, they also found changes in the PALs and eating habits of schoolchildren in New Zealand after 6 weeks of a program called “Healthy Homework.” This program was designed for the physical education curriculum, with the goal of increasing physical activity and healthy eating through school homework that required children to receive weekly booklets with guidelines on various healthy activities that they were to realize.
Poor dietary and low PAL are important contributing factors to obesity and risk factors for CVD. Knowledge on benefits of healthy eating and the importance of physical activity for health is very important for the prevention and treatment of obesity. Schools are conducive to the implementation of health education programs; therefore, teachers should develop interactive and enjoyable strategies for use with their classes to disseminate information to encourage the adoption of a healthy lifestyle. 19
After the intervention, the lipid profile of the IG improved for all measures, except HDL. These results are consistent with other short-term studies of overweight and obese children and adolescents who have combined diet and exercise. 20 , 21 Although there was a reduction in FG in the IG and an increase in FG in the CG, these results were not significant.
A study on lifestyle intervention conducted in Germany with overweight children aged 8–16 years old improved participants’ dietary pattern and was effective in reducing excess weight, %BF, and WC. 22 Leite et al examined the effects of 12 weeks of a program of physical activity and nutritional counseling on obese adolescents and found a reduction in body weight, BMI, WC, TG, and SBP in the adolescents who had more than one risk factor for CVD. 23 These findings are in agreement with our results.
Cardiorespiratory capacity is represented by VO 2max and its value decreases in children with overweight and obesity, being strongly associated with the clustering of cardiovascular risks factors. 24 This observation was explained by the fact that this population participates in organized physical education less than their non-obese peers. 25 In our study, there was a significant increase (2.2%; P < 0.01) in VO 2max in the IG after the intervention, that may be due to an increase of PAL.
The positive results of this study underscore the importance of physical activity combined with orientation toward healthy habits, as well as the benefits of using an illustrative diary, against obesity and other risk factors for CVD, and may be used as subsidies for implementation of interventional programs in schools strategies.
A limitation of this study was the use of subjective methods to measure dietary habits and PAL, thus the extent to which the stated dietary habits and PAL reflect actual habits may be questioned. However, reproducible and validated questionnaires were used to minimize this problem.
The program was effective in reducing risk factors for CVD and the use of an illustrative diary for 10 weeks may have been the key to this result, since the students were motivated to change their poor eating and physical activity habits to healthy ones and increase their PALs.
Future studies should be carried out to evaluate the behavior of the students, to know if the introduced concepts were still in use and if it had affected their PAL. Future studies may require a greater number of students to show a complete set of variables that may be changed within the proposed program.
The authors declare no conflicts of interest in this work.
Global F&V Newsletter
- Vegetable and Fruit Breaks in Australian Primary Schools
- U.S. Fresh Fruit and Vegetable Program: A Win for Children, Schools, Public Health and Agriculture
Fruit and vegetable improvements seen in New Zealand children in the Healthy Homework Pilot Study
- Health Promoting Schools in New Zealand provides Fruit and Leadership

