Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.

4.2 Basic Concepts
Open Resources for Nursing (Open RN)
Before learning how to use the nursing process, it is important to understand basic concepts concerning how critical thinking relates to nursing practice. Let’s take a deeper look at how nurses think.
Critical Thinking and Clinical Reasoning
Nurses make decisions while providing patient care by using critical thinking and clinical reasoning. Critical thinking is a broad term used in nursing that includes “reasoning about clinical issues such as teamwork, collaboration, and streamlining workflow.” [1] Using critical thinking means that nurses take extra steps to maintain patient safety and don’t just “follow orders.” It also means the accuracy of patient information is validated and plans for caring for patients are based on their needs, current clinical practice, and research.
“Critical thinkers” possess certain attitudes that foster rational thinking. These attitudes are as follows:
- Independence of thought: Thinking on your own
- Fair-mindedness: Treating every viewpoint in an unbiased, unprejudiced way
- Insight into egocentricity and sociocentricity: Thinking of the greater good and not just thinking of yourself. Knowing when you are thinking of yourself (egocentricity) and when you are thinking or acting for the greater good (sociocentricity)
- Intellectual humility: Recognizing your intellectual limitations and abilities
- Nonjudgmental: Using professional ethical standards and not basing your judgments on your own personal or moral standards
- Integrity: Being honest and demonstrating strong moral principles
- Perseverance: Persisting in doing something despite it being difficult
- Confidence: Believing in yourself to complete a task or activity
- Interest in exploring thoughts and feelings: Wanting to explore different ways of knowing
- Curiosity: Asking “why” and wanting to know more
Clinical reasoning is defined as, “A complex cognitive process that uses formal and informal thinking strategies to gather and analyze patient information, evaluate the significance of this information, and weigh alternative actions.” [2] To make sound judgments about patient care, nurses must generate alternatives, weigh them against the evidence, and choose the best course of action. The ability to clinically reason develops over time and is based on knowledge and experience. [3]
Inductive and Deductive Reasoning and Clinical Judgment
Inductive and deductive reasoning are important critical thinking skills. They help the nurse use clinical judgment when implementing the nursing process.
Inductive reasoning involves noticing cues, making generalizations, and creating hypotheses based on specific information or incidents. Cues are data that fall outside of expected findings that give the nurse a hint or indication of a patient’s potential problem or condition. The nurse organizes these cues into patterns and creates a generalization. A generalization is a judgment formed from a set of facts, cues, and observations and is similar to gathering pieces of a jigsaw puzzle into patterns until the whole picture becomes more clear. Based on generalizations created from patterns of data, the nurse creates a hypothesis regarding a patient problem. A hypothesis is a proposed explanation for a situation. It attempts to explain the “why” behind the problem that is occurring. If a “why” is identified, then a solution can begin to be explored.
No one can draw conclusions without first noticing cues. Paying close attention to a patient, the environment, and interactions with family members is critical for inductive reasoning. As you work to improve your inductive reasoning, begin by first noticing details about the things around you. A nurse is similar to the detective looking for cues in Figure 4.1. [4] Be mindful of your five primary senses: the things that you hear, feel, smell, taste, and see. Nurses need strong inductive reasoning patterns and be able to take action quickly, especially in emergency situations. They can see how certain objects or events form a pattern (i.e., generalization) that indicates a common problem (i.e., hypothesis).
Example: A nurse assesses a patient and finds the surgical incision site is red, warm, and tender to the touch. The nurse recognizes these cues form a pattern of signs of infection and creates a hypothesis that the incision has become infected. The provider is notified of the patient’s change in condition, and a new prescription is received for an antibiotic. This is an example of the use of inductive reasoning in nursing practice.

Deductive reasoning is another type of critical thinking that is referred to as “top-down thinking.” Deductive reasoning relies on using a general standard or rule to create a strategy. Deductive reasoning relies on a general statement or hypothesis – sometimes called a premise or standard – that is held to be true. The premise is used to reach a specific, logical conclusion. Nurses use standards set by their state’s Nurse Practice Act, federal regulations, the American Nursing Association, professional organizations, and their employer to make decisions about patient care and solve problems.
Example: Based on research findings, hospital leaders determine patients recover more quickly if they receive adequate rest. The hospital creates a policy for quiet zones at night by initiating no overhead paging, promoting low-speaking voices by staff, and reducing lighting in the hallways. (See Figure 4.2). [5] The nurse further implements this policy by organizing care for patients that promotes periods of uninterrupted rest at night. This is an example of deductive thinking because the intervention is applied to all patients regardless if they have difficulty sleeping or not.

Clinical judgment is the result of critical thinking and clinical reasoning using inductive and deductive reasoning. Clinical judgment is defined by the National Council of State Boards of Nursing (NCSBN) as, “The observed outcome of critical thinking and decision-making. It uses nursing knowledge to observe and assess presenting situations, identify a prioritized patient concern, and generate the best possible evidence-based solutions in order to deliver safe patient care.” [6] The NCSBN administers the national licensure exam (NCLEX) that evaluates the decision-making ability of nursing graduates and sets a minimum standard for safe, competent nursing care by entry-level licensed nurses. The NCLEX uses the NCSBN Clinical Judgment Measurement Model (NCJMM) to measure clinical judgment.
Evidence-based practice (EBP) is defined by the American Nurses Association (ANA) as, “A lifelong problem-solving approach that integrates the best evidence from well-designed research studies and evidence-based theories; clinical expertise and evidence from assessment of the health care consumer’s history and condition, as well as health care resources; and patient, family, group, community, and population preferences and values.” [7]
Nursing Process
The nursing process is a critical thinking model based on a systematic approach to patient-centered care. Nurses use the nursing process to perform clinical reasoning and make clinical judgments when providing patient care. The nursing process is based on the Standards of Professional Nursing Practice established by the American Nurses Association (ANA). These standards are authoritative statements of the actions and behaviors that all registered nurses (RNs), regardless of role, population, specialty, and setting, are expected to perform competently. [8] The mnemonic ADOPIE is an easy way to remember the ANA Standards and the nursing process. Each letter refers to the six components of the nursing process: A ssessment, D iagnosis, O utcomes Identification, P lanning, I mplementation, and E valuation.
The nursing process is a continuous, cyclical process that is constantly adapting to the patient’s current health status. See Figure 4.3 [9] for an illustration of the nursing process.

The ANA’s Standards of Professional Nursing Practice associated with each component of the nursing process are described below.
The “Assessment” Standard of Practice is defined as, “The registered nurse collects pertinent data and information relative to the health care consumer’s health or the situation.” [10] A registered nurse uses a systematic method to collect and analyze patient data. Assessment includes physiological data, as well as psychological, sociocultural, spiritual, economic, and lifestyle data. For example, a nurse’s assessment of a hospitalized patient in pain includes recognizing cues such as the patient’s response to pain, such as the inability to get out of bed, refusal to eat, withdrawal from family members, or anger directed at hospital staff. [11]
Licensed practical/vocational nurses (LPN/VNs) assist with gathering data according to their state’s scope of practice, but do not analyze data because this is outside their scope of practice. The “Assessment” component of the nursing process is further described in the “ Assessment ” section of this chapter.
The “Diagnosis” Standard of Practice is defined as, “The registered nurse analyzes the assessment data to determine actual or potential diagnoses, problems, and issues.” [12] A nursing diagnosis is the nurse’s clinical judgment about the response from the client to actual or potential health conditions or needs. Nursing diagnoses are the bases for the nurse’s care plan and are different than medical diagnoses. [13]
Analyzing assessment data and formulating a nursing diagnosis is outside the scope of practice for LPN/VNs, and as such, they do not assist with this phase of the nursing process. The “Diagnosis” component of the nursing process is further described in the “ Diagnosis ” section of this chapter.
Outcome Identification
The “Outcome Identification” Standard of Practice is defined as, “The registered nurse identifies expected outcomes for a plan individualized to the health care consumer or the situation.” [14] The nurse sets measurable and achievable short- and long-term goals and specific outcomes in collaboration with the patient based on their assessment data and nursing diagnoses.
Outcome identification is outside the scope of practice of LPN/VNs, and as such, they do not assist with this phase of the nursing process. The “Outcome Identification” component of the nursing process is further described in the “ Outcome Identification ” section of this chapter.
The “Planning” Standard of Practice is defined as, “The registered nurse develops a collaborative plan encompassing strategies to achieve expected outcomes.” [15] Assessment data, diagnoses, and goals are used to select evidence-based nursing interventions customized to each patient’s needs in order to achieve their previously established goals and outcomes. Nursing interventions are planned and documented by RNs in the client’s nursing care plan so that nurses, as well as other health professionals, can refer to it for continuity of care. [16]
The “Planning” component of the nursing process is further described in the “ Planning ” section of this chapter.
Nursing Care Plans
Creating nursing care plans is a part of the “Planning” step of the nursing process. A nursing care plan is a type of documentation that demonstrates the individualized planning and delivery of nursing care for each specific patient using the nursing process. RNs create nursing care plans so that the care provided to the patient across shifts is consistent among health care personnel. Some interventions can be delegated to LPN/VNs or trained Unlicensed Assistive Personnel (UAPs) with RN supervision.
Creating the nursing care plan is outside the scope of practice, and as such, the LPN/VNs do not perform this task, although they may contribute to it. Developing nursing care plans and implementing appropriate delegation are further discussed under the “ Planning ” and “ Implementation of Interventions ” sections of this chapter.
Implementation
The “Implementation” Standard of Practice is defined as, “The nurse implements the identified plan.” [17] Nursing interventions are implemented or delegated with supervision according to the care plan to assure continuity of care across multiple nurses and health professionals caring for the patient. Interventions are documented in the patient’s electronic medical record as they are completed. [18] LPN/VNs implement interventions contained in the nursing care plan, provided they are within their scope of practice. The LPN/VN is responsible for documenting the interventions they perform in the client’s medical record.
The “Implementation” Standard of Professional Practice also includes the subcategories “Coordination of Care” and “Health Teaching and Health Promotion” to promote health and a safe environment. [19]
The “Implementation” component of the nursing process is further described in the “ Implementation of Interventions ” section of this chapter.
The “Evaluation” Standard of Practice is defined as, “The registered nurse evaluates progress toward attainment of goals and outcomes.” [20] During evaluation, nurses reassess the patient and compare the findings against established outcomes to determine the effectiveness of the interventions and overall nursing care plan. During this phase, RNs ask, “Were outcomes met? Are any modifications required for the nursing care plan?” Both the patient’s status and the effectiveness of the nursing care plan are continuously evaluated and modified as needed. [21]
Evaluating and modifying the nursing care plan is outside the scope of practice of LPN/VNs, although they can assist in gathering assessment data to assist the RN in performing this step of the nursing process. The “Evaluation” component of the nursing process is further described in the “ Evaluation ” section of this chapter.
Benefits of Using the Nursing Process
Using the nursing process has many benefits for nurses, patients, and other members of the health care team. The benefits of using the nursing process include the following:
- Promotes quality patient care
- Decreases omissions and duplications
- Provides a guide for all staff involved to provide consistent and responsive care
- Encourages collaborative management of a patient’s health care problems
- Improves patient safety
- Improves patient satisfaction
- Identifies a patient’s goals and strategies to attain them
- Increases the likelihood of achieving positive patient outcomes
- Saves time, energy, and frustration by creating a care plan that is accessible to all staff caring for a client
By using these components of the nursing process as a critical thinking model, nurses plan outcomes and interventions that are customized to the client’s specific needs, ensure the interventions are evidence-based, and evaluate the effectiveness of interventions in meeting the client’s needs.
NCSBN Clinical Judgment Measurement Model
The NCSBN Clinical Judgment Measurement Model (NCJMM) complements the nursing process, but it is a model that assesses an NCLEX candidate’s clinical judgment. Terminology used by this model includes recognize cues, analyze cues, prioritize hypotheses, generate solutions, take action, and evaluate outcomes. See Figure 4.3b [22] and Table 4.2a for comparisons of NCJMM terms and the nursing process. [23] , [24] , [25]
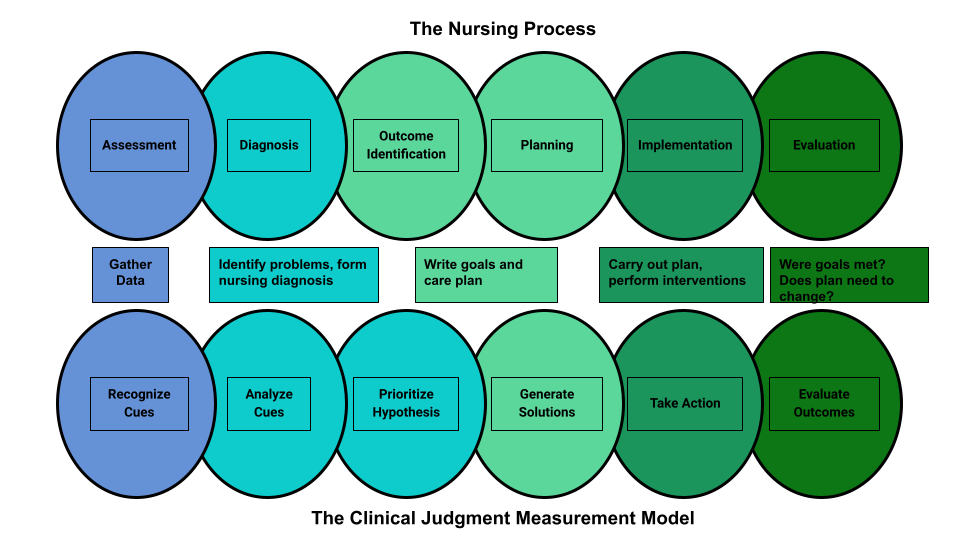
Figure 4.3b Comparison of the Steps of the NCJMM to the Nursing Process
Table 4.2a Comparison of the NCJMM to the Nursing Process
| Determining what client findings are significant, most important, and of immediate concern to the nurse (i.e., identifying “relevant cues”). | ||
| Analyzing data to determine if it is “expected” or “unexpected” or “normal” or “abnormal” for this client at this time according to their age, development, and clinical status. Making a clinical judgment concerning the client’s “human response to health conditions/life processes, or a vulnerability for that response”; also referred to as “forming a hypothesis.” | (Analysis of Data) | |
| Ranking client conditions and problems according to urgency, complexity, and time. | ||
| Planning individualized interventions that meet the desired outcomes for the client; may include gathering additional assessment data. | ||
| Implementing interventions that are safe and most appropriate for the client’s current priority conditions and problems. | ||
| Comparing actual client outcomes with desired client outcomes to determine effectiveness of care and making appropriate revisions to the nursing care plan. |
Learning activities are incorporated throughout this book to help students practice answering NCLEX Next Generation-style test questions.
Review Scenario A in the following box for an example of a nurse using the nursing process and NCJMM skills while providing patient care.
Client Scenario A : Using the Nursing Process [26]

A nurse is caring for a hospitalized client with a medical diagnosis of heart failure who has a prescription to receive furosemide 80mg IV every morning. The nurse uses critical thinking according to the nursing process and the NCJMM before administering the prescribed medication:
Assessment/Recognize Cues: During the morning assessment, the nurse notes that the patient has a blood pressure of 98/60, heart rate of 100, respirations of 18, and a temperature of 98.7F.
Diagnosis/Analyze Cues: The nurse reviews the medical record for the patient’s vital signs baseline and observes the blood pressure trend is around 110/70 and the heart rate in the 80s.
Planning/Prioritize Hypothesis: The nurse recognizes cues (assessment data) that form a pattern related to fluid imbalance and hypothesizes that the patient may be dehydrated.
Planning/Generate Solutions: The nurse gathers additional information and notes the patient’s weight has decreased four pounds since yesterday. The nurse talks with the patient and validates the hypothesis when the patient reports that their mouth feels like cotton, and they feel light-headed. By using critical thinking and clinical judgment, the nurse diagnoses the patient with the nursing diagnosis Fluid Volume Deficit and plans interventions for reestablishing fluid balance.
Implementation/Take Action: The nurse withholds the administration of IV furosemide and contacts the health care provider to discuss the patient’s current fluid status. After contacting the provider, the nurse initiates additional nursing interventions to promote oral intake and closely monitors hydration status.
Evaluation/Evaluate Outcomes: By the end of the shift, the nurse evaluates the patient status and determines that fluid balance has been restored.
In Scenario A, the nurse is using clinical judgment and not just “following orders” to administer the Lasix as scheduled. The nurse assesses the patient, recognizes and analyzes cues, creates a hypothesis regarding the fluid status, plans and implements nursing interventions, and evaluates outcomes. While performing these steps, the nurse promotes client safety by contacting the provider before administering a medication that could cause harm to the client at this time.
Holistic Nursing Care
Using the nursing process and clinical judgment while implementing evidence-based practices is referred to as the “science of nursing.” Before getting deeper into the science of nursing in the remainder of this chapter, it is important to discuss the “art of nursing” that relies on holistic care provided in a compassionate and caring manner using the nursing process.
The American Nurses Association (ANA) defines nursing as, “Nursing integrates the art and science of caring and focuses on the protection, promotion, and optimization of health and human functioning; prevention of illness and injury; facilitation of healing; and alleviation of suffering through compassionate presence. Nursing is the diagnosis and treatment of human responses and advocacy in the care of individuals, families, groups, communities, and populations in the recognition of the connection of all humanity.” [27]
The ANA further describes nursing as a learned profession built on a core body of knowledge that integrates both the art and science of nursing. The art of nursing is defined as, “Unconditionally accepting the humanity of others, respecting their need for dignity and worth, while providing compassionate, comforting care.” [28]
Nurses care for individuals holistically, including their emotional, spiritual, psychosocial, cultural, and physical needs. They consider problems, issues, and needs that the person experiences as a part of a family and a community as they use the nursing process. Review a scenario illustrating holistic nursing care provided to a patient and their family in the following box.
Holistic Nursing Care Scenario
A single mother brings her child to the emergency room for ear pain and a fever. The physician diagnoses the child with an ear infection and prescribes an antibiotic. The mother is advised to make a follow-up appointment with their primary provider in two weeks. While providing discharge teaching, the nurse discovers that the family is unable to afford the expensive antibiotic prescribed and cannot find a primary care provider in their community they can reach by a bus route. The nurse asks a social worker to speak with the mother about affordable health insurance options and available providers in her community and follows up with the prescribing physician to obtain a prescription for a less expensive generic antibiotic. In this manner, the nurse provides holistic care and advocates for improved health for the child and their family.
Caring and the Nursing Process
The American Nurses Association (ANA) states, “The act of caring is foundational to the practice of nursing.” [29] Successful use of the nursing process requires the development of a care relationship with the patient. A care relationship is a mutual relationship that requires the development of trust between both parties. This trust is often referred to as the development of rapport and underlies the art of nursing. While establishing a caring relationship, the whole person is assessed, including the individual’s beliefs, values, and attitudes, while also acknowledging the vulnerability and dignity of the patient and family. Assessing and caring for the whole person takes into account the physical, mental, emotional, and spiritual aspects of being a human being. [30] Caring interventions can be demonstrated in simple gestures such as active listening, making eye contact, using therapeutic touch, and providing emotional support while respecting their cultural beliefs associated with caring behaviors. [31] See Figure 4.4 [32] for an image of a nurse using touch as a therapeutic communication technique to communicate caring.
Dr. Jean Watson is a nurse theorist who has published many works on the art and science of caring in the nursing profession. Her theory of human caring sought to balance the cure orientation of medicine, giving nursing its unique disciplinary, scientific, and professional standing with itself and the public. Dr. Watson’s caring philosophy encourages nurses to be authentically present with their patients while creating a healing environment. [33]

Now that we have discussed basic concepts related to the nursing process, as well as the science and art of nursing, let’s look more deeply at each component of the nursing process in the following sections.
- Klenke-Borgmann, L., Cantrell, M. A., & Mariani, B. (2020). Nurse educator’s guide to clinical judgment: A review of conceptualization, measurement, and development. Nursing Education Perspectives, 41 (4), 215-221. ↵
- Powers, L., Pagel, J., & Herron, E. (2020). Nurse preceptors and new graduate success. American Nurse Journal, 15 (7), 37-39. ↵
- “ The Detective ” by paurian is licensed under CC BY 2.0 ↵
- “ In the Quiet Zone… ” by C.O.D. Library is licensed under CC BY-NC-SA 2.0 ↵
- NCSBN. (n.d.). NCSBN clinical judgment model . https://www.ncsbn.org/14798.htm ↵
- American Nurses Association. (2021). Nursing: Scope and standards of practice (4th ed.). American Nurses Association. ↵
- “ The Nursing Process ” by Kim Ernstmeyer at Chippewa Valley Technical College is licensed under CC BY 4.0 ↵
- American Nurses Association. (n.d.). The nursing process. https://www.nursingworld.org/practice-policy/workforce/what-is-nursing/the-nursing-process/ ↵
- American Nurses Association. (n.d.). The nursing process . https://www.nursingworld.org/practice-policy/workforce/what-is-nursing/the-nursing-process/ ↵
- American Nurses Association. (2021). Nursing: Scope and standards of practice (3rd ed.). American Nurses Association. ↵
- American Nurses Association. (n.d.) The nursing process. https://www.nursingworld.org/practice-policy/workforce/what-is-nursing/the-nursing-process / ↵
- American Nurses Association. (n.d.). The nursing process. https://www.nursingworld.org/practice-policy/workforce/what-is-nursing/the-nursing-process / ↵
- “ Nursing Process and NCJMM ” by Tami Davis is licensed under CC BY 4.0 ↵
- NCSBN (n.d.) NCSBN Clinical Judgment Measurement Model. https://www.ncsbn.org/14798.htm ↵
- Ignativicius, V., & Silvestri, L. (2022). Preparing for the Next-Generation NCLEX (NGN): A “how-to” step-by-step faculty resource manual. Elsevier. https://evolve.elsevier.com/education/wp-content/uploads/sites/2/NGN_FacultyGuide_Final.pdf ↵
- “Patient Image in LTC.JPG” by ARISE project is licensed under CC BY 4.0 ↵
- Walivaara, B., Savenstedt, S., & Axelsson, K. (2013). Caring relationships in home-based nursing care - registered nurses’ experiences. The Open Journal of Nursing, 7 , 89-95. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3722540/pdf/TONURSJ-7-89.pdf ↵
- “ hospice-1793998_1280.jpg ” by truthseeker08 is licensed under CC0 ↵
- Watson Caring Science Institute. (n.d.). Watson Caring Science Institute. Jean Watson, PHD, RN, AHN-BC, FAAN, (LL-AAN) . https://www.watsoncaringscience.org/jean-bio/ ↵
Reasoning about clinical issues such as teamwork, collaboration, and streamlining workflow.
A complex cognitive process that uses formal and informal thinking strategies to gather and analyze patient information, evaluate the significance of this information, and weigh alternative actions.
A type of reasoning that involves forming generalizations based on specific incidents.
Subjective or objective data that gives the nurse a hint or indication of a potential problem, process, or disorder.
A judgment formed from a set of facts, cues, and observations.
A proposed explanation for a situation. It attempts to explain the “why” behind the problem that is occurring.
“Top-down thinking” or moving from the general to the specific. Deductive reasoning relies on a general statement or hypothesis—sometimes called a premise or standard—that is held to be true. The premise is used to reach a specific, logical conclusion.
The observed outcome of critical thinking and decision-making. It is an iterative process that uses nursing knowledge to observe and access presenting situations, identify a prioritized client concern, and generate the best possible evidence-based solutions in order to deliver safe client care.
A lifelong problem-solving approach that integrates the best evidence from well-designed research studies, theories, clinical expertise, health care resources, and patient preferences and values.
An easy way to remember the ANA Standards and the nursing process. Each letter refers to the six components of the nursing process: Assessment, Diagnosis, Outcomes Identification, Planning, Implementation, and Evaluation.
Individual, family, or group which includes significant others and populations.
Specific documentation of the planning and delivery of nursing care that is required by the Joint Commission.
Nursing integrates the art and science of caring and focuses on the protection, promotion, and optimization of health and human functioning; prevention of illness and injury; facilitation of healing; and alleviation of suffering through compassionate presence. Nursing is the diagnosis and treatment of human responses and advocacy in the care of individuals, families, groups, communities, and populations in recognition of the connection of all humanity.
A relationship described as one in which the whole person is assessed while balancing the vulnerability and dignity of the patient and family.
Developing a relationship of mutual trust and understanding.
Nursing Fundamentals Copyright © by Open Resources for Nursing (Open RN) is licensed under a Creative Commons Attribution 4.0 International License , except where otherwise noted.
Share This Book
The First Step: Ask; Fundamentals of Evidence-Based Nursing Practice
In this module, we will learn about identifying the problem, start the “Ask” process with developing an answerable clinical question, and learn about purpose statements and hypotheses.
Content includes:
- Identifying the problem
- Determining the Population, Intervention, Comparison, and Outcome (PICO)
- Asking a Research/Clinical Question (Based on PICO)
Statements of Purpose
Objectives:
- Describe the process of developing a research/practice problem.
- Describe the components of a PICO.
- Identify different types of PICOs.
- Distinguish function and form of statements of purpose.
- Describe the function and characteristics of hypotheses.
Development of a Research/Practice Problem
Practice questions frequently arise from day-to-day problems that are encountered by providers (Dearholt & Dang, 2012). Often, these problems are very obvious. However, sometimes we need to back up and take a close look at the status quo to see underlying issues. The basis for any research project is indeed the underlying problem or issue. A good problem statement or paragraph is a declaration of what it is that is problematic or what it is that we do not know much about (a gap in knowledge) (Polit & Beck, 2018).
The process of defining the practice/clinical problem begins by seeking answers to clinical concerns. This is the first step in the EBP process: To ask . We start by asking some broad questions to help guide the process of developing our practice problem.
- Is there evidence that the current treatment works?
- Does the current practice help the patient?
- Why are we doing the current practice?
- Should we be doing the current practice this way?
- Is there a way to do this current practice more efficiently?
- Is there a more cost-effective method to do this practice?
Problem Statements:
For our EBP Project, we will need to ask these broad questions and then develop our problem that exists. This establishes the “background” of the issue we want to know more about.
For example, if we are choosing a clinical question based on wanting to know if adjunct music therapy helps decrease postoperative pain levels than just pharmaceuticals alone, we might consider the underlying problems of:
- Postoperative pain is not adequately managed in greater than 80% of patients in the US, although rates vary depending on such factors as type of surgery performed, analgesic/anesthetic intervention used, and time elapsed after surgery (Gan, 2017).
- Poorly controlled acute postoperative pain is associated with increased morbidity, functional and quality-of-life impairment, delayed recovery time, prolonged duration of opioid use, and higher health-care costs (Gan, 2017).
- Multimodal analgesic techniques are widely used but new evidence is disappointing (Rawal, 2016).
In the above examples, we are establishing that poorly managed postoperative pain is a problem. Thus, looking at evidence about adjunctive music therapy may help to address how we might manage pain more effectively. These are our problem statements. This would be our introduction section on the EBP poster. For the sake of our EBP poster, you do not need to list these on the poster references. A heads up: The sources used to help develop our research/clinical program should not be the same resources that we use to answer our upcoming clinical question. In essence, we will be conducting two literature reviews: One, to establish the underlying problem; and, two: To find published research that helps to answer our developed clinical question.
Here is the introduction to the article titled, “The relationships among pain, depression, and physical activity in patients with heart failure” (Haedtke et al, 2017). You can read that the underlying problem is multifocal: 67% of patient with heart failure (HF) experience pain, depression is a comorbidity that affects 22% to 42% of HF patients, and that little attention has been paid to this relationship in patients with HF. The researchers have established the need for further research and why further research is needed.

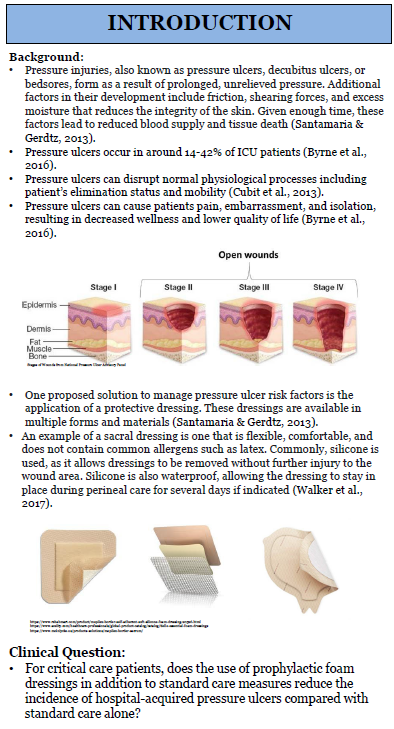
Here is another example of how the clinical problem is addressed in an EBP poster that wants to appraise existing evidence related to dressing choice for decubitus ulcers.
When trying to communicate clinical problems, there are two main sources (Titler et al, 1994, 2001):
- Problem-focused triggers : These are identified by staff during routine monitoring of quality, risk, adverse events, financial, or benchmarking data.
- Knowledge-focused triggers : There are identified through reading published evidence or learning new information at conferences or other professional meetings.
Sources of Evidence-Based Clinical Problems:
| Triggers | Sources of Evidence |
| Problem-focused |
|
| Knowledge-focused |
Most problem statements have the following components:
- Problem identification: What is wrong with the current situation or action?
- Background: What is the nature of the problem or the context of the situation? (this helps to establish the why)
- Scope of the problem: How many people are affected? Is this a small problem? Big problem? Potential to grow quickly to a large problem? Has been increasing/decreasing recently?
- Consequences of the problem: If we do nothing or leave as the status quo, what is the cost of not fixing the issue?
- Knowledge gaps: What information about the problem is lacking? We need to know what we do not know.
- Proposed solution: How will the information or evidence contribute to the solution of the problem?
If you are stumped on a topic, ask faculty, RNs at local facilities, colleagues, and key stakeholders at local facilities for some ideas! There is usually “something” that the nursing field is concerned about or has questions about.
Components of a PICO Question
After we have asked ourselves some background questions, we need to develop a foreground (focused) question. A thoughtful development of a well-structured foreground clinical/practice question is important because the question drives the strategies that you will use to search for the published evidence. The question needs to be very specific, non-ambiguous , and measurable in order to find the relevant evidence needed and also increased the likelihood that you will find what you are looking for.
In developing your clinical/practice question, there is a helpful format to utilize to establish the key component. This format includes the Patient/Population, Intervention/Influence/Exposure, Comparison, and Outcome (PICO) (Richardson, Wilson, Nishikawa, & Hayward, 1995).
Let’s dive into each component to better understand.
P atient, population, or problem: We want to describe the patient, the population, or the problem. Get specific. We will want to know exactly who we are wanting to know about. Consider age, gender, setting of the patient (e.g. postoperative), and/or symptoms.
I ntervention: The intervention is the action or, in other words, the treatment, process of care, education given, or assessment approaches. We will come back to this in more depth, but for now remember that the intervention is also called the “Independent Variable”.
C omparison: Here we are comparing with other interventions. A comparison can be standard of care that already exists, current practice, an opposite intervention/action, or a different intervention/action.
O utcome: What is that that we are looking at for a result or consequence of the intervention? The outcome needs to have a metric for actually measuring results. The outcome can include quality of life, patient satisfaction, cost impacts, or treatment results. The outcome is also called the “Dependent Variable”.
The PICO question is a critical aspect of the EBP project to guide the problem identification and create components that can be used to shape the literature search.

Let’s watch a nice YouTube video, “PICO: A Model for Evidence-Based Research”:
“PICO: A Model for Evidence Based Research” by Binghamton University Libraries. Licensed CCY BY .
Great! Okay, let’s move on and discuss the various types of PICOs.
Types of PICOs
Before we start developing our clinical question, let’s go over the various types of PICOs and the clinical question that can result from the components. There are various types of PICOs but we are concerned with the therapy/treatment/intervention format of PICO for our EBP posters.
Let’s take a look at the various types of PICOs:
| Type of Question | PICO Template |
| Therapy/Intervention/Treatment (We will use this type for our EBP Posters) | In _________ (Population), what is the effect of ___________ (Intervention) in comparison to ___________(Comparison) on __________ (Outcome)? Or Does _________ (Intervention) compared to __________ (Comparison) decrease/increase ______________ (Outcome) in ____________ (Population)?
|
| Diagnosis/Assessment | For _________ (Population), does __________ (Identifying tool/procedure) yield more accurate or more appropriate diagnostic/assessment information than __________ (Comparative tool/procedure) about __________ (Outcome)?
|
| Prognosis | For ______ (Population), does _______ (Exposure to disease or condition), relative to _______ (Comparative disease or condition) increase the risk of ________ (Outcome)?
|
| Etiology/Harm | Does (Influence, exposure, or characteristic) increase the risk of ________ (Outcome) compared to ________ (Comparative influence, exposure, or condition) in ________ (Population)?
|
| Description (Prevalence/Incidence) | These questions vary from the typical PICO in that explicit comparisons are not typical (except to compare population). In ______ (Population), how prevalent is ________ (Outcome)?
|
| Meaning or Process | Explicit comparisons are not typical in these types of questions. These are qualitative questions and are used to elicit narrative, subjective responses. What is it like for ________ (Population) to experience _________ (situation, condition, circumstance)?
|
The first step in developing a research or clinical practice question is developing your PICO. Well, we’ve done that above. You will select each component of your PICO and then turn that into your question. Making the EBP question as specific as possible really helps to identify specific terms and narrow the search, which will result in reducing the time it times searching for relevant evidence.
Once you have your pertinent clinical question, you will use the components to begin your search in published literature for articles that help to answer your question. In class, we will practice with various situations to develop PICOs and clinical questions.
Many articles have the researcher’s statement of purpose (sometimes referred to as “aim”, “goal”, or “objective”) for their research project. This helps to identify what the overarching direction of inquiry may be. You do not need a statement of purpose/aim/goal/objective for your EBP poster. However, knowing what a statement of purpose is will help you when appraising articles to help answer your clinical question.
The following statement of purpose was written as an aim. The population (P) was identified as patients with HF, the interventions (I) included physical activity/exercise, and the outcomes (O) included pain, depression, total activity time, and sitting time as correlated with the interventions.
In the articles above, the authors made it easy and included their statements of purpose within the abstract at the beginning of the article. Most articles do not feature this ease, and you will need to read the introduction or methodology section of the article to find the statement of purpose, much like within article 3.1.
In qualitative studies, the statement of purpose usually indicates the nature of the inquiry, the key concept, the key phenomenon, and the population.
Function and Characteristics of Hypotheses.
A hypothesis (plural: hypothes es ) is a statement of predicted outcome. Meaning, it is an educated and formulated guess as to how the intervention (independent variable – more on that soon!) impacts the outcome (dependent variable). It is not always a cause and effect. Sometimes there can be just a simple association or correlation. We will come back to that in a few modules.
In your PICO statement, you can think of the “I” as the independent variable and the “O” as the dependent variable . Variables will begin making more sense as we go. But for now, remember this:
Independent Variable (IV): This is a measure that can be manipulated by the researcher. Perhaps it is a medication, an educational program, or a survey. The independent variable enacts change (or not) onto the independent variable.
Dependent Variable (DV): This is the result of the independent variable. This is the variable that we utilize statistical analyses to measure. For instance, if we are intervening with a blood pressure medication (our IV), then our DV would be the measurement of the actual blood pressure.
Most of the time, a hypothesis results from a well-worded research question. Here is an example:
Research Question : “Does sexual abuse in childhood affect the development of irritable bowel syndrome in women?”
Research Hypothesis : Women (P) who were sexually abused in childhood (I) have a higher incidence of irritable bowel syndrome (O) than women who were not abused (C).
You may note in that hypothesis that there is a predicted direction of outcome. One thing leads to something.
But, why do we need a hypothesis? First, they help to promote critical thinking. Second, it gives the researcher a way to measure a relationship. Suppose we conducted a study guided only by a research question. Take the above question, for example. Without a hypothesis, the researcher is seemingly prepared to accept any result (Polit & Beck, 2021). The problem with that is that it is almost always possible to explain something superficially after the fact, even if the findings are inconclusive. A hypothesis reduces the possibility that spurious results will be misconstrued (Polit & Beck, 2021).