- Partager sur Facebook
- Partager sur LinkedIn
- Partager sur Twitter
Combining the school and home environment
Nutrition and physical activity interventions in children mostly focus on the school setting; however, evidence suggests that children have greater access to unhealthy food and are less active at home 1, 2 .
Funded by the Health Research Council, Healthy Homework is a school-based intervention, that was piloted in two New Zealand schools, with the lowest and highest decile ratings, in 2009 (four intervention, and four control classes). The main aim of the study was to improve dietary and physical activity behaviours in participating children (n=100; aged 9-11 years).
Healthy eating as your homework task– study design
In this study, we developed, implemented, and evaluated the first compulsory homework syllabus aimed at improving key health behaviours outside of school. Ten nutrition and physical activityrelated health behaviours were identified, one of them being fruit and vegetable consumption. The programme consisted of a six-Week homework schedule complemented by an in-class teaching unit, and was designed to support the achievement objectives associated with the New Zealand Health and Physical Education Curriculum.
The fruit and vegetable homework component was not only designed to increase general awareness and promotion relating to fruit and vegetable consumption, but more specifically to encourage students to actively consume the recommended servings i.e. at least two fruit servings and three vegetable servings each day for a week as part of their homework task. Tasks were designed to include family and parental involvement wherever possible, and also included a related question to encourage independent inquiry. Food diaries were used (i.e. four-days; two week days and two weekend days) to assess nutrition intake before and after the intervention. Food diary completion was part of the homework task and it was anticipated that the compliance and accuracy of recording would be adequate. Changes in fruit and vegetable consumption were compared within each group (intervention and control) and between groups pre and post intervention.
Increases in fruit and vegetable consumption shown
In the intervention group there was a significant increase in fruit and vegetable consumption between baseline and follow-up on the weekend (p=0.001). Fruit consumption increased by one half serve (0.5 to 1 serve); vegetable consumption increased by 1.5 serves (0.5 to 2.0). Upon comparison between intervention and control groups, a positive effect was shown for vegetable consumption on weekends (0.83 servings per day, 95% CI: 0.24-1.43; p = 0.007) and overall (0.45 servings per day, 95% CI: 0.09-0.82; p = 0.016), with no significant effect on weekdays. No significant interactions with gender or school were observed.
Importance of findings
This increase in vegetable consumption represents an approximate 28% of the daily vegetable recommendation (three servings per day) 3 and is a noteworthy finding. Our findings are comparable with those of other studies conducted with children but that have focused exclusively on fruit and vegetable intake, which show increases of 0.2-0.6 servings of fruit and vegetables post intervention 4,5 . An improvement in fruit and vegetable consumption was one of the key priorities for the Healthy Homework initiative. Our favourable findings may represent small changes in the home environment that have the potential to extend to other healthy lifestyle patterns.
Future directions
A key question is whether the increase in vegetable consumption extended beyond the timeframe of the intervention, as a longer term follow-up period was not included in this pilot study. A larger Healthy Homework study is currently being conducted in 20 schools across both the North and South islands of New Zealand. A six-month followup period has been incorporated into this study, which will enable both short and long-term effects of the intervention to be determined. At this stage we believe that homework centred on health behaviours that includes family member participation and the home environment is a promising way to enhance fruit and vegetable consumption in children, among other health behaviours. Results from the larger study will hopefully verify this. Future investigations taking a similar approach of encouraging children to actively change their behaviour as a component of their homework to support any theory learned in class time are warranted.
- Rockell JE, Parnell WR, Wilson NC, Skidmore PM, Regan A: Nutrients and foods consumed by New Zealand children on schooldays and non-school days. Public Health Nutr 20101-6.
- Duncan JS, Schofield G, Duncan EK: Pedometer-determined physical activity and body composition in New Zealand children. Med Sci Sports Exerc 2006, 38:1402-1409.
- Ministry of Health. Food And Nutrition Guidelines for Healthy Children Aged 2–12 Years. A background paper. 2003. Ministry of Health: Wellington.
- Blanchette L, Brug J: Determinants of fruit and vegetable consumption among 6-12-year-old children and effective interventions to increase consumption. J Hum Nutr Diet 2005, 18:431-443.
- Knai C, Pomerleau J, Lock K, McKee M: Getting children to eat more fruit and vegetables: a systematic review. Prev Med 2006, 42:85-95.
Masks Strongly Recommended but Not Required in Maryland, Starting Immediately
Due to the downward trend in respiratory viruses in Maryland, masking is no longer required but remains strongly recommended in Johns Hopkins Medicine clinical locations in Maryland. Read more .
- Vaccines
- Masking Guidelines
- Visitor Guidelines
Pilot Study Provides ‘Blueprint’ for Evaluating Diet’s Effect on Brain Health