Not all research articles will list a hypothesis. This makes it more difficult to critically appraise the results. That is not to say that the results would be invalidated, but it should ignite a spirit of further inquiry as to if the results are valid.
Hypotheses (also called alternative hypothesis) can be stated as:
- Directional or nondirectional
- Simple or complex
- Research or Null
Simple hypothesis : Statement of causal (cause and effect) relationship – one independent variable (intervention) and one dependent variable (outcome).
Example : If you stay up late, then you feel tired the next day.
Complex hypothesis : Statement of causal (cause and effect) or associative (not causal) between two or more independent variables (interventions) and/or two or more dependent variables (outcomes).
Example : Higher the poverty, higher the illiteracy in society, higher will be the rate of crime (three variables – two independent variables and one dependent variable).
Directional hypothesis : Specifies not only the existence but also the expected direction of the relationship between the dependent (outcome) and the independent (intervention) variables. You will also see this called “One-tailed hypothesis”.
Example : Depression scores will decrease following a 6-week intervention.
Nondirectional hypothesis : Does not specify the direction of relationship between the variables. You will also see this called “Two-tailed hypothesis”.
Example : College students will perform differently from elementary school students on a memory task (without predicting which group of students will perform better).

Null hypothesis : The null hypothesis assumes that any kind of difference between the chosen characteristics that you see in a set of data is due to chance. Now, the null hypothesis is why the plain old hypothesis is also called alternative hypothesis. We don’t just assume that the hypothesis is true. So, it is considered an alternative to something just happening by chance (null).
Example : Let’s say our research question is, “Do teens use cell phones to access the internet more than adults?” – our null hypothesis could state: Age has no effect on how cell phones are used for internet access.
And then, further develop the problem and background through finding existing literature to help answer the following questions:
- Knowledge gaps: What information about the problem is lacking? We need to know what we do not know.
With the previous example of pain in the pediatric population, here is an example of an Introduction section from a past student poster:
- What was the research problem? Was the problem statement easy to locate and was it clearly stated? Did the problem statement build a coherent and persuasive argument for the new study?
- Does the problem have significance for nursing?
- Was there a good fit between the research problem and the paradigm (and tradition) within which the research was conducted?
- Did the report formally present a statement of purpose, research question, and/or hypotheses? Was this information communicated clearly and concisely, and was it placed in a logical and useful location?
- Were purpose statements or research questions worded appropriately (e.g., were key concepts/variables identified and the population specified?
- If there were no formal hypotheses, was their absence justified? Were statistical tests used in analyzing the data despite the absence of stated hypotheses?
- Were hypotheses (if any) properly worded—did they state a predicted relationship between two or more variables? Were they presented as research or as null hypotheses?
References & Attribution
“ Green check mark ” by rawpixel licensed CC0 .
“ Light bulb doodle ” by rawpixel licensed CC0 .
“ Magnifying glass ” by rawpixel licensed CC0
“ Orange flame ” by rawpixel licensed CC0 .
Chen, P., Nunez-Smith, M., Bernheim, S… (2010). Professional experiences of international medical graduates practicing primary care in the United States. Journal of General Internal Medicine, 25 (9), 947-53.
Dearholt, S.L., & Dang, D. (2012). Johns Hopkins nursing evidence-based practice: Model and guidelines (2nd Ed.). Indianapolis, IN: Sigma Theta Tau International.
Gan, T. (2017). Poorly controlled postoperative pain: Prevalence, consequences, and prevention. Journal of Pain Research, 10, 2287-2298.
Genc, A., Can, G., Aydiner, A. (2012). The efficiency of the acupressure in prevention of the chemotherapy-induced nausea and vomiting. Support Care Cancer, 21 , 253-261.
Haedtke, C., Smith, M., VanBuren, J., Kein, D., Turvey, C. (2017). The relationships among pain, depression, and physical activity in patients with heart failure. Journal of Cardiovascular Nursing, 32 (5), E21-E25.
Pankong, O., Pothiban, L., Sucamvang, K., Khampolsiri, T. (2018). A randomized controlled trial of enhancing positive aspects of caregiving in Thai dementia caregivers for dementia. Pacific Rim Internal Journal of Nursing Res, 22 (2), 131-143.
Polit, D. & Beck, C. (2021). Lippincott CoursePoint Enhanced for Polit’s Essentials of Nursing Research (10th ed.). Wolters Kluwer Health.
Rawal, N. (2016). Current issues in postoperative pain management. European Journal of Anaesthesiology, 33 , 160-171.
Richardson, W.W., Wilson, M.C., Nishikawa, J., & Hayward, R.S. (1995). The well-built clinical question: A key to evidence-based decisions. American College of Physicians, 123 (3), A12-A13.
Titler, M. G., Kleiber, C., Steelman, V.J. Rakel, B. A. Budreau, G., Everett,…Goode, C.J. (2001). The Iowa model of evidence-based practice to promote quality care. Critical Care Nursing Clinics of North America, 13 (4), 497-509.
Evidence-Based Practice & Research Methodologies Copyright © by Tracy Fawns is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License , except where otherwise noted.
Share This Book

The P value: What it really means
As nurses, we must administer nursing care based on the best available scientific evidence. But for many nurses, critical appraisal, the process used to determine the best available evidence, can seem intimidating. To make critical appraisal more approachable, let’s examine the P value and make sure we know what it is and what it isn’t.
Defining P value
The P value is the probability that the results of a study are caused by chance alone. To better understand this definition, consider the role of chance.
The concept of chance is illustrated with every flip of a coin. The true probability of obtaining heads in any single flip is 0.5, meaning that heads would come up in half of the flips and tails would come up in half of the flips. But if you were to flip a coin 10 times, you likely would not obtain heads five times and tails five times. You’d be more likely to see a seven-to-three split or a six-to-four split. Chance is responsible for this variation in results.
Just as chance plays a role in determining the flip of a coin, it plays a role in the sampling of a population for a scientific study. When subjects are selected, chance may produce an unequal distribution of a characteristic that can affect the outcome of the study. Statistical inquiry and the P value are designed to help us determine just how large a role chance plays in study results. We begin a study with the assumption that there will be no difference between the experimental and control groups. This assumption is called the null hypothesis. When the results of the study indicate that there is a difference, the P value helps us determine the likelihood that the difference is attributed to chance.
Competing hypotheses
In every study, researchers put forth two kinds of hypotheses: the research or alternative hypothesis and the null hypothesis. The research hypothesis reflects what the researchers hope to show—that there is a difference between the experimental group and the control group. The null hypothesis directly competes with the research hypothesis. It states that there is no difference between the experimental group and the control group.
It may seem logical that researchers would test the research hypothesis—that is, that they would test what they hope to prove. But the probability theory requires that they test the null hypothesis instead. To support the research hypothesis, the data must contradict the null hypothesis. By demonstrating a difference between the two groups, the data contradict the null hypothesis.
Testing the null hypothesis
Now that you know why we test the null hypothesis, let’s look at how we test the null hypothesis.
After formulating the null and research hypotheses, researchers decide on a test statistic they can use to determine whether to accept or reject the null hypothesis. They also propose a fixed-level P value. The fixed level P value is often set at .05 and serves as the value against which the test-generated P value must be compared. (See Why .05?)
A comparison of the two P values determines whether the null hypothesis is rejected or accepted. If the P value associated with the test statistic is less than the fixed-level P value, the null hypothesis is rejected because there’s a statistically significant difference between the two groups. If the P value associated with the test statistic is greater than the fixed-level P value, the null hypothesis is accepted because there’s no statistically significant difference between the groups.
The decision to use .05 as the threshold in testing the null hypothesis is completely arbitrary. The researchers credited with establishing this threshold warned against strictly adhering to it.
Remember that warning when appraising a study in which the test statistic is greater than .05. The savvy reader will consider other important measurements, including effect size, confidence intervals, and power analyses when deciding whether to accept or reject scientific findings that could influence nursing practice.
Real-world hypothesis testing
How does this play out in real life? Let’s assume that you and a nurse colleague are conducting a study to find out if patients who receive backrubs fall asleep faster than patients who do not receive backrubs.
1. State your null and research hypotheses
Your null hypothesis will be that there will be no difference in the average amount of time it takes patients in each group to fall asleep. Your research hypothesis will be that patients who receive backrubs fall asleep, on average, faster than those who do not receive backrubs. You will be testing the null hypothesis in hopes of supporting your research hypothesis.
2. Propose a fixed-level P value
Although you can choose any value as your fixed-level P value, you and your research colleague decide you’ll stay with the conventional .05. If you were testing a new medical product or a new drug, you would choose a much smaller P value (perhaps as small as .0001). That’s because you would want to be as sure as possible that any difference you see between groups is attributed to the new product or drug and not to chance. A fixed-level P value of .0001 would mean that the difference between the groups was attributed to chance only 1 time out of 10,000. For a study on backrubs, however, .05 seems appropriate.
3. Conduct hypothesis testing to calculate a probability value
You and your research colleague agree that a randomized controlled study will help you best achieve your research goals, and you design the process accordingly. After consenting to participate in the study, patients are randomized to one of two groups:
- the experimental group that receives the intervention—the backrub group
- the control group—the non-backrub group.
After several nights of measuring the number of minutes it takes each participant to fall asleep, you and your research colleague find that on average, the backrub group takes 19 minutes to fall asleep and the non-backrub group takes 24 minutes to fall asleep.
Now the question is: Would you have the same results if you conducted the study using two different groups of people? That is, what role did chance play in helping the backrub group fall asleep 5 minutes faster than the non-backrub group? To answer this, you and your colleague will use an independent samples t-test to calculate a probability value.
An independent samples t-test is a kind of hypothesis test that compares the mean values of two groups (backrub and non-backrub) on a given variable (time to fall asleep).
Hypothesis testing is really nothing more than testing the null hypothesis. In this case, the null hypothesis is that the amount of time needed to fall asleep is the same for the experimental group and the control group. The hypothesis test addresses this question: If there’s really no difference between the groups, what is the probability of observing a difference of 5 minutes or more, say 10 minutes or 15 minutes?
We can define the P value as the probability that the observed time difference resulted from chance. Some find it easier to understand the P value when they think of it in relationship to error. In this case, the P value is defined as the probability of committing a Type 1 error. (Type 1 error occurs when a true null hypothesis is incorrectly rejected.)
4. Compare and interpret the P value
Early on in your study, you and your colleague selected a fixed-level P value of .05, meaning that you were willing to accept that 5% of the time, your results might be caused by chance. Also, you used an independent samples t-test to arrive at a probability value that will help you determine the role chance played in obtaining your results. Let’s assume, for the sake of this example, that the probability value generated by the independent samples t-test is .01 (P = .01). Because this P value associated with the test statistic is less than the fixed-level statistic (.01 < .05), you can reject the null hypothesis. By doing so, you declare that there is a statistically significant difference between the experimental and control groups. (See Putting the P value in context.)
In effect, you’re saying that the chance of observing a difference of 5 minutes or more, when in fact there is no difference, is less than 5 in 100. If the P value associated with the test statistic would have been greater than .05, then you would accept the null hypothesis, which would mean that there is no statistically significant difference between the control and experimental groups. Accepting the null hypothesis would mean that a difference of 5 minutes or more between the two groups would occur more than 5 times in 100.
Putting the P value in context
Although the P value helps you interpret study results, keep in mind that many factors can influence the P value—and your decision to accept or reject the null hypothesis. These factors include the following:
- Insufficient power. The study may not have been designed appropriately to detect an effect of the independent variable on the dependent variable. Therefore, a change may have occurred without your knowing it, causing you to incorrectly reject your hypothesis.
- Unreliable measures. Instruments that don’t meet consistency or reliability standards may have been used to measure a particular phenomenon.
- Threats to internal validity. Various biases, such as selection of patients, regression, history, and testing bias, may unduly influence study outcomes.
A decision to accept or reject study findings should focus not only on P value but also on other metrics including the following:
- Confidence intervals (an estimated range of values with a high probability of including the true population value of a given parameter)
- Effect size (a value that measures the magnitude of a treatment effect)
Remember, P value tells you only whether a difference exists between groups. It doesn’t tell you the magnitude of the difference.
5. Communicate your findings
The final step in hypothesis testing is communicating your findings. When sharing research findings (hypotheses) in writing or discussion, understand that they are statements of relationships or differences in populations. Your findings are not proved or disproved. Scientific findings are always subject to change. But each study leads to better understanding and, ideally, better outcomes for patients.
Key concepts
The P value isn’t the only concept you need to understand to analyze research findings. But it is a very important one. And chances are that understanding the P value will make it easier to understand other key analytical concepts.
Selected references
Burns N, Grove S: The Practice of Nursing Research: Conduct, Critique, and Utilization. 5th ed. Philadelphia: WB Saunders; 2004.
Glaser DN: The controversy of significance testing: misconceptions and alternatives. Am J Crit Care. 1999;8(5):291-296.
Kenneth J. Rempher, PhD, RN, MBA, CCRN, APRN,BC, is Director, Professional Nursing Practice at Sinai Hospital of Baltimore (Md.). Kathleen Urquico, BSN, RN, is a Direct Care Nurse in the Rubin Institute of Advanced Orthopedics at Sinai Hospital of Baltimore.

NurseLine Newsletter
- First Name *
- Last Name *
- Hidden Referrer
*By submitting your e-mail, you are opting in to receiving information from Healthcom Media and Affiliates. The details, including your email address/mobile number, may be used to keep you informed about future products and services.
Test Your Knowledge
Recent posts.

Interpreting statistical significance in nursing research

Introduction to qualitative nursing research

Navigating statistics for successful project implementation

Nurse research and the institutional review board

Research 101: Descriptive statistics

Research 101: Forest plots

Understanding confidence intervals helps you make better clinical decisions

Differentiating statistical significance and clinical significance

Differentiating research, evidence-based practice, and quality improvement

Are you confident about confidence intervals?

Making sense of statistical power
Nursing Theories & Theorists Explained
What is nursing theory.
- Nursing Theory Users
- Metaparadigms
Nursing Theorists
Nursing theory in practice.

Nursing theory is "a creative and rigorous structuring of ideas that project a tentative, purposeful, and systematic view of phenomena," per the book Integrated Theory and Knowledge Development in Nursing.
Nursing theory provides the foundational knowledge that enables nurses to care for their patients and guides their actions. Theories are in place, regardless of nursing specialization, to establish guidelines for both broad and specific nursing practices.
Nursing theory is heavily influenced by Florence Nightingale's pioneering work, which significantly influenced the modern nursing definition . Nightingale's Environmental Theory stated that nursing “ought to signify the proper use of fresh air, light, warmth, cleanliness, quiet, and the proper selection and administration of diet – all at the least expense of vital power to the patient.”
Find Nursing Programs
By identifying potential risk factors for illness or conditions that would exacerbate an illness and potentially lead to death, Nightingale saw the importance of a patient’s environment to their overall health and well-being. As a result, healthcare professionals, including nurses, began to treat patients differently and the start of population health and public health is seen.
In Florence Nightingale’s Environmental Theory, she identified five environmental factors:
- Efficient drainage
- Cleanliness or sanitation
- Light or direct sunlight
These factors were essential to decrease the spread of contagious diseases and decreasing mortality and morbidity.
While Florence Nightingale may have introduced the first nursing theory in 1860, it is still extremely relevant today. In countries where fresh air, pure water, efficient drainage, cleanliness or sanitation, and light or direct sunlight are not present, morbidity and mortality are increased.
What are Nursing Theories Used For?
Nursing theories provide the foundation for nursing practice and are essential to the care of patients. Academic hospitals and Magnet hospitals will consistently ensure that nursing theories are incorporated into their policies and procedures to ensure best practice is being used.
Most nurses and institutions will employ a variety of nursing theories within their everyday practice versus just one theory. Most do it unknowingly.
Nursing theories help bedside nurses evaluate patient care and base nursing interventions on the evaluation of the findings.
The theories can also provide nurses with the rationale to make certain decisions. An example of a nursing theory in use is seen in the care of a Jehovah’s Witnesses patient that does not believe in blood transfusions. While the patient may need a blood transfusion, Dorothea Orem’s Self-Care theory provides nurses with a solid basis for assisting their patients and giving them the opportunity to express independence and control in caring for themselves. While the nurse may not agree with the patient’s decision to not receive a blood transfusion, Orem’s theory suggests the importance of allowing the patient to make the decision and respecting it as their own choice.
Oftentimes, the integration of nursing theory is not as obvious as in the aforementioned example. However, it is important for nurses and nursing students to understand and respect the importance of nursing theories and their impact on modern-day nursing and healthcare.
Popular Online Master of Science in Nursing (MSN) Programs

GCU's College of Nursing and Health Care Professions has a nearly 35-year tradition of preparing students to fill evolving healthcare roles as highly qualified professionals. GCU offers a full spectrum of nursing degrees, from a pre-licensure BSN degree to a Doctor of Nursing Practice (DNP) program.
Enrollment: Nationwide
- MSN - Family NP
- MSN - Adult Gerontology Acute Care NP
- MSN - Nursing Education
- MSN - Health Informatics
- MSN - Public Health Nursing
- MSN - Health Care Quality & Patient Safety
- MBA & MSN - Nursing Leadership in Health Care Systems
- See more GCU nursing programs

At Purdue Global, discover a faster, more affordable way to earn your Nursing degree. Purdue Global is committed to keeping your tuition costs as low as possible and helping you find the most efficient path to your degree.
Enrollment: Nationwide, but certain programs have state restrictions. Check with Purdue for details.
- Accelerated BSN-to-MSN
- MSN - Adult-Gerontology Acute Care NP
- MSN - Psychiatric Mental Health NP
- MSN - Nurse Educator
- MSN - Executive Leader
- MSN - Nurse Informatics
- MSN/MBA Dual Degree
- See more Purdue nursing programs
Capella’s online RN-to-BSN degree is an accredited program designed for working nurses. Thousands of nurses have completed their BSN program with FlexPath, that allows you to control your pace and set your own deadlines. With FlexPath, you can complete your RN-to-BSN program in 9 months and under $10,000. Fastest 25% of students. Cost varies by pace, transfer credits, other factors. Fees apply.
Enrollment: Nationwide, but certain programs have state restrictions. Check with Capella for details.
- MSN - Adult-Gerontology Primary Care NP
- MSN - Nursing Informatics
- MSN - Care Coordination
- MSN - Nursing Leadership & Admin
- See more Capella nursing programs

WGU's award-winning online programs are created to help you succeed while graduating faster and with less debt. WGU is a CCNE accredited, nonprofit university offering nursing bachelor's and master's degrees.
- BSN-to-MSN - Nursing Education
- RN-to-MSN - Nursing Education
- BSN-to-MSN - Family NP
- BSN-to-MSN - Psychiatric Mental Health NP
- RN-to-MSN - Nursing Leadership & Management
- See more WGU nursing programs

Who are Nursing Theories Used By?
While all nurses, regardless of position and specialty, utilize nursing theories in their practice, not all nurses are aware of their implications. Generally speaking, most nursing theories are used by nurse educators and nurse researchers.
Nurse educators will utilize nursing theories in designing course curriculums based on educational principles, research, and theories to provide nursing students with the knowledge and skills needed to provide care to their patients.
Nurse researchers will conduct theory-guided research in order to create best practices and to predict potential clinical problems or explain existing knowledge.
Nursing Metaparadigms
There have been countless nursing theories introduced since Florence Nightingale's Environmental Theory, including Imogene King‘s Theory of Goal and Dorothy Johnson’s Behavioral System Model. What they all have in common is they center around the nursing metaparadigm.
A metaparadigm is a set of theories or ideas that provide structure for how a discipline should function. Nursing metaparadigms were first classified by Fawcett into four specific categories,
- Environment
These four concepts are fundamental to all nursing theories and without identification of them and their relevance to the theory, it is incomplete.
Furthermore, these four basic nursing metaparadigms point to the holistic care of a patient and their medical health is interconnected to the four concepts.
>> Show Me Online Nursing Programs
The Four Main Concepts of Nursing Theory
Fawcett’s four specific concepts help define nursing and set it apart from other disciplines and professions. These four concepts have been used to define the context and content of the nursing profession. The person is the most important concept in nursing theory, but each theorist's interpretation of the other concepts is how to differentiate between them.
Person (also referred to as Client or Human Being) is the recipient of nursing care and may include individuals, patients, groups, families, and communities.
2. Environment
Environment or situation is defined as the internal and external surroundings that affect the patient. It includes all positive or negative conditions that affect the patient, the physical environment, such as families, friends, and significant others, and the setting for where they go for their healthcare.
Health is defined as the degree of wellness or well-being that the client experiences. It may have different meanings for each patient, the clinical setting, and the health care provider.
The attributes, characteristics, and actions of the nurse providing care on behalf of or in conjunction with, the client.
Levels of Nursing Theory
Nursing theories are categorized into three levels including,
- Grand Nursing Theories
- Mid-range Nursing Theories
- Nursing Practice Theories
Grand Nursing Theories
These are theories based on broad, abstract, and complex concepts. They provide the general framework for nursing ideas pertaining to components such as people and health. These theories typically stem from a nurse theorist’s own experience.
Mid-Range Nursing Theories
These are theories that drill down into specific areas of nursing rather than deal with sweeping concepts. They can emerge from nursing practice, research, or from the theories of similar disciplines.
Nursing Practice Theories
These are theories that narrow their focus even further, specifically focusing on concepts concerning a defined patient population. These theories tend to directly affect patients more than the other two types of theories. Bedside nurses will often use these theories in their everyday practice.
We talked about Nightingale and Orems' role as nursing theorists and reviewed their respective theories. Let's explore the work of some other notable nursing theorists and how their work helps nurses and other healthcare providers give better patient care.
Virginia Henderson: Nursing Need Theory
Virginia Henderson's Nursing Need Theory centers around the concept of basic human needs. Henderson believed that the role of a nurse is to assist individuals in meeting their fundamental needs and help them increase their independence.
Her theory emphasizes the nurse's role in supporting patients in activities such as:
Maintaining desired postures
Dress and undress
Cleanliness
Communicating fears, opinions, and needs, and
Worshiping according to their faith
Jean Watson: Theory of Human Caring
Jean Watson is a contemporary nursing theorist renowned for her Theory of Human Caring . Watson emphasizes the importance of creating a caring and compassionate relationship between the nurse and the patient.
Her theory focuses on ten factors:
Upholding humanistic-altruistic values by practicing kindness and compassion
Being genuinely present and fostering faith, hope, and belief systems while respecting the subjective experiences of oneself and others
Cultivating self-awareness and spiritual practices, transcending ego-centeredness to achieve a transpersonal presence.
Developing and nurturing loving, trusting, and caring relationships
Encouraging the expression of both positive and negative emotions, actively listening to others' stories without judgment
Applying creative problem-solving through the caring-healing process
Engaging in transpersonal teaching and learning within a caring relationship, adapting to the individual's perspective and transitioning towards a coaching approach for enhanced health
Creating a healing environment on various levels, fostering an atmosphere of authentic caring presence at an energetic and subtle level.
Acknowledging the interconnectedness of mind, body, and spirit while upholding human dignity
Embracing the spiritual, mysterious, and unknown aspects of life
Madeleine Leininger: Transcultural Nursing Theory
Leininger's Transcultural Nursing Theory , also called Culture Care Theory, focuses on providing culturally congruent care by understanding and respecting the values, beliefs, and practices of diverse individuals and groups.
Hildegard Peplau: Interpersonal Relations Theory
Peplau's Interpersonal Theory of Interpersonal Relations emphasizes that the journey of nurse-patient relationships involves three pivotal stages that are essential for their success:
The initial orientation
A dynamic working phase, and
A thoughtful termination process
According to Peplau, the nurse's role is to facilitate the patient's growth and development by utilizing therapeutic communication, empathy, and understanding.
Betty Neuman: Neuman Systems Model
The Neuman Systems Model focuses on identifying stressors that have the potential to negatively impact an individual's health and overall well-being. It incorporates various factors such as physiological, psychological, sociocultural, and developmental aspects.
The theory also provides a flexible structure for assessment, intervention, and evaluation in nursing practice.
Sister Callista Roy: Adaptation Model
The Roy Adaptation Model is based on the belief that individuals are adaptive systems, constantly interacting with their environment to maintain their physiological and psychosocial integrity. It views the person as a holistic being, consisting of four interconnected adaptive modes:
Physiological Mode: Deals with physical and biological aspects of adaptation, including the body's response to stressors, maintaining homeostasis, and meeting basic physiological needs.
Self-Concept Mode: Focuses on individuals' perception of themselves, including self-esteem and self-image.
Role Function Mode: Considers the roles people have in their lives, such as spouse, parent, employee, or student.
Interdependence Mode: Emphasizes the importance of social relationships and how individuals interact with others, such as support from social networks.
Martha Rogers: Science of Unitary Human Being
Rogers' Science of Unitary Human Beings believed that nursing should focus on promoting harmony and balance within the individual and their environment.
Her theory emphasizes the interconnectedness of human beings with their surroundings and the importance of energy fields in health and healing. Spoken another way, patients cannot be considered as “separate” from their environment.
Patricia Benner: Novice to Expert Theory
Benner's Novice to Expert Theory describes the stages of nursing skill from novice to advanced beginner, and finally, to competent.
She emphasizes the importance of practical experience and clinical judgment in nursing practice and highlights that expertise develops over time through practice and reflection.
Imogene King: Theory of Goal Attainment
King's Theory of Goal Attainment focuses on the nurse-patient relationship and the mutual goal-setting process. Her theory emphasizes that nurses and patients should collaborate to establish goals that promote the patient's well-being and health.
Katharine Kolcaba: Comfort Theory
Kolcaba's Comfort Theory highlights the significance of providing comfort to patients as a central goal of nursing care.
Her theory defines comfort as the immediate experience of being strengthened in physical, psychospiritual, environmental, and sociocultural dimensions.
Kolcalba’s framework proposes that healthcare providers:
Assess if patient’s comfort needs are not being met
Create interventions to meet those needs
Measure comfort prior to and after the interventions
Nursing theories are used every day in practice even if nurses aren’t aware of their use. Theories help guide evidence-based research which then leads to best practices and policies. These policies and procedures keep patients safe, while providing the best care possible.
Nursing theories also allow nurses to positively influence the health and well-being of their patients beyond taking care of them at the bedside. Nursing theory-guided practice helps improve the quality of care delivered and helps continue to move the nursing profession forward into the 21st century.
Most bedside nurses will not necessarily know the theories behind their practice so their usefulness is often dismissed. Advanced practice nurses, nurse scholars, nurse educators, and nurse researchers are most likely going to be up to date on current nursing theories and their impact on the nursing profession.
Nursing theories should continue to guide nursing practice both in academia and at the bedside. It allows nurses to provide current best-practice care to their patients while also impacting them beyond the bedside. Florence Nightingale’s Environmental Theory was groundbreaking during the 1860s and helped change the course of nursing and healthcare while changing the outcomes of patients through the identification of environmental factors that may hinder their health and well-being.
Nursing Theory FAQs
What are the major nursing theories .
- All nursing theories encompass person, environment, health, and the nurse and are categorized into three hierarchies: grand nursing theories, middle-range nursing theories, and practice level nursing theories.
What are examples of nursing theory?
- Some examples of nursing theories include the Environmental Theory, the Casey Model of Nursing, the Martha Rogers Theory, the Tidal Model, and the Cultural Care Theory.
What is the Casey model of nursing?
- The Casey Model of Nursing is a model of nursing designed to encompass the child-health relationship with five focuses: child, family, health, environment, and the nurse.
What is Martha Roger's Theory?
- The Martha Rogers Theory of nursing looks at people as “unitary” human beings that can’t be divided into parts and nursing as a blend of both art and science.
What is a partnership model in nursing?
- It’s a patient and family-centered care system that focuses on partnership between the two, along with education, support, communication, and collaborative practice.
What are the principles of the tidal model?
- The tidal model of nursing has 6 principles: curiosity, virtue, mystery investigation, respect of the person, crisis as an opportunity, possessing goals, and pursuit of elegance.

Kathleen Gaines (nee Colduvell) is a nationally published writer turned Pediatric ICU nurse from Philadelphia with over 13 years of ICU experience. She has an extensive ICU background having formerly worked in the CICU and NICU at several major hospitals in the Philadelphia region. After earning her MSN in Education from Loyola University of New Orleans, she currently also teaches for several prominent Universities making sure the next generation is ready for the bedside. As a certified breastfeeding counselor and trauma certified nurse, she is always ready for the next nursing challenge.

Plus, get exclusive access to discounts for nurses, stay informed on the latest nurse news, and learn how to take the next steps in your career.
By clicking “Join Now”, you agree to receive email newsletters and special offers from Nurse.org. We will not sell or distribute your email address to any third party, and you may unsubscribe at any time by using the unsubscribe link, found at the bottom of every email.
Nursing Theories and Theorists: The Definitive Guide for Nurses

In this guide for nursing theories and nursing theorists , we aim to help you understand what comprises a nursing theory and its importance, purpose, history, types, or classifications, and give you an overview through summaries of selected nursing theories.
Table of Contents
- What are Nursing Theories?
Defining Terms
History of nursing theories, environment, definitions, relational statements, assumptions, why are nursing theories important, in academic discipline, in research, in the profession, grand nursing theories, middle-range nursing theories, practice-level nursing theories, factor-isolating theory, explanatory theory, prescriptive theories, other ways of classifying nursing theories, florence nightingale, hildegard e. peplau, virginia henderson, faye glenn abdellah, ernestine wiedenbach, lydia e. hall, joyce travelbee, kathryn e. barnard, evelyn adam, nancy roper, winifred logan, and alison j. tierney, ida jean orlando, jean watson.
- Marilyn Anne Ray
Patricia Benner
Kari martinsen, katie eriksson, myra estrin levine, martha e. rogers, dorothea e. orem, imogene m. king, betty neuman, sister callista roy, dorothy e. johnson, anne boykin and savina o. schoenhofer, afaf ibrahim meleis, nola j. pender, madeleine m. leininger, margaret a. newman, rosemarie rizzo parse, helen c. erickson, evelyn m. tomlin, and mary ann p. swain, gladys l. husted and james h. husted, ramona t. mercer, merle h. mishel, pamela g. reed, carolyn l. wiener and marylin j. dodd, georgene gaskill eakes, mary lermann burke, and margaret a. hainsworth, phil barker, katharine kolcaba, cheryl tatano beck, kristen m. swanson, cornelia m. ruland and shirley m. moore, wanda de aguiar horta, recommended resources, what are nursing theories.
Nursing theories are organized bodies of knowledge to define what nursing is, what nurses do, and why they do it. Nursing theories provide a way to define nursing as a unique discipline that is separate from other disciplines (e.g., medicine). It is a framework of concepts and purposes intended to guide nursing practice at a more concrete and specific level.
Nursing, as a profession, is committed to recognizing its own unparalleled body of knowledge vital to nursing practice—nursing science. To distinguish this foundation of knowledge, nurses need to identify, develop, and understand concepts and theories in line with nursing. As a science, nursing is based on the theory of what nursing is, what nurses do, and why. Nursing is a unique discipline and is separate from medicine. It has its own body of knowledge on which delivery of care is based.
The development of nursing theory demands an understanding of selected terminologies, definitions, and assumptions.
- Philosophy. These are beliefs and values that define a way of thinking and are generally known and understood by a group or discipline.
- Theory . A belief, policy, or procedure proposed or followed as the basis of action. It refers to a logical group of general propositions used as principles of explanation. Theories are also used to describe, predict, or control phenomena.
- Concept. Concepts are often called the building blocks of theories. They are primarily the vehicles of thought that involve images.
- Models. Models are representations of the interaction among and between the concepts showing patterns. They present an overview of the theory’s thinking and may demonstrate how theory can be introduced into practice.
- Conceptual framework. A conceptual framework is a group of related ideas, statements, or concepts. It is often used interchangeably with the conceptual model and with grand theories .
- Proposition. Propositions are statements that describe the relationship between the concepts.
- Domain . The domain is the perspective or territory of a profession or discipline.
- Process. Processes are organized steps, changes, or functions intended to bring about the desired result.
- Paradigm. A paradigm refers to a pattern of shared understanding and assumptions about reality and the world, worldview, or widely accepted value system.
- Metaparadigm. A metaparadigm is the most general statement of discipline and functions as a framework in which the more restricted structures of conceptual models develop. Much of the theoretical work in nursing focused on articulating relationships among four major concepts: person, environment, health, and nursing.
The first nursing theories appeared in the late 1800s when a strong emphasis was placed on nursing education.
- In 1860, Florence Nightingale defined nursing in her “ Environmental Theory ” as “the act of utilizing the patient’s environment to assist him in his recovery.”
- In the 1950s, there is a consensus among nursing scholars that nursing needed to validate itself through the production of its own scientifically tested body of knowledge.
- In 1952, Hildegard Peplau introduced her Theory of Interpersonal Relations that emphasizes the nurse -client relationship as the foundation of nursing practice.
- In 1955, Virginia Henderson conceptualized the nurse’s role as assisting sick or healthy individuals to gain independence in meeting 14 fundamental needs. Thus her Nursing Need Theory was developed.
- In 1960, Faye Abdellah published her work “Typology of 21 Nursing Problems,” which shifted the focus of nursing from a disease-centered approach to a patient-centered approach.
- In 1962, Ida Jean Orlando emphasized the reciprocal relationship between patient and nurse and viewed nursing’s professional function as finding out and meeting the patient’s immediate need for help.
- In 1968, Dorothy Johnson pioneered the Behavioral System Model and upheld the fostering of efficient and effective behavioral functioning in the patient to prevent illness.
- In 1970, Martha Rogers viewed nursing as both a science and an art as it provides a way to view the unitary human being, who is integral with the universe.
- In 1971, Dorothea Orem stated in her theory that nursing care is required if the client is unable to fulfill biological, psychological, developmental, or social needs.
- In 1971, Imogene King ‘s Theory of Goal attainment stated that the nurse is considered part of the patient’s environment and the nurse-patient relationship is for meeting goals towards good health.
- In 1972, Betty Neuman , in her theory, states that many needs exist, and each may disrupt client balance or stability. Stress reduction is the goal of the system model of nursing practice.
- In 1979, Sr. Callista Roy viewed the individual as a set of interrelated systems that maintain the balance between these various stimuli.
- In 1979, Jean Watson developed the philosophy of caring, highlighted humanistic aspects of nursing as they intertwine with scientific knowledge and nursing practice.
The Nursing Metaparadigm
Four major concepts are frequently interrelated and fundamental to nursing theory: person, environment, health, and nursing. These four are collectively referred to as metaparadigm for nursing .