A new study of 40 older adults with #obesity and insulin resistance randomly assigned to either an #IntermittentFasting diet or a standard healthy diet offers important clues about the potential benefits of both eating plans on #brain health. ›
Researchers from Johns Hopkins Medicine and the National Institutes of Health’s National Institute on Aging say their study of 40 older adults with obesity and insulin resistance who were randomly assigned to either an intermittent fasting diet or a standard healthy diet approved by the U.S. Department of Agriculture (USDA) offers important clues about the potential benefits of both eating plans on brain health.
Insulin resistance is a hallmark of type 2 diabetes and is common in people with obesity. Studies suggest that people with insulin resistance are at higher risk than usual for Alzheimer’s disease and other cognitive impairment. As a result, various weight loss regimens figure widely as ways to reduce risk of these metabolic and brain disorders.
Previous Johns Hopkins research on animal models of diabetes and Alzheimer’s disease showed that intermittent fasting can improve cognition and insulin sensitivity. The new study, published June 19 in Cell Metabolism , tested the effects of intermittent fasting on women and men at risk for cognitive impairment, and it offers a “blueprint,” the authors write, for using a wide panel of biomarkers to assess dietary impact, including analysis of extracellular vesicles — tiny packets of materials shed from neurons, which are types of brain cells that send messages. Such neuron-derived extracellular vesicles are shed into circulating blood and were collected from the new study’s participants during an eight-week period while each person followed one of the two diets.
The results revealed that both types of diet plans had benefits regarding decreasing insulin resistance and improving cognition, with improvements in memory and executive function with both diets, but more strongly with the intermittent fasting diet, according to Mark Mattson, Ph.D. , adjunct professor of neuroscience at the Johns Hopkins University School of Medicine and former chief of the laboratory of neurosciences at the National Institute on Aging in Baltimore. “Other scientists may want to incorporate the (brain) markers (we used) into additional, larger studies of diet and brain health,” Mattson says.
Because people with obesity and insulin resistance may be more at risk of cognitive impairment and Alzheimer’s disease than people with normal metabolism and body mass index (BMI), Dimitrios Kapogiannis, M.D. , chief of the human neuroscience section at the National Institute on Aging and adjunct associate professor of neurology at the Johns Hopkins University School of Medicine, developed a method to isolate neuron-derived extracellular vesicles from blood. His laboratory found molecular evidence of insulin resistance in extracellular vesicles shed from neurons of people with diabetes and Alzheimer’s disease, and because blood samples are relatively easy to collect, they were considered good candidates for widespread use.
To test the effects of the two diets on brain function biomarkers, participants in the new study were recruited from June 2015 and December 2022, and four in-person assessments were completed at facilities run by the National Institute on Aging at MedStar Harbor Hospital in Baltimore. Among the participants, 40 completed their eight-week study. Also, 20 were assigned to an intermittent fasting diet that restricted calories to one-quarter of the recommended daily intake for two consecutive days per week, and they followed the USDA’s healthy living diet — which consists of fruits, vegetables, whole grains, lean proteins, low-fat dairy products and limited added sugars, saturated fats and sodium — for the remaining five days. The USDA’s healthy living diet was assigned to 20 other study participants each day of the week.
The average age of participants in both groups was 63, and 25 were white, 14 were Black and one was Hispanic. There were 24 men and 16 women. All were obese and had insulin resistance.
The researchers found that both diets had equally positive effects on reducing insulin resistance markers in extracellular vesicles, improving BrainAGE (a measurement of the brain’s biological age using structural MRI data) and lowering glucose concentration in the brain. Reduced glucose concentration is a corollary of higher glucose use.
Both diets also improved customary measurements of metabolic health, including weight, BMI, measurement of waist circumference, blood lipids such as cholesterol, and insulin resistance. Executive function and memory (which are a set of mental skills that helps with planning and achieving goals) improved approximately 20% more in the intermittent fasting group than in the healthy living diet group.
A few study participants reported modest side effects including constipation and loose stools, and occasional headaches.
The researchers also saw increased levels of a neurofilament protein (a structural protein in neurons) in both diet groups, but mainly in the intermittent fasting group. What that means regarding brain health is unclear.
“This is a marker to continue to evaluate in further studies,” says Mattson. “Neurons release a lot of proteins, and one idea is that intermittent fasting may be causing some kind of neuroplasticity (a change in structure) in neurons, causing the release of neurofilament proteins.”
The Johns Hopkins researchers and others caution that people interested in intermittent fasting should plan carefully with a health care practitioner because it could be harmful to some people, including those with type 1 diabetes and eating disorders.
The research reported in Cell Metabolism was supported by the National Institutes of Health’s National Institute on Aging (ZIAAG000966, ZIAAG000975).
Other researchers who contributed to the study are Apostolos Manolopoulos, Francheska Delgado-Peraza, Maja Mustapic, Carlos Nogueras-Ortiz, Pamela Yao, Krishna Pucha, Janet Brooks, Qinghua Chen, Lisa Hartnell, Mark Cookson and Josephine Egan from the National Institute on Aging, Roger Mullins from Morgan State University, Konstantinos Avgerinos from Wayne State University, Shalaila Haas and Sophia Frangou from Mount Sinai School of Medicine and Ruiyang Ge from the University of British Columbia.
Academia.edu no longer supports Internet Explorer.
To browse Academia.edu and the wider internet faster and more securely, please take a few seconds to upgrade your browser .
Enter the email address you signed up with and we'll email you a reset link.
- We're Hiring!
- Help Center