Person (also referred to as Client or Human Beings) is the recipient of nursing care and may include individuals, patients, groups, families, and communities.
Environment (or situation) is defined as the internal and external surroundings that affect the client. It includes all positive or negative conditions that affect the patient, the physical environment, such as families, friends, and significant others, and the setting for where they go for their healthcare.
Health is defined as the degree of wellness or well-being that the client experiences. It may have different meanings for each patient, the clinical setting, and the health care provider.
The nurse’s attributes, characteristics, and actions provide care on behalf of or in conjunction with the client. There are numerous definitions of nursing, though nursing scholars may have difficulty agreeing on its exact definition. The ultimate goal of nursing theories is to improve patient care .
You’ll find that these four concepts are used frequently and defined differently throughout different nursing theories. Each nurse theorist’s definition varies by their orientation, nursing experience , and different factors that affect the theorist’s nursing view. The person is the main focus, but how each theorist defines the nursing metaparadigm gives a unique take specific to a particular theory. To give you an example, below are the different definitions of various theorists on the nursing metaparadigm:

Components of Nursing Theories
For a theory to be a theory, it has to contain concepts, definitions, relational statements, and assumptions that explain a phenomenon. It should also explain how these components relate to each other.
A term given to describe an idea or response about an event, a situation, a process, a group of events, or a group of situations. Phenomena may be temporary or permanent. Nursing theories focus on the phenomena of nursing.
Interrelated concepts define a theory. Concepts are used to help describe or label a phenomenon. They are words or phrases that identify, define, and establish structure and boundaries for ideas generated about a particular phenomenon. Concepts may be abstract or concrete.
- Abstract Concepts . Defined as mentally constructed independently of a specific time or place.
- Concrete Concepts . Are directly experienced and related to a particular time or place.
Definitions are used to convey the general meaning of the concepts of the theory. Definitions can be theoretical or operational.
- Theoretical Definitions . Define a particular concept based on the theorist’s perspective.
- Operational Definitions . States how concepts are measured.
Relational statements define the relationships between two or more concepts. They are the chains that link concepts to one another.
Assumptions are accepted as truths and are based on values and beliefs. These statements explain the nature of concepts, definitions, purpose, relationships, and structure of a theory.
Nursing theories are the basis of nursing practice today. In many cases, nursing theory guides knowledge development and directs education, research, and practice. Historically, nursing was not recognized as an academic discipline or as a profession we view today. Before nursing theories were developed, nursing was considered to be a task-oriented occupation. The training and function of nurses were under the direction and control of the medical profession. Let’s take a look at the importance of nursing theory and its significance to nursing practice:
- Nursing theories help recognize what should set the foundation of practice by explicitly describing nursing.
- By defining nursing, a nursing theory also helps nurses understand their purpose and role in the healthcare setting.
- Theories serve as a rationale or scientific reasons for nursing interventions and give nurses the knowledge base necessary for acting and responding appropriately in nursing care situations.
- Nursing theories provide the foundations of nursing practice, generate further knowledge, and indicate which direction nursing should develop in the future (Brown, 1964).
- By providing nurses a sense of identity, nursing theory can help patients, managers, and other healthcare professionals to acknowledge and understand the unique contribution that nurses make to the healthcare service (Draper, 1990).
- Nursing theories prepare the nurses to reflect on the assumptions and question the nursing values, thus further defining nursing and increasing the knowledge base.
- Nursing theories aim to define, predict, and demonstrate nursing phenomenon (Chinn and Jacobs, 1978).
- It can be regarded as an attempt by the nursing profession to maintain and preserve its professional limits and boundaries.
- Nursing theories can help guide research and informing evidence-based practice.
- Provide a common language and terminology for nurses to use in communication and practice.
- Serves as a basis for the development of nursing education and training programs.
- In many cases, nursing theories guide knowledge development and directs education, research, and practice, although each influences the others. (Fitzpatrick and Whall, 2005).
Purposes of Nursing Theories
The primary purpose of theory in nursing is to improve practice by positively influencing the health and quality of life of patients. Nursing theories are essential for the development and advancement of the nursing profession. Nursing theories are also developed to define and describe nursing care, guide nursing practice, and provide a basis for clinical decision-making . In the past, the accomplishments of nursing led to the recognition of nursing in an academic discipline, research, and profession.
Much of the earlier nursing programs identified the major concepts in one or two nursing models, organized the concepts, and build an entire nursing curriculum around the created framework. These models’ unique language was typically introduced into program objectives, course objectives, course descriptions, and clinical performance criteria. The purpose was to explain the fundamental implications of the profession and enhance the profession’s status.
The development of theory is fundamental to the research process, where it is necessary to use theory as a framework to provide perspective and guidance to the research study. Theory can also be used to guide the research process by creating and testing phenomena of interest. To improve the nursing profession’s ability to meet societal duties and responsibilities, there needs to be a continuous reciprocal and cyclical connection with theory, practice, and research. This will help connect the perceived “gap” between theory and practice and promote the theory-guided practice.
Clinical practice generates research questions and knowledge for theory. In a clinical setting, its primary contribution has been the facilitation of reflecting, questioning, and thinking about what nurses do. Because nurses and nursing practice are often subordinate to powerful institutional forces and traditions, introducing any framework that encourages nurses to reflect on, question, and think about what they do provide an invaluable service.
Classification of Nursing Theories
There are different ways to categorize nursing theories. They are classified depending on their function, levels of abstraction, or goal orientation.
By Abstraction
There are three major categories when classifying nursing theories based on their level of abstraction: grand theory, middle-range theory, and practice-level theory.