Duncan, S., McPhee, J., Schluter, P., Zinn, C., Smith, R., & Schofield, G. (2011). Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: The Healthy Homework Study. International Journal of Behavioral Nutrition and Physical Activity, 8, 127-136

Background: Most physical activity and nutrition interventions in children focus on the school setting; however, evidence suggests that children are less active and have greater access to unhealthy food at home. The aim of this pilot study was to examine the efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children. Methods: The six-week ‘Healthy Homework’ programme and complementary teaching resource was developed under the guidance of an intersectoral steering group. Eight senior classes (year levels 5-6) from two diverse Auckland primary schools were randomly assigned into intervention and control groups. A total of 97 children (57 intervention, 40 control) aged 9-11 years participated in the evaluation of the intervention. Daily step counts were monitored immediately before and after the intervention using sealed multiday memory pedometers. Screen time, sports participation, active transport to and from school, and the consumption of fruits, vegetables, unhealthy foods and drinks were recorded concurrently in a 4-day food and activity diary. Results: Healthy Homework resulted in a significant intervention effect of 2,830 steps.day-1 (95% CI: 560, 5,300, P = 0.013). This effect was consistent between sexes, schools, and day types (weekdays and weekend days). In addition, significant intervention effects were observed for vegetable consumption (0.83 servings.day-1, 95% CI: 0.24, 1.43, P = 0.007) and unhealthy food consumption (-0.56 servings.day-1, 95% CI: -1.05, -0.07, P = 0.027) on weekends but not weekdays, with no interactions with sex or school. Effects for all other variables were not statistically significant regardless of day type. Conclusions: Compulsory health-related homework appears to be an effective approach for increasing physical activity and improving vegetable and unhealthy food consumption in children. Further research in a larger study is required to confirm these initial results.
Related Papers
International Journal of …
Scott Duncan
Background Most physical activity and nutrition interventions in children focus on the school setting; however, evidence suggests that children are less active and have greater access to unhealthy food at home. The aim of this pilot study was to examine the efficacy of a ...
Anindo Majumdar
International Journal of Behavioral Nutrition and Physical Activity
Trish Gorely
Public Health Research
Catherine Chittleborough
BACKGROUND: Previous studies of the effect of school-based interventions to improve healthy behaviours have had important limitations. OBJECTIVE: To investigate the effectiveness of a school-based intervention to increase physical activity, reduce sedentary behaviour and increase fruit and vegetable consumption. DESIGN: Cluster randomised controlled trial. SETTING: Sixty English primary schools. PARTICIPANTS: Children in year 4 (aged 8–9 years) at recruitment, year 5 (aged 9–10 years) during the intervention and immediate follow-up and year 6 (aged 10–11 years) during 1 year of follow-up. INTERVENTION: Active for Life Year 5 (AFLY5) included teacher training, lesson plans, materials for 16 lessons, parent-interactive homework and written materials for school newsletters and parents. MAIN OUTCOME MEASURES: Primary outcome measures included accelerometer-assessed levels of physical activity and sedentary behaviour, and child-reported consumption of fruit and vegetables. Secondary outcome measures included child-reported screen viewing; consumption of snacks, high-fat food and high-energy drinks; body mass index; and waist circumference. RESULTS: We recruited 60 schools (2221 children). At the immediate follow-up, no difference was found between children in intervention and control schools for any of the three primary outcomes. The intervention was effective on three of the nine secondary outcomes; children in intervention schools reported spending less time screen viewing at weekends [–21 minutes per day, 95% confidence interval (CI) –37 to –4 minutes per day], eating fewer servings of snacks per day (–0.22, 95% CI –0.38 to –0.05 servings of snacks per day) and drinking fewer servings of high-energy drinks per day (–0.26, 95% CI –0.43 to –0.10 servings of high-energy drinks per day) than the children in control schools. The results remained consistent 1 year later. The intervention increased children’s perception of maternal efforts to limit the time they spent screen viewing and children’s knowledge about healthy physical activity and fruit and vegetable consumption, with these two mediators explaining approximately one-quarter of the effect of the intervention on screen viewing. The intervention did not affect other mediators. The cost of implementing the intervention from a provider perspective was approximately £18 per child. Process evaluation showed that AFLY5 was implemented with a high degree of fidelity. Teachers supported the aims of AFLY5, but their views of the programme itself were mixed. LIMITATIONS: Responses to parental questionnaires for the economic evaluation were low and we struggled to engage all teachers for the process evaluation. Although the participating schools included a range of levels of socioeconomic deprivation, class sizes and rural and urban settings, we cannot assume that results generalise to all primary schools. CONCLUSIONS: AFLY5 is not effective at increasing levels of physical activity, reducing sedentary behaviour and increasing fruit and vegetable consumption in primary school children, but may be effective in reducing time spent screen viewing at weekends and the consumption of snacks and high-energy drinks. FUTURE WORK: Our findings suggest that school-based interventions are unlikely to have a major impact on promoting healthy levels of physical activity and healthy diets in primary school children. We would recommend trials of the effect and cost-effectiveness of more intensive family and community interventions. TRIAL REGISTRATION: Current Controlled Trials ISRCTN50133740.
Maria Jansen
Schools can help to improve children’s health. The ‘Healthy Primary School of the Future’ (HPSF) aims to sustainably integrate health and well-being into the school system. This study examined the effects of HPSF on children’s dietary and physical activity (PA) behaviours after 1 and 2 years’ follow-up. The study (n = 1676 children) has a quasi-experimental design with four intervention schools, i.e., two full HPSF (focus: nutrition and PA) and two partial HPSF (focus: PA), and four control schools. Accelerometers and child- and parent-reported questionnaires were used at baseline, after 1 (T1) and 2 (T2) years. Mixed-model analyses showed significant favourable effects for the full HPSF versus control schools for, among others, school water consumption (effect size (ES) = 1.03 (T1), 1.14 (T2)), lunch intake of vegetables (odds ratio (OR) = 3.17 (T1), 4.39 (T2)) and dairy products (OR = 4.43 (T1), 4.52 (T2)), sedentary time (ES = −0.23 (T2)) and light PA (ES = 0.22 (T2)). Almost no ...
Nanna Wurr Stjernqvist
11 12 Background: Strategies to improve health behavior and wellbeing of Danish children are 13 needed. A multicomponent intervention “WeAct – together for health” was developed to 14 improve the dietary habits, physical activity and wellbeing among school children aged 10-12 15 years by increasing their health competences and promoting a healthy school environment. 16 This paper describes the development and evaluation of the intervention guided by theory and 17 adjustment to real life setting. 18 19 Methods: The intervention builds upon the health promoting school approach and the IVAC 20 model. The settings are the school and the family. Three educational components targeted the 21 school: 1) Lunch meal habits integrated into science and Danish (“IEAT”) and physical 22 activity integrated into maths (“IMOVE”), 2) Vision workshop integrated primarily into 23 Danish, and 3) the Action and Change process at class and school level. Teachers participated 24 in a course to develop comp...
Archives of Pediatrics & Adolescent Medicine
Graham Colditz
Heidi Bates
Journal of the American Dietetic Association
Paula Quatromoni , Lei Zhu
Loading Preview
Sorry, preview is currently unavailable. You can download the paper by clicking the button above.
RELATED PAPERS
BMC Public Health
Flo Harrison
International Journal of Child Health and Nutrition
Lifescience Global Canada
ISRN Obesity
Anthea Magarey
Health Education Journal
simone casucci
Motricidade
Claudio Tkac
Tara Coppinger , Con Burns , C. O'Neill , Seán Lacey
Muideen Abiodun
Romanian Journal of Diabetes Nutrition and Metabolic Diseases
Cristian Serafinceanu
Connie Mobley , Amy Virus
Public Health Nutrition
Agneta Yngve
Perspectives in Public Health
penney upton
International Journal of Environmental Research and Public Health
francesca celenza
IOSR Journals publish within 3 days
American Journal of Public Health
Bruce Simons-morton
Health Behavior and Policy Review
Deborah H John
Yossi Harel-fisch
Inga Thorsdottir , E. Johannsson
Applied Physiology, Nutrition, and Metabolism
Hawaii medical journal
Alan Titchenal
RELATED TOPICS
- We're Hiring!
- Help Center
- Find new research papers in:
- Health Sciences
- Earth Sciences
- Cognitive Science
- Mathematics
- Computer Science
- Academia ©2024
- Alzheimer's disease & dementia
- Arthritis & Rheumatism
- Attention deficit disorders
- Autism spectrum disorders
- Biomedical technology
- Diseases, Conditions, Syndromes
- Endocrinology & Metabolism
- Gastroenterology
- Gerontology & Geriatrics
- Health informatics
- Inflammatory disorders
- Medical economics
- Medical research
- Medications
- Neuroscience
- Obstetrics & gynaecology
- Oncology & Cancer
- Ophthalmology
- Overweight & Obesity
- Parkinson's & Movement disorders
- Psychology & Psychiatry
- Radiology & Imaging
- Sleep disorders
- Sports medicine & Kinesiology
- Vaccination
- Breast cancer
- Cardiovascular disease
- Chronic obstructive pulmonary disease
- Colon cancer
- Coronary artery disease
- Heart attack
- Heart disease
- High blood pressure
- Kidney disease
- Lung cancer
- Multiple sclerosis
- Myocardial infarction
- Ovarian cancer
- Post traumatic stress disorder
- Rheumatoid arthritis
- Schizophrenia
- Skin cancer
- Type 2 diabetes
- Full List »
share this!
June 25, 2024
This article has been reviewed according to Science X's editorial process and policies . Editors have highlighted the following attributes while ensuring the content's credibility:
fact-checked
peer-reviewed publication
trusted source
Pilot study provides 'blueprint' for evaluating diet's effect on brain health
by Johns Hopkins University
. DOI: 10.1016/j.cmet.2024.05.017")