- Grand theories are abstract, broad in scope, and complex, therefore requiring further research for clarification.
- Grand nursing theories do not guide specific nursing interventions but rather provide a general framework and nursing ideas.
- Grand nursing theorists develop their works based on their own experiences and their time, explaining why there is so much variation among theories.
- Address the nursing metaparadigm components of person, nursing, health, and environment.
- More limited in scope (compared to grand theories) and present concepts and propositions at a lower level of abstraction. They address a specific phenomenon in nursing.
- Due to the difficulty of testing grand theories, nursing scholars proposed using this level of theory.
- Most middle-range theories are based on a grand theorist’s works, but they can be conceived from research, nursing practice, or the theories of other disciplines.
- Practice nursing theories are situation-specific theories that are narrow in scope and focuses on a specific patient population at a specific time.
- Practice-level nursing theories provide frameworks for nursing interventions and suggest outcomes or the effect of nursing practice.
- Theories developed at this level have a more direct effect on nursing practice than more abstract theories.
- These theories are interrelated with concepts from middle-range theories or grand theories.
By Goal Orientation
Theories can also be classified based on their goals. They can be descriptive or prescriptive .
Descriptive Theories
- Descriptive theories are the first level of theory development. They describe the phenomena and identify its properties and components in which it occurs.
- Descriptive theories are not action-oriented or attempt to produce or change a situation.
- There are two types of descriptive theories: factor-isolating theory and explanatory theory .
- Also known as category-formulating or labeling theory.
- Theories under this category describe the properties and dimensions of phenomena.
- Explanatory theories describe and explain the nature of relationships of certain phenomena to other phenomena.
- Address the nursing interventions for a phenomenon, guide practice change, and predict consequences.
- Includes propositions that call for change.
- In nursing, prescriptive theories are used to anticipate the outcomes of nursing interventions.
Classification According to Meleis
Afaf Ibrahim Meleis (2011), in her book Theoretical Nursing: Development and Progress , organizes the major nurse theories and models using the following headings: needs theories, interaction theories, and outcome theories. These categories indicate the basic philosophical underpinnings of the theories.
- Needs-Based Theories. The needs theorists were the first group of nurses who thought of giving nursing care a conceptual order. Theories under this group are based on helping individuals to fulfill their physical and mental needs. Theories of Orem, Henderson, and Abdella are categorized under this group. Need theories are criticized for relying too much on the medical model of health and placing the patient in an overtly dependent position.
- Interaction Theories. These theories emphasized nursing on the establishment and maintenance of relationships. They highlighted the impact of nursing on patients and how they interact with the environment, people, and situations. Theories of King, Orlando, and Travelbee are grouped under this category.
- Outcome Theories . These theories describe the nurse as controlling and directing patient care using their knowledge of the human physiological and behavioral systems. The nursing theories of Johnson , Levine , Rogers , and Roy belong to this group.
Classification According to Alligood
In her book, Nursing Theorists and Their Work, Raile Alligood (2017) categorized nursing theories into four headings: nursing philosophy, nursing conceptual models, nursing theories and grand theories, and middle-range nursing theories.
- Nursing Philosophy . It is the most abstract type and sets forth the meaning of nursing phenomena through analysis, reasoning, and logical presentation. Works of Nightingale, Watson, Ray, and Benner are categorized under this group.
- Nursing Conceptual Models . These are comprehensive nursing theories that are regarded by some as pioneers in nursing. These theories address the nursing metaparadigm and explain the relationship between them. Conceptual models of Levine, Rogers, Roy, King, and Orem are under this group.
- Grand Nursing Theories. Are works derived from nursing philosophies, conceptual models, and other grand theories that are generally not as specific as middle-range theories. Works of Levine, Rogers, Orem, and King are some of the theories under this category.
- Middle-Range Theories. Are precise and answer specific nursing practice questions . They address the specifics of nursing situations within the model’s perspective or theory from which they are derived. Examples of Middle-Range theories are that of Mercer, Reed, Mishel, and Barker.
List of Nursing Theories and Theorists
You’ve learned from the previous sections the definition of nursing theory, its significance in nursing, and its purpose in generating a nursing knowledge base. This section will give you an overview and summary of the various published works in nursing theory (in chronological order). Deep dive into learning about the theory by clicking on the links provided for their biography and comprehensive review of their work.
See Also: Florence Nightingale: Environmental Theory and Biography
- Founder of Modern Nursing and Pioneer of the Environmental Theory.
- Defined Nursing as “the act of utilizing the environment of the patient to assist him in his recovery.”
- Stated that nursing “ought to signify the proper use of fresh air, light, warmth, cleanliness, quiet, and the proper selection and administration of diet – all at the least expense of vital power to the patient.”
- Identified five (5) environmental factors: fresh air, pure water, efficient drainage, cleanliness or sanitation, and light or direct sunlight.
See Also: Hildegard Peplau: Interpersonal Relations Theory
- Pioneered the Theory of Interpersonal Relations
- Peplau’s theory defined Nursing as “An interpersonal process of therapeutic interactions between an individual who is sick or in need of health services and a nurse specially educated to recognize, respond to the need for help.”
- Her work is influenced by Henry Stack Sullivan, Percival Symonds, Abraham Maslow , and Neal Elgar Miller.
- It helps nurses and healthcare providers develop more therapeutic interventions in the clinical setting.
See Also: Virginia Henderson: Nursing Need Theory
- Developed the Nursing Need Theory
- Focuses on the importance of increasing the patient’s independence to hasten their progress in the hospital.
- Emphasizes the basic human needs and how nurses can assist in meeting those needs.
- “The nurse is expected to carry out a physician’s therapeutic plan, but individualized care is the result of the nurse’s creativity in planning for care.”
See Also: Faye Glenn Abdellah: 21 Nursing Problems Theory
- Developed the 21 Nursing Problems Theory
- “Nursing is based on an art and science that molds the attitudes, intellectual competencies, and technical skills of the individual nurse into the desire and ability to help people, sick or well, cope with their health needs.”
- Changed the focus of nursing from disease-centered to patient-centered and began to include families and the elderly in nursing care.
- The nursing model is intended to guide care in hospital institutions but can also be applied to community health nursing, as well.
- Developed The Helping Art of Clinical Nursing conceptual model.
- Definition of nursing reflects on nurse-midwife experience as “People may differ in their concept of nursing, but few would disagree that nursing is nurturing or caring for someone in a motherly fashion.”
- Guides the nurse action in the art of nursing and specified four elements of clinical nursing: philosophy, purpose, practice, and art.
- Clinical nursing is focused on meeting the patient’s perceived need for help in a vision of nursing that indicates considerable importance on the art of nursing.
See Also: Lydia Hall: Care, Cure, Core Theory
- Developed the Care, Cure, Core Theory is also known as the “ Three Cs of Lydia Hall . “
- Hall defined Nursing as the “participation in care, core and cure aspects of patient care , where CARE is the sole function of nurses, whereas the CORE and CURE are shared with other members of the health team.”
- The major purpose of care is to achieve an interpersonal relationship with the individual to facilitate the development of the core.
- The “care” circle defines a professional nurse’s primary role, such as providing bodily care for the patient. The “core” is the patient receiving nursing care. The “cure” is the aspect of nursing that involves the administration of medications and treatments.
- States in her Human-to-Human Relationship Model that the purpose of nursing was to help and support an individual, family, or community to prevent or cope with the struggles of illness and suffering and, if necessary, to find significance in these occurrences, with the ultimate goal being the presence of hope.
- Nursing was accomplished through human-to-human relationships.
- Extended the interpersonal relationship theories of Peplau and Orlando.
- Developed the Child Health Assessment Model .
- Concerns improving the health of infants and their families.
- Her findings on parent-child interaction as an important predictor of cognitive development helped shape public policy.
- She is the founder of the Nursing Child Assessment Satellite Training Project (NCAST), which produces and develops research-based products, assessment , and training programs to teach professionals, parents, and other caregivers the skills to provide nurturing environments for young children.
- Borrows from psychology and human development and focuses on mother-infant interaction with the environment.
- Contributed a close link to practice that has modified the way health care providers assess children in light of the parent-child relationship.
- Focuses on the development of models and theories on the concept of nursing.
- Includes the profession’s goal, the beneficiary of the professional service, the role of the professional, the source of the beneficiary’s difficulty, the intervention of the professional, and the consequences.
- A good example of using a unique basis of nursing for further expansion.
- A Model for Nursing Based on a Model of Living
- Logan produced a simple theory, “which actually helped bedside nurses.”
- The trio collaborated in the fourth edition of The Elements of Nursing: A Model for Nursing Based on a Model of Living and prepared a monograph entitled The Roper-Logan-Tierney Model of Nursing: Based on Activities of Daily Living.
- Includes maintaining a safe environment, communicating, breathing, eating and drinking, eliminating, personal cleansing and dressing , controlling body temperature, mobilizing, working and playing, expressing sexuality, sleeping , and dying .
See Also: Ida Jean Orlando: Nursing Process Theory
- She developed the Nursing Process Theory.
- “Patients have their own meanings and interpretations of situations, and therefore nurses must validate their inferences and analyses with patients before drawing conclusions.”
- Allows nurses to formulate an effective nursing care plan that can also be easily adapted when and if any complexity comes up with the patient.
- According to her, persons become patients requiring nursing care when they have needs for help that cannot be met independently because of their physical limitations, negative reactions to an environment, or experience that prevents them from communicating their needs.
- The role of the nurse is to find out and meet the patient’s immediate needs for help.
See Also: Jean Watson: Theory of Human Caring
- She pioneered the Philosophy and Theory of Transpersonal Caring .
- “Nursing is concerned with promoting health, preventing illness, caring for the sick, and restoring health.”
- Mainly concerns with how nurses care for their patients and how that caring progresses into better plans to promote health and wellness, prevent illness and restore health.
- Focuses on health promotion , as well as the treatment of diseases.
- Caring is central to nursing practice and promotes health better than a simple medical cure.
Marilyn Anne Ray
- Developed the Theory of Bureaucratic Caring
- “Improved patient safety , infection control, reduction in medication errors , and overall quality of care in complex bureaucratic health care systems cannot occur without knowledge and understanding of complex organizations, such as the political and economic systems, and spiritual-ethical caring, compassion and right action for all patients and professionals.”
- Challenges participants in nursing to think beyond their usual frame of reference and envision the world holistically while considering the universe as a hologram.
- Presents a different view of how health care organizations and nursing phenomena interrelate as wholes and parts in the system.
- Caring, Clinical Wisdom, and Ethics in Nursing Practice
- “The nurse-patient relationship is not a uniform, professionalized blueprint but rather a kaleidoscope of intimacy and distance in some of the most dramatic, poignant, and mundane moments of life.”
- Attempts to assert and reestablish nurses’ caring practices when nurses are rewarded more for efficiency, technical skills, and measurable outcomes.
- States that caring practices are instilled with knowledge and skill regarding everyday human needs.
- Philosophy of Caring
- “Nursing is founded on caring for life, on neighborly love, […]At the same time, the nurse must be professionally educated.”
- Human beings are created and are beings for whom we may have administrative responsibility.
- Caring, solidarity, and moral practice are unavoidable realities.
- Theory of Carative Caring
- “Caritative nursing means that we take ‘caritas’ into use when caring for the human being in health and suffering […] Caritative caring is a manifestation of the love that ‘just exists’ […] Caring communion, true caring, occurs when the one caring in a spirit of caritas alleviates the suffering of the patient.”
- The ultimate goal of caring is to lighten suffering and serve life and health.
- Inspired many in the Nordic countries and used it as the basis of research, education, and clinical practice.
See Also: Myra Estrin Levine: Conservation Model for Nursing
- According to the Conservation Model , “Nursing is human interaction.”
- Provides a framework within which to teach beginning nursing students.
- Logically congruent, externally and internally consistent, has breadth and depth, and is understood, with few exceptions, by professionals and consumers of health care.
See Also: Martha Rogers: Theory of Unitary Human Beings
- In Roger’s Theory of Human Beings , she defined Nursing as “an art and science that is humanistic and humanitarian.
- The Science of Unitary Human Beings contains two dimensions: the science of nursing, which is the knowledge specific to the field of nursing that comes from scientific research; and the art of nursing, which involves using nursing creatively to help better the lives of the patient.
- A patient can’t be separated from his or her environment when addressing health and treatment.
See Also: Dorothea E. Orem: Self-Care Theory
- In her Self-Care Theory , she defined Nursing as “The act of assisting others in the provision and management of self-care to maintain or improve human functioning at the home level of effectiveness.”
- Focuses on each individual’s ability to perform self-care .
- Composed of three interrelated theories: (1) the theory of self-care , (2) the self-care deficit theory, and (3) the theory of nursing systems, which is further classified into wholly compensatory, partially compensatory, and supportive-educative.
See Also: Imogene M. King: Theory of Goal Attainment
- Conceptual System and Middle-Range Theory of Goal Attainment
- “Nursing is a process of action, reaction and interaction by which nurse and client share information about their perception in a nursing situation” and “a process of human interactions between nurse and client whereby each perceives the other and the situation, and through communication , they set goals, explore means, and agree on means to achieve goals.”
- Focuses on this process to guide and direct nurses in the nurse-patient relationship, going hand-in-hand with their patients to meet good health goals.
- Explains that the nurse and patient go hand-in-hand in communicating information, set goals together, and then take actions to achieve those goals.
See Also: Betty Neuman: Neuman’s Systems Model
- In Neuman’s System Model , she defined nursing as a “unique profession in that is concerned with all of the variables affecting an individual’s response to stress.”
- The focus is on the client as a system (which may be an individual, family, group, or community) and on the client’s responses to stressors.
- The client system includes five variables (physiological, psychological, sociocultural, developmental, and spiritual). It is conceptualized as an inner core (basic energy resources) surrounded by concentric circles that include lines of resistance, a normal defense line, and a flexible line of defense.
See Also: Sister Callista Roy: Adaptation Model of Nursing
- In Adaptation Model , Roy defined nursing as a “health care profession that focuses on human life processes and patterns and emphasizes the promotion of health for individuals, families, groups, and society as a whole.”
- Views the individual as a set of interrelated systems that strives to maintain a balance between various stimuli.
- Inspired the development of many middle-range nursing theories and adaptation instruments.
See Also: Dorothy E. Johnson: Behavioral Systems Model
- The Behavioral System Model defined Nursing as “an external regulatory force that acts to preserve the organization and integrate the patients’ behaviors at an optimum level under those conditions in which the behavior constitutes a threat to the physical or social health or in which illness is found.”
- Advocates to foster efficient and effective behavioral functioning in the patient to prevent illness and stresses the importance of research-based knowledge about the effect of nursing care on patients.
- Describes the person as a behavioral system with seven subsystems: the achievement, attachment-affiliative, aggressive-protective, dependency, ingestive, eliminative, and sexual subsystems.
- The Theory of Nursing as Caring: A Model for Transforming Practice
- Nursing is an “exquisitely interwoven” unity of aspects of the discipline and profession of nursing.
- Nursing’s focus and aim as a discipline of knowledge and a professional service are “nurturing persons living to care and growing in caring.”
- Caring in nursing is “an altruistic, active expression of love, and is the intentional and embodied recognition of value and connectedness.”
- Transitions Theory
- It began with observations of experiences faced as people deal with changes related to health, well-being, and the ability to care for themselves.
- Types of transitions include developmental, health and illness, situational, and organizational.
- Acknowledges the role of nurses as they help people go through health/illness and life transitions.
- Focuses on assisting nurses in facilitating patients’, families’, and communities’ healthy transitions.
See Also: Nola Pender: Health Promotion Model
- Health Promotion Model
- Describes the interaction between the nurse and the consumer while considering the role of the health promotion environment.
- It focuses on three areas: individual characteristics and experiences, behavior-specific cognitions and affect, and behavioral outcomes.
- Describes the multidimensional nature of persons as they interact within their environment to pursue health.
See Also: Madeleine M. Leininger: Transcultural Nursing Theory
- Culture Care Theory of Diversity and Universality
- Defined transcultural nursing as “a substantive area of study and practice focused on comparative cultural care (caring) values, beliefs, and practices of individuals or groups of similar or different cultures to provide culture-specific and universal nursing care practices in promoting health or well-being or to help people to face unfavorable human conditions, illness, or death in culturally meaningful ways.”
- Involves learning and understanding various cultures regarding nursing and health-illness caring practices, beliefs, and values to implement significant and efficient nursing care services to people according to their cultural values and health-illness context.
- It focuses on the fact that various cultures have different and unique caring behaviors and different health and illness values, beliefs, and patterns of behaviors.
- Health as Expanding Consciousness
- “Nursing is the process of recognizing the patient in relation to the environment, and it is the process of the understanding of consciousness.”
- “The theory of health as expanding consciousness was stimulated by concern for those for whom health as the absence of disease or disability is not possible . . . “
- Nursing is regarded as a connection between the nurse and patient, and both grow in the sense of higher levels of consciousness.
- Human Becoming Theory
- “Nursing is a science, and the performing art of nursing is practiced in relationships with persons (individuals, groups, and communities) in their processes of becoming.”
- Explains that a person is more than the sum of the parts, the environment, and the person is inseparable and that nursing is a human science and art that uses an abstract body of knowledge to help people.
- It centered around three themes: meaning, rhythmicity, and transcendence.
- Modeling and Role-Modeling
- “Nursing is the holistic helping of persons with their self-care activities in relation to their health . . . The goal is to achieve a state of perceived optimum health and contentment.”
- Modeling is a process that allows nurses to understand the unique perspective of a client and learn to appreciate its importance.
- Role-modeling occurs when the nurse plans and implements interventions that are unique for the client.
- Created the Symphonological Bioethical Theory
- “Symphonology (from ‘ symphonia ,’ a Greek word meaning agreement) is a system of ethics based on the terms and preconditions of an agreement.”
- Nursing cannot occur without both nurse and patient. “A nurse takes no actions that are not interactions.”
- Founded on the singular concept of human rights, the essential agreement of non-aggression among rational people forms the foundation of all human interaction.
- Maternal Role Attainment—Becoming a Mother
- “Nursing is a dynamic profession with three major foci: health promotion and prevention of illness, providing care for those who need professional assistance to achieve their optimal level of health and functioning, and research to enhance the knowledge base for providing excellent nursing care.”
- “Nurses are the health professionals having the most sustained and intense interaction with women in the maternity cycle.”
- Maternal role attainment is an interactional and developmental process occurring over time. The mother becomes attached to her infant, acquires competence in the caretaking tasks involved in the role, and expresses pleasure and gratification. (Mercer, 1986).
- Provides proper health care interventions for nontraditional mothers for them to favorably adopt a strong maternal identity.
- Uncertainty in Illness Theory
- Presents a comprehensive structure to view the experience of acute and chronic illness and organize nursing interventions to promote optimal adjustment.
- Describes how individuals form meaning from illness-related situations.
- The original theory’s concepts were organized in a linear model around the following three major themes: Antecedents of uncertainty, Process of uncertainty appraisal, and Coping with uncertainty.
- Self-Transcendence Theory
- Self-transcendence refers to the fluctuation of perceived boundaries that extend the person (or self) beyond the immediate and constricted views of self and the world (Reed, 1997).
- Has three basic concepts: vulnerability, self-transcendence, and well-being.
- Gives insight into the developmental nature of humans associated with health circumstances connected to nursing care.
- Theory of Illness Trajectory
- “The uncertainty surrounding a chronic illness like cancer is the uncertainty of life writ large. By listening to those who are tolerating this exaggerated uncertainty, we can learn much about the trajectory of living.”
- Provides a framework for nurses to understand how cancer patients stand uncertainty manifested as a loss of control.
- Provides new knowledge on how patients and families endure uncertainty and work strategically to reduce uncertainty through a dynamic flow of illness events, treatment situations, and varied players involved in care organization.
- Theory of Chronic Sorrow
- “Chronic sorrow is the presence of pervasive grief -related feelings that have been found to occur periodically throughout the lives of individuals with chronic health conditions, their family caregivers and the bereaved.”
- This middle-range theory defines the aspect of chronic sorrow as a normal response to the ongoing disparity created by the loss.
- Barker’s Tidal Model of Mental Health Recovery is widely used in mental health nursing.
- It focuses on nursing’s fundamental care processes, is universally applicable, and is a practical guide for psychiatry and mental health nursing.
- Draws on values about relating to people and help others in their moments of distress. The values of the Tidal Model are revealed in the Ten Commitments: Value the voice, Respect the language, Develop genuine curiosity, Become the apprentice, Use the available toolkit, Craft the step beyond, Give the gift of time, Reveal personal wisdom, Know that change is constant, and Be transparent.
- Theory of Comfort
- “Comfort is an antidote to the stressors inherent in health care situations today, and when comfort is enhanced, patients and families are strengthened for the tasks ahead. Also, nurses feel more satisfied with the care they are giving.”
- Patient comfort exists in three forms: relief, ease, and transcendence. These comforts can occur in four contexts: physical, psychospiritual, environmental, and sociocultural.
- As a patient’s comfort needs change, the nurse’s interventions change, as well.
- Postpartum Depression Theory
- “The birth of a baby is an occasion for joy—or so the saying goes […] But for some women, joy is not an option.”
- Described nursing as a caring profession with caring obligations to persons we care for, students, and each other.
- Provides evidence to understand and prevent postpartum depression .
- Theory of Caring
- “Caring is a nurturing way of relating to a valued other toward whom one feels a personal sense of commitment and responsibility.”
- Defines nursing as informed caring for the well-being of others.
- Offers a structure for improving up-to-date nursing practice, education, and research while bringing the discipline to its traditional values and caring-healing roots.
- Peaceful End-of-Life Theory
- The focus was not on death itself but on providing a peaceful and meaningful living in the time that remained for patients and their significant others.
- The purpose was to reflect the complexity involved in caring for terminally ill patients.
- Also known as Wanda Horta, she introduced the concepts of nursing that are accepted in Brazil.
- Wrote the book Nursing Process which presents relevance to the various fields of Nursing practice for providing a holistic view of the patient.
- Her work was recognized in all the teaching institutions called the Theory of Basic Human Needs . It is based on Maslow’s Theory of Human Motivation, whose primary concept is the hierarchy of Basic Human Needs (BHN).
- Horta’s Theory of Basic Human Needs is considered the highest point of her work, and the summary of all her research concludes sickness as a science and art of assisting a human being in meeting basic human needs, making the patient independent of this assistance through education in recovery, maintenance, and health promotion .
- Classified basic human needs into three main dimensions – psychobiological, psychosocial and psychospiritual – and establishes a relationship between the concepts of human being, environment, and nursing.
- The theory describes nursing as an element of a healthcare team and states that it can function efficiently through a scientific method. Horta referred this method as the nursing process .
- She defined the nursing process as the dynamics of systematic and interrelated actions to assist human beings. It is characterized by six phases: nursing history, nursing diagnosis , assistance plan, care plan or nursing prescription, evolution, and prognosis.
Recommended books and resources to learn more about nursing theory:
Disclosure: Included below are affiliate links from Amazon at no additional cost from you. We may earn a small commission from your purchase. For more information, check out our privacy policy .
- Nursing Theorists and Their Work (10th Edition) by Alligood Nursing Theorists and Their Work, 10th Edition provides a clear, in-depth look at nursing theories of historical and international significance. Each chapter presents a key nursing theory or philosophy, showing how systematic theoretical evidence can enhance decision making, professionalism, and quality of care.
- Knowledge Development in Nursing: Theory and Process (11th Edition) Use the five patterns of knowing to help you develop sound clinical judgment. This edition reflects the latest thinking in nursing knowledge development and adds emphasis to real-world application. The content in this edition aligns with the new 2021 AACN Essentials for Nursing Education.
- Nursing Knowledge and Theory Innovation, Second Edition: Advancing the Science of Practice (2nd Edition) This text for graduate-level nursing students focuses on the science and philosophy of nursing knowledge development. It is distinguished by its focus on practical applications of theory for scholarly, evidence-based approaches. The second edition features important updates and a reorganization of information to better highlight the roles of theory and major philosophical perspectives.
- Nursing Theories and Nursing Practice (5th Edition) The only nursing research and theory book with primary works by the original theorists. Explore the historical and contemporary theories that are the foundation of nursing practice today. The 5th Edition, continues to meet the needs of today’s students with an expanded focus on the middle range theories and practice models.
- Strategies for Theory Construction in Nursing (6th Edition) The clearest, most useful introduction to theory development methods. Reflecting vast changes in nursing practice, it covers advances both in theory development and in strategies for concept, statement, and theory development. It also builds further connections between nursing theory and evidence-based practice.
- Middle Range Theory for Nursing (4th Edition) This nursing book’s ability to break down complex ideas is part of what made this book a three-time recipient of the AJN Book of the Year award. This edition includes five completely new chapters of content essential for nursing books. New exemplars linking middle range theory to advanced nursing practice make it even more useful and expand the content to make it better.
- Nursing Research: Methods and Critical Appraisal for Evidence-Based Practice This book offers balanced coverage of both qualitative and quantitative research methodologies. This edition features new content on trending topics, including the Next-Generation NCLEX® Exam (NGN).
- Nursing Research (11th Edition) AJN award-winning authors Denise Polit and Cheryl Beck detail the latest methodologic innovations in nursing, medicine, and the social sciences. The updated 11th Edition adds two new chapters designed to help students ensure the accuracy and effectiveness of research methods. Extensively revised content throughout strengthens students’ ability to locate and rank clinical evidence.
Recommended site resources related to nursing theory:
- Nursing Theories and Theorists: The Definitive Guide for Nurses MUST READ! In this guide for nursing theories, we aim to help you understand what comprises a nursing theory and its importance, purpose, history, types or classifications, and give you an overview through summaries of selected nursing theories.
Other resources related to nursing theory:
- Betty Neuman: Neuman Systems Model
- Dorothea Orem: Self-Care Deficit Theory
- Dorothy Johnson: Behavioral System Model
- Faye Abdellah: 21 Nursing Problems Theory
- Florence Nightingale: Environmental Theory
- Hildegard Peplau: Interpersonal Relations Theory
- Ida Jean Orlando: Deliberative Nursing Process Theory
- Imogene King: Theory of Goal Attainment
- Jean Watson: Theory of Human Caring
- Lydia Hall: Care, Cure, Core Nursing Theory
- Madeleine Leininger: Transcultural Nursing Theory
- Martha Rogers: Science of Unitary Human Beings
- Myra Estrin Levine: The Conservation Model of Nursing
- Nola Pender: Health Promotion Model
- Sister Callista Roy: Adaptation Model of Nursing
- Virginia Henderson: Nursing Need Theory
Suggested readings and resources for this study guide :
- Alligood, M., & Tomey, A. (2010). Nursing theorists and their work, seventh edition (No ed.). Maryland Heights: Mosby-Elsevier.
- Alligood, M. R. (2017). Nursing Theorists and Their Work-E-Book . Elsevier Health Sciences.
- Barnard, K. E. (1984). Nursing research related to infants and young children. In Annual review of nursing research (pp. 3-25). Springer, Berlin, Heidelberg.
- Brown, H. I. (1979). Perception, theory, and commitment: The new philosophy of science . University of Chicago Press. [ Link ]
- Brown M (1964) Research in the development of nursing theory: the importance of a theoretical framework in nursing research. Nursing Research.
- Camacho, A. C. L. F., & Joaquim, F. L. (2017). Reflections based on Wanda Horta on the basic instruments of nursing. Rev Enferm UFPE [Internet], 11(12), 5432-8.
- Chinn, P. L., & Jacobs, M. K. (1978). A model for theory development in nursing. Advances in Nursing Science , 1 (1), 1-12. [ Link ]
- Colley, S. (2003). Nursing theory: its importance to practice. Nursing Standard (through 2013), 17(46), 33. [ Link ]
- Fawcett, J. (2005). Criteria for evaluation of theory. Nursing science quarterly, 18(2), 131-135. [ Link ]
- Fitzpatrick, J. J., & Whall, A. L. (Eds.). (1996). Conceptual models of nursing: Analysis and application . Connecticut, Norwalk: Appleton & Lange.
- Kaplan, A. (2017). The conduct of inquiry: Methodology for behavioural science . Routledge. [ Link ]
- Meleis, A. I. (2011). Theoretical nursing: Development and progress . Lippincott Williams & Wilkins.
- Neuman, B. M., & Fawcett, J. (2002). The Neuman systems model .
- Nightingale F (1860) Notes on Nursing. New York NY, Appleton.
- Perão, O. F., Zandonadi, G. C., Rodríguez, A. H., Fontes, M. S., Nascimento, E. L. P., & Santos, E. K. A. (2017). Patient safety in an intensive care unit according to Wanda Horta’s theory. Cogitare Enfermagem, 22(3), e45657.
- Peplau H (1988) The art and science of nursing: similarities, differences, and relations. Nursing Science Quarterly
- Rogers M (1970) An Introduction to the Theoretical Basis of Nursing. Philadelphia PA, FA Davis.
49 thoughts on “Nursing Theories and Theorists: The Definitive Guide for Nurses”
Great work indeed
Amazing and simple post I have ever come across about nursing theories.
Thank you for the simplicity
where do i find the reference page in apa format?
The reference listed below the article is in APA format.
i love this. insightful. Comprehensive ,Well researched .
Thank you for these theories they are a life saver and simplified. My school require us to write about 2 nursing theorist from memory for a Comprehensive exam in which if you do not pass it you are required to wait for a year to retake the exam.
Merci beaucoup, puisque je suis très satisfait.
I’m pleased to congratulate you about your work! I really appreciate it! From: Cameroon
An entire’s semester worth of a nursing theory class, expertly and succinctly summarized in one paper. I wish my instructor were as easy to understand. Good work.
I thought this was in a chronological order based on their published works date? Then why Orlando’s theory comes at the later part? Can someone englighten me please because I am making a timeline for our project.
Great job. Very clear and succinct.
I like it. Well explained!
easy to understand and very helpful
thankyou very much.
The article was beneficial to me to understand nursing theories
This is amazing and I love it so enriching!
Thanks for the article may God bless you more Plus More Power and Protection
Thanks so much
Please can someone help me with a nursing theory related to “teamwork” please
Thank you so much !
I loved the text and saw that the nursing theorist Wanda Aguiar Horta, a Brazilian nurse and great theorist regarding basic human needs, was not included.
I suggest reviewing and including it to be more complete.
If you need, I can help with inclusion!
Best Regards
Hi João Carlos, we’d love to hear about her work. Please send us the details via our contact page: https://nurseslabs.com/contact/
Excellent study guide! Detailed, Informative and Valued! Thank you!
hi can someone help me which theorist can relate in Ear, Nose, Throat nursing care.
Wonderful contribution of shared knowledge- now how do we get the word out for nurses that are not able to afford a BSN?
Thanks for the work. It’s very helpful
This has helped me understand theories a bit better, however, there is one that is eluding me. Where does the normative theory fit in?
very educative.I have understood theories more than before.Thanks
hard work. great work in deed
I love reading your material, plain concise and easy
Very informative, more knowledgeable about the theorist
Thank you for your information. This material is great and when I have looked for material for nursing theory. I got is material with complete
A big hand of applause 👏🏿 This is a treasure for nurses of the world. Thank you so much
Hi G. ALex,
Wow, thanks for the awesome feedback! 😊 Super glad you found it to be a treasure. Just curious, was there a particular section that stood out to you or something you’d love to see more of? Always keen to hear what resonates with fellow nurses!
This is really hard work put together in a very easy to understand way.Thank you so much.It came handy
Hi Sigala, Thanks a ton for noticing the effort! 😊 Super happy to hear it came in handy for you. If you ever have suggestions or topics you’d like to see, give me a shout. Cheers to making things understandable!
Absolutely helpful. Thank you.
So glad to hear the nursing theories guide was a hit for you! 😊 If you have any other topics or questions in mind, just give a shout. Always here to help. Keep rocking your studies! Thanks Ishe!
Am happy, to read these theories, very educating. Am going to make use of it when caring for my patients. GREAT NURSES GREAT! I LOVE YOU ALL.
Hi Eboh, I’m thrilled to hear you’re excited about applying these nursing theories in practice! They can really enhance the care we provide. It’s all about putting that knowledge to good use. By the way, which theory resonated with you the most, or which do you see being most applicable in your day-to-day patient care?
How do I relate one of the theories to effective management of intravenous lines? Which theory and how to relate to the above?
Hi wanted to ask you who wrote this page who is the autor because i need to write them on footnotes and i can’t find autor of the page,neither the year it was published. Thank you. Btw this article was really helpful i never understood nursing theories this good.
Hey there Innaya, I’m glad to hear the article on nursing theories was so helpful to you! Here’s how you can cite it in APA format:
Vera, M. (2019, September 11). Nursing Theories and Theorists: The Definitive Guide for Nurses Nurseslabs. https://nurseslabs.com/nursing-theories/
If you need any more help with citations or have other questions, feel free to ask. Happy to assist!
Please is there an app I could download all these from?
Hi Felicia, Thanks for your interest! As of now, we don’t have a dedicated app for downloading our content. However, our website is mobile-friendly, so you can easily access all our resources from your smartphone or tablet browser.
wonderful insights, and very precise and easy to understand, I even got to know and learn about other new theorists of Nursing I didn’t know before.
Thank you so much for this wonderful work.
Its so amazing and very helpful. Please how can I cite any of these theory using Vancouver?
Leave a Comment Cancel reply
- Bipolar Disorder
- Therapy Center
- When To See a Therapist
- Types of Therapy
- Best Online Therapy
- Best Couples Therapy
- Best Family Therapy
- Managing Stress
- Sleep and Dreaming
- Understanding Emotions
- Self-Improvement
- Healthy Relationships
- Student Resources
- Personality Types
- Guided Meditations
- Verywell Mind Insights
- 2024 Verywell Mind 25
- Mental Health in the Classroom
- Editorial Process
- Meet Our Review Board
- Crisis Support
How to Write a Great Hypothesis
Hypothesis Definition, Format, Examples, and Tips
Kendra Cherry, MS, is a psychosocial rehabilitation specialist, psychology educator, and author of the "Everything Psychology Book."
:max_bytes(150000):strip_icc():format(webp)/IMG_9791-89504ab694d54b66bbd72cb84ffb860e.jpg "example nursing hypothesis")
Amy Morin, LCSW, is a psychotherapist and international bestselling author. Her books, including "13 Things Mentally Strong People Don't Do," have been translated into more than 40 languages. Her TEDx talk, "The Secret of Becoming Mentally Strong," is one of the most viewed talks of all time.
:max_bytes(150000):strip_icc():format(webp)/VW-MIND-Amy-2b338105f1ee493f94d7e333e410fa76.jpg "example nursing hypothesis")
Verywell / Alex Dos Diaz
- The Scientific Method
Hypothesis Format
Falsifiability of a hypothesis.
- Operationalization
Hypothesis Types
Hypotheses examples.
- Collecting Data
A hypothesis is a tentative statement about the relationship between two or more variables. It is a specific, testable prediction about what you expect to happen in a study. It is a preliminary answer to your question that helps guide the research process.
Consider a study designed to examine the relationship between sleep deprivation and test performance. The hypothesis might be: "This study is designed to assess the hypothesis that sleep-deprived people will perform worse on a test than individuals who are not sleep-deprived."
At a Glance
A hypothesis is crucial to scientific research because it offers a clear direction for what the researchers are looking to find. This allows them to design experiments to test their predictions and add to our scientific knowledge about the world. This article explores how a hypothesis is used in psychology research, how to write a good hypothesis, and the different types of hypotheses you might use.
The Hypothesis in the Scientific Method
In the scientific method , whether it involves research in psychology, biology, or some other area, a hypothesis represents what the researchers think will happen in an experiment. The scientific method involves the following steps:
- Forming a question
- Performing background research
- Creating a hypothesis
- Designing an experiment
- Collecting data
- Analyzing the results
- Drawing conclusions
- Communicating the results
The hypothesis is a prediction, but it involves more than a guess. Most of the time, the hypothesis begins with a question which is then explored through background research. At this point, researchers then begin to develop a testable hypothesis.
Unless you are creating an exploratory study, your hypothesis should always explain what you expect to happen.
In a study exploring the effects of a particular drug, the hypothesis might be that researchers expect the drug to have some type of effect on the symptoms of a specific illness. In psychology, the hypothesis might focus on how a certain aspect of the environment might influence a particular behavior.
Remember, a hypothesis does not have to be correct. While the hypothesis predicts what the researchers expect to see, the goal of the research is to determine whether this guess is right or wrong. When conducting an experiment, researchers might explore numerous factors to determine which ones might contribute to the ultimate outcome.
In many cases, researchers may find that the results of an experiment do not support the original hypothesis. When writing up these results, the researchers might suggest other options that should be explored in future studies.
In many cases, researchers might draw a hypothesis from a specific theory or build on previous research. For example, prior research has shown that stress can impact the immune system. So a researcher might hypothesize: "People with high-stress levels will be more likely to contract a common cold after being exposed to the virus than people who have low-stress levels."
In other instances, researchers might look at commonly held beliefs or folk wisdom. "Birds of a feather flock together" is one example of folk adage that a psychologist might try to investigate. The researcher might pose a specific hypothesis that "People tend to select romantic partners who are similar to them in interests and educational level."
Elements of a Good Hypothesis
So how do you write a good hypothesis? When trying to come up with a hypothesis for your research or experiments, ask yourself the following questions:
- Is your hypothesis based on your research on a topic?
- Can your hypothesis be tested?
- Does your hypothesis include independent and dependent variables?
Before you come up with a specific hypothesis, spend some time doing background research. Once you have completed a literature review, start thinking about potential questions you still have. Pay attention to the discussion section in the journal articles you read . Many authors will suggest questions that still need to be explored.
How to Formulate a Good Hypothesis
To form a hypothesis, you should take these steps:
- Collect as many observations about a topic or problem as you can.
- Evaluate these observations and look for possible causes of the problem.
- Create a list of possible explanations that you might want to explore.
- After you have developed some possible hypotheses, think of ways that you could confirm or disprove each hypothesis through experimentation. This is known as falsifiability.
In the scientific method , falsifiability is an important part of any valid hypothesis. In order to test a claim scientifically, it must be possible that the claim could be proven false.
Students sometimes confuse the idea of falsifiability with the idea that it means that something is false, which is not the case. What falsifiability means is that if something was false, then it is possible to demonstrate that it is false.
One of the hallmarks of pseudoscience is that it makes claims that cannot be refuted or proven false.
The Importance of Operational Definitions
A variable is a factor or element that can be changed and manipulated in ways that are observable and measurable. However, the researcher must also define how the variable will be manipulated and measured in the study.
Operational definitions are specific definitions for all relevant factors in a study. This process helps make vague or ambiguous concepts detailed and measurable.
For example, a researcher might operationally define the variable " test anxiety " as the results of a self-report measure of anxiety experienced during an exam. A "study habits" variable might be defined by the amount of studying that actually occurs as measured by time.
These precise descriptions are important because many things can be measured in various ways. Clearly defining these variables and how they are measured helps ensure that other researchers can replicate your results.
Replicability
One of the basic principles of any type of scientific research is that the results must be replicable.
Replication means repeating an experiment in the same way to produce the same results. By clearly detailing the specifics of how the variables were measured and manipulated, other researchers can better understand the results and repeat the study if needed.
Some variables are more difficult than others to define. For example, how would you operationally define a variable such as aggression ? For obvious ethical reasons, researchers cannot create a situation in which a person behaves aggressively toward others.
To measure this variable, the researcher must devise a measurement that assesses aggressive behavior without harming others. The researcher might utilize a simulated task to measure aggressiveness in this situation.
Hypothesis Checklist
- Does your hypothesis focus on something that you can actually test?
- Does your hypothesis include both an independent and dependent variable?
- Can you manipulate the variables?
- Can your hypothesis be tested without violating ethical standards?
The hypothesis you use will depend on what you are investigating and hoping to find. Some of the main types of hypotheses that you might use include:
- Simple hypothesis : This type of hypothesis suggests there is a relationship between one independent variable and one dependent variable.
- Complex hypothesis : This type suggests a relationship between three or more variables, such as two independent and dependent variables.
- Null hypothesis : This hypothesis suggests no relationship exists between two or more variables.
- Alternative hypothesis : This hypothesis states the opposite of the null hypothesis.
- Statistical hypothesis : This hypothesis uses statistical analysis to evaluate a representative population sample and then generalizes the findings to the larger group.
- Logical hypothesis : This hypothesis assumes a relationship between variables without collecting data or evidence.
A hypothesis often follows a basic format of "If {this happens} then {this will happen}." One way to structure your hypothesis is to describe what will happen to the dependent variable if you change the independent variable .
The basic format might be: "If {these changes are made to a certain independent variable}, then we will observe {a change in a specific dependent variable}."
A few examples of simple hypotheses:
- "Students who eat breakfast will perform better on a math exam than students who do not eat breakfast."
- "Students who experience test anxiety before an English exam will get lower scores than students who do not experience test anxiety."
- "Motorists who talk on the phone while driving will be more likely to make errors on a driving course than those who do not talk on the phone."
- "Children who receive a new reading intervention will have higher reading scores than students who do not receive the intervention."
Examples of a complex hypothesis include:
- "People with high-sugar diets and sedentary activity levels are more likely to develop depression."
- "Younger people who are regularly exposed to green, outdoor areas have better subjective well-being than older adults who have limited exposure to green spaces."
Examples of a null hypothesis include:
- "There is no difference in anxiety levels between people who take St. John's wort supplements and those who do not."
- "There is no difference in scores on a memory recall task between children and adults."
- "There is no difference in aggression levels between children who play first-person shooter games and those who do not."
Examples of an alternative hypothesis:
- "People who take St. John's wort supplements will have less anxiety than those who do not."
- "Adults will perform better on a memory task than children."
- "Children who play first-person shooter games will show higher levels of aggression than children who do not."
Collecting Data on Your Hypothesis
Once a researcher has formed a testable hypothesis, the next step is to select a research design and start collecting data. The research method depends largely on exactly what they are studying. There are two basic types of research methods: descriptive research and experimental research.
Descriptive Research Methods
Descriptive research such as case studies , naturalistic observations , and surveys are often used when conducting an experiment is difficult or impossible. These methods are best used to describe different aspects of a behavior or psychological phenomenon.
Once a researcher has collected data using descriptive methods, a correlational study can examine how the variables are related. This research method might be used to investigate a hypothesis that is difficult to test experimentally.
Experimental Research Methods
Experimental methods are used to demonstrate causal relationships between variables. In an experiment, the researcher systematically manipulates a variable of interest (known as the independent variable) and measures the effect on another variable (known as the dependent variable).
Unlike correlational studies, which can only be used to determine if there is a relationship between two variables, experimental methods can be used to determine the actual nature of the relationship—whether changes in one variable actually cause another to change.
The hypothesis is a critical part of any scientific exploration. It represents what researchers expect to find in a study or experiment. In situations where the hypothesis is unsupported by the research, the research still has value. Such research helps us better understand how different aspects of the natural world relate to one another. It also helps us develop new hypotheses that can then be tested in the future.
Thompson WH, Skau S. On the scope of scientific hypotheses . R Soc Open Sci . 2023;10(8):230607. doi:10.1098/rsos.230607
Taran S, Adhikari NKJ, Fan E. Falsifiability in medicine: what clinicians can learn from Karl Popper [published correction appears in Intensive Care Med. 2021 Jun 17;:]. Intensive Care Med . 2021;47(9):1054-1056. doi:10.1007/s00134-021-06432-z
Eyler AA. Research Methods for Public Health . 1st ed. Springer Publishing Company; 2020. doi:10.1891/9780826182067.0004
Nosek BA, Errington TM. What is replication ? PLoS Biol . 2020;18(3):e3000691. doi:10.1371/journal.pbio.3000691
Aggarwal R, Ranganathan P. Study designs: Part 2 - Descriptive studies . Perspect Clin Res . 2019;10(1):34-36. doi:10.4103/picr.PICR_154_18
Nevid J. Psychology: Concepts and Applications. Wadworth, 2013.
By Kendra Cherry, MSEd Kendra Cherry, MS, is a psychosocial rehabilitation specialist, psychology educator, and author of the "Everything Psychology Book."
- Resources Home 🏠
- Try SciSpace Copilot
- Search research papers
- Add Copilot Extension
- Try AI Detector
- Try Paraphraser
- Try Citation Generator
- April Papers
- June Papers
- July Papers