Researchers from Johns Hopkins Medicine and the National Institutes of Health's National Institute on Aging say their study of 40 older adults with obesity and insulin resistance who were randomly assigned to either an intermittent fasting diet or a standard healthy diet approved by the U.S. Department of Agriculture (USDA) offers important clues about the potential benefits of both eating plans on brain health.
The paper is published in the journal Cell Metabolism .
Insulin resistance is a hallmark of type 2 diabetes and is common in people with obesity. Studies suggest that people with insulin resistance are at higher risk than usual for Alzheimer's disease and other cognitive impairment. As a result, various weight loss regimens figure widely as ways to reduce risk of these metabolic and brain disorders.
Previous Johns Hopkins research on animal models of diabetes and Alzheimer's disease has shown that intermittent fasting can improve cognition and insulin sensitivity. The new study tested the effects of intermittent fasting on women and men at risk for cognitive impairment. It offers a "blueprint," the authors write, for using a wide panel of biomarkers to assess dietary impact, including analysis of extracellular vesicles—tiny packets of materials shed from neurons, which are types of brain cells that send messages. Such neuron-derived extracellular vesicles are shed into circulating blood and were collected from the new study's participants during an eight-week period while each person followed one of the two diets.
The results revealed that both types of diet plans had benefits regarding decreasing insulin resistance and improving cognition, with improvements in memory and executive function with both diets, but more strongly with the intermittent fasting diet, according to Mark Mattson, Ph.D., adjunct professor of neuroscience at the Johns Hopkins University School of Medicine and former chief of the laboratory of neurosciences at the National Institute on Aging in Baltimore.
"Other scientists may want to incorporate the (brain) markers (we used) into additional, larger studies of diet and brain health," Mattson says.
Because people with obesity and insulin resistance may be more at risk of cognitive impairment and Alzheimer's disease than people with normal metabolism and body mass index (BMI), Dimitrios Kapogiannis, M.D., chief of the human neuroscience section at the National Institute on Aging and adjunct associate professor of neurology at the Johns Hopkins University School of Medicine, developed a method to isolate neuron-derived extracellular vesicles from blood. His laboratory found molecular evidence of insulin resistance in extracellular vesicles shed from neurons of people with diabetes and Alzheimer's disease, and because blood samples are relatively easy to collect, they were considered good candidates for widespread use.
To test the effects of the two diets on brain function biomarkers, participants in the new study were recruited from June 2015 and December 2022, and four in-person assessments were completed at facilities run by the National Institute on Aging at MedStar Harbor Hospital in Baltimore.
Among the participants, 40 completed their eight-week study. Also, 20 were assigned to an intermittent fasting diet that restricted calories to one-quarter of the recommended daily intake for two consecutive days per week, and they followed the USDA's healthy living diet—which consists of fruits, vegetables, whole grains, lean proteins, low-fat dairy products and limited added sugars, saturated fats and sodium—for the remaining five days. The USDA's healthy living diet was assigned to 20 other study participants each day of the week.
The average age of participants in both groups was 63, and 25 were white, 14 were Black and one was Hispanic. There were 24 men and 16 women. All were obese and had insulin resistance.
The researchers found that both diets had equally positive effects on reducing insulin resistance markers in extracellular vesicles, improving BrainAGE (a measurement of the brain's biological age using structural MRI data) and lowering glucose concentration in the brain. Reduced glucose concentration is a corollary of higher glucose use.
Both diets also improved customary measurements of metabolic health, including weight, BMI, measurement of waist circumference, blood lipids such as cholesterol, and insulin resistance.
Executive function and memory (which are a set of mental skills that help with planning and achieving goals) improved approximately 20% more in the intermittent fasting group than in the healthy living diet group.
A few study participants reported modest side effects including constipation and loose stools, and occasional headaches.
The researchers also saw increased levels of a neurofilament protein (a structural protein in neurons) in both diet groups, but mainly in the intermittent fasting group. What that means regarding brain health is unclear.
"This is a marker to continue to evaluate in further studies," says Mattson. "Neurons release a lot of proteins, and one idea is that intermittent fasting may be causing some kind of neuroplasticity (a change in structure) in neurons, causing the release of neurofilament proteins."
The Johns Hopkins researchers and others caution that people interested in intermittent fasting should plan carefully with a health care practitioner because it could be harmful to some people, including those with type 1 diabetes and eating disorders.
Explore further
Feedback to editors

Kids given 'digital pacifiers' to calm tantrums fail to learn how to regulate emotions, study finds
2 hours ago

Poorer teen mental ability linked to as much as tripling in stroke risk before age of 50
8 hours ago

'Hidden' sex differences in neurological reward pathways suggest opportunity for improved psychiatric therapeutics
10 hours ago

New study sheds light on potassium channels to help researchers design better drugs

Maternal suicide: New study provides insights into complicating factors surrounding perinatal deaths

Master autoimmune regulator gets by with a little help from its friends

Study finds hypothalamus helps switch between survival tasks
12 hours ago

Study reveals how antibody mAb 77 neutralizes measles virus

Collaboration develop a potent therapy candidate for fatal prion diseases

Naloxone, witnessed overdoses could reduce opioid-related deaths
13 hours ago
Related Stories

Myths about intermittent fasting debunked
Jun 24, 2024

Video: Does intermittent fasting increase heart disease risk?
May 23, 2024

Intermittent fasting aids early diabetes outcomes more than drugs
Jun 25, 2024

Fasting diet reduces risk markers of type 2 diabetes, study finds
Apr 6, 2023

Intermittent fasting may reverse type 2 diabetes
Dec 14, 2022
Does intermittent fasting have benefits for our brain?
Mar 12, 2024
Recommended for you