The Craft of Writing a Strong Hypothesis

Table of Contents
Writing a hypothesis is one of the essential elements of a scientific research paper. It needs to be to the point, clearly communicating what your research is trying to accomplish. A blurry, drawn-out, or complexly-structured hypothesis can confuse your readers. Or worse, the editor and peer reviewers.
A captivating hypothesis is not too intricate. This blog will take you through the process so that, by the end of it, you have a better idea of how to convey your research paper's intent in just one sentence.
What is a Hypothesis?
The first step in your scientific endeavor, a hypothesis, is a strong, concise statement that forms the basis of your research. It is not the same as a thesis statement , which is a brief summary of your research paper .
The sole purpose of a hypothesis is to predict your paper's findings, data, and conclusion. It comes from a place of curiosity and intuition . When you write a hypothesis, you're essentially making an educated guess based on scientific prejudices and evidence, which is further proven or disproven through the scientific method.
The reason for undertaking research is to observe a specific phenomenon. A hypothesis, therefore, lays out what the said phenomenon is. And it does so through two variables, an independent and dependent variable.
The independent variable is the cause behind the observation, while the dependent variable is the effect of the cause. A good example of this is “mixing red and blue forms purple.” In this hypothesis, mixing red and blue is the independent variable as you're combining the two colors at your own will. The formation of purple is the dependent variable as, in this case, it is conditional to the independent variable.
Different Types of Hypotheses