Vaccination may reduce memory loss from COVID-19 infections
14 hours ago
Let us know if there is a problem with our content
Use this form if you have come across a typo, inaccuracy or would like to send an edit request for the content on this page. For general inquiries, please use our contact form . For general feedback, use the public comments section below (please adhere to guidelines ).
Please select the most appropriate category to facilitate processing of your request
Thank you for taking time to provide your feedback to the editors.
Your feedback is important to us. However, we do not guarantee individual replies due to the high volume of messages.
E-mail the story
Your email address is used only to let the recipient know who sent the email. Neither your address nor the recipient's address will be used for any other purpose. The information you enter will appear in your e-mail message and is not retained by Medical Xpress in any form.
Newsletter sign up
Get weekly and/or daily updates delivered to your inbox. You can unsubscribe at any time and we'll never share your details to third parties.
More information Privacy policy
Donate and enjoy an ad-free experience
We keep our content available to everyone. Consider supporting Science X's mission by getting a premium account.
E-mail newsletter
IMAGES
VIDEO
COMMENTS
Introduction: While most health interventions in children focus on the school setting, evidence suggests that children participate in more unhealthy behaviours outside of school. A potential solution is the introduction of a compulsory health-related homework programme into the school curriculum; however, the feasibility and acceptability of implementing a non-academic homework syllabus in ...
Background Most physical activity and nutrition interventions in children focus on the school setting; however, evidence suggests that children are less active and have greater access to unhealthy food at home. The aim of this pilot study was to examine the efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children. Methods The six-week 'Healthy ...
The Healthy Homework intervention was conducted between August 2011 and August 2012. Figure 1 depicts participant allocation and retention across each phase of the study in the form of a CONSORT flow diagram. A total of 675 children (intervention = 171 boys and 175 girls; control = 155 boys and 174 girls) aged 7-10 years provided written parental consent and assent to participate in the ...
cases, the homework element assumed secondary impor-tance to the school-based components. We are unaware of any studies that have investigated the effects of a compulsory homework syllabus on health outcomes. The aim of this pilot study was to examine the efficacy of a compulsory homework programme for increasing
Funding for the Healthy Homework study was provided by a Health Research Council of New Zealand Project Grant (10-207). ... G. Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: the healthy homework pilot study. Int J Behav Nutr Phys Act. 2011; 8:127. doi: 10.1186/1479-5868-8-127.
Duncan, Scott ; McPhee, Julia C ; Schluter, Philip et al. / Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: the healthy homework pilot study. In: International Journal of Behavioral Nutrition and Physical Activity. 2011 ; Vol. 8. pp. 127 - 136.
Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: the healthy homework pilot study.pdf. Available via license: CC BY 2.0.
The aim of this pilot study was to examine the efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children. ... vegetables, unhealthy foods and drinks were recorded concurrently in a 4-day food and activity diary. Results Healthy Homework resulted in a significant intervention effect of 2,830 ...
healthy eating in children: the healthy homework pilot study. Int J Behav. Nutr Phys Act. 2011;8:127. 28. Abraham C, Michie S. A taxonomy of behavior change techniques used in.
The aim of this pilot study was to examine the efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children. Methods: The six-week 'Healthy Homework' programme and complementary teaching resource was developed under the guidance of an intersectoral steering group.
Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: the healthy homework pilot study (PDF) Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: the healthy homework pilot study | Richard J M Smith - Academia.edu
The aim of this pilot study was to examine the efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children. ... vegetables, unhealthy foods and drinks were recorded concurrently in a 4-day food and activity diary. Healthy Homework resulted in a significant intervention effect of 2,830 steps.day-1 ...
The aim of this pilot study was to examine the efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children.MethodsThe six-week 'Healthy Homework' programme and complementary teaching resource was developed under the guidance of an intersectoral steering group.
these possibilities, however, explain the difference in out- The significant improvements observed in the present comes between AFLY5 and Healthy Homework. One clear study are in contrast to the lack of effects reported by the distinction was that Healthy Homework included a mini- AFLY5 study [25, 26], which featured an intervention de- mum of ...
Recently, promising findings have been demonstrated through a compulsory, health-related homework programme alongside in-class teaching upon primary school-aged children's PA levels (Duncan et al., ... Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: The healthy homework pilot study.
Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: the healthy homework pilot study. Sign in | Create an account. https://orcid.org. Europe PMC. Menu ...
The aim of this pilot study was to examine the efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children. Methods: The six-week 'Healthy Homework' programme and complementary teaching resource was developed under the guidance of an intersectoral steering group. Eight senior classes (year levels ...
Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: the healthy homework pilot study. Authors. Duncan Scott; McPhee Julia C + 4 moreSchluter Philip J; Zinn Caryn; Smith Richard; Schofield Grant; Publication date 1 November 2011. Publisher
For example, a study evaluated the effectiveness of a six-week "Healthy Homework" program to increase physical activity and healthy eating in children aged 9-11 years [53]. Healthy homework ...
These findings corroborate Duncan et al's results. 18 In their study, they also found changes in the PALs and eating habits of schoolchildren in New Zealand after 6 weeks of a program called "Healthy Homework." This program was designed for the physical education curriculum, with the goal of increasing physical activity and healthy eating ...
A key question is whether the increase in vegetable consumption extended beyond the timeframe of the intervention, as a longer term follow-up period was not included in this pilot study. A larger Healthy Homework study is currently being conducted in 20 schools across both the North and South islands of New Zealand.
Researchers from Johns Hopkins Medicine and the National Institutes of Health's National Institute on Aging say their study of 40 older adults with obesity and insulin resistance who were randomly assigned to either an intermittent fasting diet or a standard healthy diet approved by the U.S. Department of Agriculture (USDA) offers important clues about the potential benefits of both eating ...
The aim of this pilot study was to. Background Most physical activity and nutrition interventions in children focus on the school setting; however, evidence suggests that children are less active and have greater access to unhealthy food at home. The aim of this pilot study was to
Conclusions Compared with the control group, the Healthy Homework pilot study resulted approximately 25% more physical activity each day in both boys and girls, and was effective at Page 9 of 10 encouraging activity on both weekdays and weekends. Promising improvements to other important behaviours, such as vegetable and unhealthy food ...
Researchers from Johns Hopkins Medicine and the National Institutes of Health's National Institute on Aging say their study of 40 older adults with obesity and insulin resistance who were randomly ...