Types of hypotheses
Some would stand by the notion that there are only two types of hypotheses: a Null hypothesis and an Alternative hypothesis. While that may have some truth to it, it would be better to fully distinguish the most common forms as these terms come up so often, which might leave you out of context.
Apart from Null and Alternative, there are Complex, Simple, Directional, Non-Directional, Statistical, and Associative and casual hypotheses. They don't necessarily have to be exclusive, as one hypothesis can tick many boxes, but knowing the distinctions between them will make it easier for you to construct your own.
1. Null hypothesis
A null hypothesis proposes no relationship between two variables. Denoted by H 0 , it is a negative statement like “Attending physiotherapy sessions does not affect athletes' on-field performance.” Here, the author claims physiotherapy sessions have no effect on on-field performances. Even if there is, it's only a coincidence.
2. Alternative hypothesis
Considered to be the opposite of a null hypothesis, an alternative hypothesis is donated as H1 or Ha. It explicitly states that the dependent variable affects the independent variable. A good alternative hypothesis example is “Attending physiotherapy sessions improves athletes' on-field performance.” or “Water evaporates at 100 °C. ” The alternative hypothesis further branches into directional and non-directional.
- Directional hypothesis: A hypothesis that states the result would be either positive or negative is called directional hypothesis. It accompanies H1 with either the ‘<' or ‘>' sign.
- Non-directional hypothesis: A non-directional hypothesis only claims an effect on the dependent variable. It does not clarify whether the result would be positive or negative. The sign for a non-directional hypothesis is ‘≠.'
3. Simple hypothesis
A simple hypothesis is a statement made to reflect the relation between exactly two variables. One independent and one dependent. Consider the example, “Smoking is a prominent cause of lung cancer." The dependent variable, lung cancer, is dependent on the independent variable, smoking.
4. Complex hypothesis
In contrast to a simple hypothesis, a complex hypothesis implies the relationship between multiple independent and dependent variables. For instance, “Individuals who eat more fruits tend to have higher immunity, lesser cholesterol, and high metabolism.” The independent variable is eating more fruits, while the dependent variables are higher immunity, lesser cholesterol, and high metabolism.
5. Associative and casual hypothesis
Associative and casual hypotheses don't exhibit how many variables there will be. They define the relationship between the variables. In an associative hypothesis, changing any one variable, dependent or independent, affects others. In a casual hypothesis, the independent variable directly affects the dependent.
6. Empirical hypothesis
Also referred to as the working hypothesis, an empirical hypothesis claims a theory's validation via experiments and observation. This way, the statement appears justifiable and different from a wild guess.
Say, the hypothesis is “Women who take iron tablets face a lesser risk of anemia than those who take vitamin B12.” This is an example of an empirical hypothesis where the researcher the statement after assessing a group of women who take iron tablets and charting the findings.
7. Statistical hypothesis
The point of a statistical hypothesis is to test an already existing hypothesis by studying a population sample. Hypothesis like “44% of the Indian population belong in the age group of 22-27.” leverage evidence to prove or disprove a particular statement.
Characteristics of a Good Hypothesis
Writing a hypothesis is essential as it can make or break your research for you. That includes your chances of getting published in a journal. So when you're designing one, keep an eye out for these pointers:
- A research hypothesis has to be simple yet clear to look justifiable enough.
- It has to be testable — your research would be rendered pointless if too far-fetched into reality or limited by technology.
- It has to be precise about the results —what you are trying to do and achieve through it should come out in your hypothesis.
- A research hypothesis should be self-explanatory, leaving no doubt in the reader's mind.
- If you are developing a relational hypothesis, you need to include the variables and establish an appropriate relationship among them.
- A hypothesis must keep and reflect the scope for further investigations and experiments.
Separating a Hypothesis from a Prediction
Outside of academia, hypothesis and prediction are often used interchangeably. In research writing, this is not only confusing but also incorrect. And although a hypothesis and prediction are guesses at their core, there are many differences between them.
A hypothesis is an educated guess or even a testable prediction validated through research. It aims to analyze the gathered evidence and facts to define a relationship between variables and put forth a logical explanation behind the nature of events.
Predictions are assumptions or expected outcomes made without any backing evidence. They are more fictionally inclined regardless of where they originate from.
For this reason, a hypothesis holds much more weight than a prediction. It sticks to the scientific method rather than pure guesswork. "Planets revolve around the Sun." is an example of a hypothesis as it is previous knowledge and observed trends. Additionally, we can test it through the scientific method.
Whereas "COVID-19 will be eradicated by 2030." is a prediction. Even though it results from past trends, we can't prove or disprove it. So, the only way this gets validated is to wait and watch if COVID-19 cases end by 2030.
Finally, How to Write a Hypothesis

Quick tips on writing a hypothesis
1. Be clear about your research question
A hypothesis should instantly address the research question or the problem statement. To do so, you need to ask a question. Understand the constraints of your undertaken research topic and then formulate a simple and topic-centric problem. Only after that can you develop a hypothesis and further test for evidence.
2. Carry out a recce
Once you have your research's foundation laid out, it would be best to conduct preliminary research. Go through previous theories, academic papers, data, and experiments before you start curating your research hypothesis. It will give you an idea of your hypothesis's viability or originality.
Making use of references from relevant research papers helps draft a good research hypothesis. SciSpace Discover offers a repository of over 270 million research papers to browse through and gain a deeper understanding of related studies on a particular topic. Additionally, you can use SciSpace Copilot , your AI research assistant, for reading any lengthy research paper and getting a more summarized context of it. A hypothesis can be formed after evaluating many such summarized research papers. Copilot also offers explanations for theories and equations, explains paper in simplified version, allows you to highlight any text in the paper or clip math equations and tables and provides a deeper, clear understanding of what is being said. This can improve the hypothesis by helping you identify potential research gaps.
3. Create a 3-dimensional hypothesis
Variables are an essential part of any reasonable hypothesis. So, identify your independent and dependent variable(s) and form a correlation between them. The ideal way to do this is to write the hypothetical assumption in the ‘if-then' form. If you use this form, make sure that you state the predefined relationship between the variables.
In another way, you can choose to present your hypothesis as a comparison between two variables. Here, you must specify the difference you expect to observe in the results.
4. Write the first draft
Now that everything is in place, it's time to write your hypothesis. For starters, create the first draft. In this version, write what you expect to find from your research.
Clearly separate your independent and dependent variables and the link between them. Don't fixate on syntax at this stage. The goal is to ensure your hypothesis addresses the issue.
5. Proof your hypothesis
After preparing the first draft of your hypothesis, you need to inspect it thoroughly. It should tick all the boxes, like being concise, straightforward, relevant, and accurate. Your final hypothesis has to be well-structured as well.
Research projects are an exciting and crucial part of being a scholar. And once you have your research question, you need a great hypothesis to begin conducting research. Thus, knowing how to write a hypothesis is very important.
Now that you have a firmer grasp on what a good hypothesis constitutes, the different kinds there are, and what process to follow, you will find it much easier to write your hypothesis, which ultimately helps your research.
Now it's easier than ever to streamline your research workflow with SciSpace Discover . Its integrated, comprehensive end-to-end platform for research allows scholars to easily discover, write and publish their research and fosters collaboration.
It includes everything you need, including a repository of over 270 million research papers across disciplines, SEO-optimized summaries and public profiles to show your expertise and experience.
If you found these tips on writing a research hypothesis useful, head over to our blog on Statistical Hypothesis Testing to learn about the top researchers, papers, and institutions in this domain.
Frequently Asked Questions (FAQs)
1. what is the definition of hypothesis.
According to the Oxford dictionary, a hypothesis is defined as “An idea or explanation of something that is based on a few known facts, but that has not yet been proved to be true or correct”.
2. What is an example of hypothesis?
The hypothesis is a statement that proposes a relationship between two or more variables. An example: "If we increase the number of new users who join our platform by 25%, then we will see an increase in revenue."
3. What is an example of null hypothesis?
A null hypothesis is a statement that there is no relationship between two variables. The null hypothesis is written as H0. The null hypothesis states that there is no effect. For example, if you're studying whether or not a particular type of exercise increases strength, your null hypothesis will be "there is no difference in strength between people who exercise and people who don't."
4. What are the types of research?
• Fundamental research
• Applied research
• Qualitative research
• Quantitative research
• Mixed research
• Exploratory research
• Longitudinal research
• Cross-sectional research
• Field research
• Laboratory research
• Fixed research
• Flexible research
• Action research
• Policy research
• Classification research
• Comparative research
• Causal research
• Inductive research
• Deductive research
5. How to write a hypothesis?
• Your hypothesis should be able to predict the relationship and outcome.
• Avoid wordiness by keeping it simple and brief.
• Your hypothesis should contain observable and testable outcomes.
• Your hypothesis should be relevant to the research question.
6. What are the 2 types of hypothesis?
• Null hypotheses are used to test the claim that "there is no difference between two groups of data".
• Alternative hypotheses test the claim that "there is a difference between two data groups".
7. Difference between research question and research hypothesis?
A research question is a broad, open-ended question you will try to answer through your research. A hypothesis is a statement based on prior research or theory that you expect to be true due to your study. Example - Research question: What are the factors that influence the adoption of the new technology? Research hypothesis: There is a positive relationship between age, education and income level with the adoption of the new technology.
8. What is plural for hypothesis?
The plural of hypothesis is hypotheses. Here's an example of how it would be used in a statement, "Numerous well-considered hypotheses are presented in this part, and they are supported by tables and figures that are well-illustrated."
9. What is the red queen hypothesis?
The red queen hypothesis in evolutionary biology states that species must constantly evolve to avoid extinction because if they don't, they will be outcompeted by other species that are evolving. Leigh Van Valen first proposed it in 1973; since then, it has been tested and substantiated many times.
10. Who is known as the father of null hypothesis?
The father of the null hypothesis is Sir Ronald Fisher. He published a paper in 1925 that introduced the concept of null hypothesis testing, and he was also the first to use the term itself.
11. When to reject null hypothesis?
You need to find a significant difference between your two populations to reject the null hypothesis. You can determine that by running statistical tests such as an independent sample t-test or a dependent sample t-test. You should reject the null hypothesis if the p-value is less than 0.05.
You might also like

Consensus GPT vs. SciSpace GPT: Choose the Best GPT for Research

Literature Review and Theoretical Framework: Understanding the Differences

Types of Essays in Academic Writing - Quick Guide (2024)
Warning: The NCBI web site requires JavaScript to function. more...

An official website of the United States government
The .gov means it's official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- Browse Titles
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Open Resources for Nursing (Open RN); Ernstmeyer K, Christman E, editors. Nursing Fundamentals [Internet]. Eau Claire (WI): Chippewa Valley Technical College; 2021.

Nursing Fundamentals [Internet].
- About Open RN
Chapter 4 Nursing Process
4.1. nursing process introduction, learning objectives.
- Use the nursing process to provide patient care
- Identify nursing diagnoses from evidence-based sources
- Describe the development of a care plan
- Prioritize patient care
- Describe documentation for each step of the nursing process
- Differentiate between the role of the PN and RN
Have you ever wondered how a nurse can receive a quick handoff report from another nurse and immediately begin providing care for a patient they previously knew nothing about? How do they know what to do? How do they prioritize and make a plan?
Nurses do this activity every shift. They know how to find pertinent information and use the nursing process as a critical thinking model to guide patient care. The nursing process becomes a road map for the actions and interventions that nurses implement to optimize their patients’ well-being and health. This chapter will explain how to use the nursing process as standards of professional nursing practice to provide safe, patient-centered care.
4.2. BASIC CONCEPTS
Before learning how to use the nursing process, it is important to understand some basic concepts related to critical thinking and nursing practice. Let’s take a deeper look at how nurses think.
Critical Thinking and Clinical Reasoning
Nurses make decisions while providing patient care by using critical thinking and clinical reasoning. Critical thinking is a broad term used in nursing that includes “reasoning about clinical issues such as teamwork, collaboration, and streamlining workflow.” [ 1 ] Using critical thinking means that nurses take extra steps to maintain patient safety and don’t just “follow orders.” It also means the accuracy of patient information is validated and plans for caring for patients are based on their needs, current clinical practice, and research.
“Critical thinkers” possess certain attitudes that foster rational thinking. These attitudes are as follows:
- Independence of thought: Thinking on your own
- Fair-mindedness: Treating every viewpoint in an unbiased, unprejudiced way
- Insight into egocentricity and sociocentricity: Thinking of the greater good and not just thinking of yourself. Knowing when you are thinking of yourself (egocentricity) and when you are thinking or acting for the greater good (sociocentricity)
- Intellectual humility: Recognizing your intellectual limitations and abilities
- Nonjudgmental: Using professional ethical standards and not basing your judgments on your own personal or moral standards
- Integrity: Being honest and demonstrating strong moral principles
- Perseverance: Persisting in doing something despite it being difficult
- Confidence: Believing in yourself to complete a task or activity
- Interest in exploring thoughts and feelings: Wanting to explore different ways of knowing
- Curiosity: Asking “why” and wanting to know more
Clinical reasoning is defined as, “A complex cognitive process that uses formal and informal thinking strategies to gather and analyze patient information, evaluate the significance of this information, and weigh alternative actions.” [ 2 ] To make sound judgments about patient care, nurses must generate alternatives, weigh them against the evidence, and choose the best course of action. The ability to clinically reason develops over time and is based on knowledge and experience. [ 3 ]
Inductive and Deductive Reasoning and Clinical Judgment
Inductive and deductive reasoning are important critical thinking skills. They help the nurse use clinical judgment when implementing the nursing process.
Inductive reasoning involves noticing cues, making generalizations, and creating hypotheses. Cues are data that fall outside of expected findings that give the nurse a hint or indication of a patient’s potential problem or condition. The nurse organizes these cues into patterns and creates a generalization. A generalization is a judgment formed from a set of facts, cues, and observations and is similar to gathering pieces of a jigsaw puzzle into patterns until the whole picture becomes more clear. Based on generalizations created from patterns of data, the nurse creates a hypothesis regarding a patient problem. A hypothesis is a proposed explanation for a situation. It attempts to explain the “why” behind the problem that is occurring. If a “why” is identified, then a solution can begin to be explored.
No one can draw conclusions without first noticing cues. Paying close attention to a patient, the environment, and interactions with family members is critical for inductive reasoning. As you work to improve your inductive reasoning, begin by first noticing details about the things around you. A nurse is similar to the detective looking for cues in Figure 4.1 . [ 4 ] Be mindful of your five primary senses: the things that you hear, feel, smell, taste, and see. Nurses need strong inductive reasoning patterns and be able to take action quickly, especially in emergency situations. They can see how certain objects or events form a pattern (i.e., generalization) that indicates a common problem (i.e., hypothesis).
Inductive Reasoning Includes Looking for Cues
Example: A nurse assesses a patient and finds the surgical incision site is red, warm, and tender to the touch. The nurse recognizes these cues form a pattern of signs of infection and creates a hypothesis that the incision has become infected. The provider is notified of the patient’s change in condition, and a new prescription is received for an antibiotic. This is an example of the use of inductive reasoning in nursing practice.
Deductive reasoning is another type of critical thinking that is referred to as “top-down thinking.” Deductive reasoning relies on using a general standard or rule to create a strategy. Nurses use standards set by their state’s Nurse Practice Act, federal regulations, the American Nursing Association, professional organizations, and their employer to make decisions about patient care and solve problems.
Example: Based on research findings, hospital leaders determine patients recover more quickly if they receive adequate rest. The hospital creates a policy for quiet zones at night by initiating no overhead paging, promoting low-speaking voices by staff, and reducing lighting in the hallways. (See Figure 4.2 ). [ 5 ] The nurse further implements this policy by organizing care for patients that promotes periods of uninterrupted rest at night. This is an example of deductive thinking because the intervention is applied to all patients regardless if they have difficulty sleeping or not.
Deductive Reasoning Example: Implementing Interventions for a Quiet Zone Policy
Clinical judgment is the result of critical thinking and clinical reasoning using inductive and deductive reasoning. Clinical judgment is defined by the National Council of State Boards of Nursing (NCSBN) as, “The observed outcome of critical thinking and decision-making. It uses nursing knowledge to observe and assess presenting situations, identify a prioritized patient concern, and generate the best possible evidence-based solutions in order to deliver safe patient care.” [ 6 ] The NCSBN administers the national licensure exam (NCLEX) that measures nursing clinical judgment and decision-making ability of prospective entry-level nurses to assure safe and competent nursing care by licensed nurses.
Evidence-based practice (EBP) is defined by the American Nurses Association (ANA) as, “A lifelong problem-solving approach that integrates the best evidence from well-designed research studies and evidence-based theories; clinical expertise and evidence from assessment of the health care consumer’s history and condition, as well as health care resources; and patient, family, group, community, and population preferences and values.” [ 7 ]
Nursing Process
The nursing process is a critical thinking model based on a systematic approach to patient-centered care. Nurses use the nursing process to perform clinical reasoning and make clinical judgments when providing patient care. The nursing process is based on the Standards of Professional Nursing Practice established by the American Nurses Association (ANA). These standards are authoritative statements of the actions and behaviors that all registered nurses, regardless of role, population, specialty, and setting, are expected to perform competently. [ 8 ] The mnemonic ADOPIE is an easy way to remember the ANA Standards and the nursing process. Each letter refers to the six components of the nursing process: A ssessment, D iagnosis, O utcomes Identification, P lanning, I mplementation, and E valuation.
The nursing process is a continuous, cyclic process that is constantly adapting to the patient’s current health status. See Figure 4.3 [ 9 ] for an illustration of the nursing process.
The Nursing Process
Review Scenario A in the following box for an example of a nurse using the nursing process while providing patient care.
Patient Scenario A: Using the Nursing Process [ 10 ]

A hospitalized patient has a prescription to receive Lasix 80mg IV every morning for a medical diagnosis of heart failure. During the morning assessment, the nurse notes that the patient has a blood pressure of 98/60, heart rate of 100, respirations of 18, and a temperature of 98.7F. The nurse reviews the medical record for the patient’s vital signs baseline and observes the blood pressure trend is around 110/70 and the heart rate in the 80s. The nurse recognizes these cues form a pattern related to fluid imbalance and hypothesizes that the patient may be dehydrated. The nurse gathers additional information and notes the patient’s weight has decreased 4 pounds since yesterday. The nurse talks with the patient and validates the hypothesis when the patient reports that their mouth feels like cotton and they feel light-headed. By using critical thinking and clinical judgment, the nurse diagnoses the patient with the nursing diagnosis Fluid Volume Deficit and establishes outcomes for reestablishing fluid balance. The nurse withholds the administration of IV Lasix and contacts the health care provider to discuss the patient’s current fluid status. After contacting the provider, the nurse initiates additional nursing interventions to promote oral intake and closely monitor hydration status. By the end of the shift, the nurse evaluates the patient status and determines that fluid balance has been restored.
In Scenario A, the nurse is using clinical judgment and not just “following orders” to administer the Lasix as scheduled. The nurse assesses the patient, recognizes cues, creates a generalization and hypothesis regarding the fluid status, plans and implements nursing interventions, and evaluates the outcome. Additionally, the nurse promotes patient safety by contacting the provider before administering a medication that could cause harm to the patient at this time.
The ANA’s Standards of Professional Nursing Practice associated with each component of the nursing process are described below.
The “Assessment” Standard of Practice is defined as, “The registered nurse collects pertinent data and information relative to the health care consumer’s health or the situation.” [ 11 ] A registered nurse uses a systematic method to collect and analyze patient data. Assessment includes physiological data, as well as psychological, sociocultural, spiritual, economic, and lifestyle data. For example, a nurse’s assessment of a hospitalized patient in pain includes the patient’s response to pain, such as the inability to get out of bed, refusal to eat, withdrawal from family members, or anger directed at hospital staff. [ 12 ]
The “Assessment” component of the nursing process is further described in the “ Assessment ” section of this chapter.
The “Diagnosis” Standard of Practice is defined as, “The registered nurse analyzes the assessment data to determine actual or potential diagnoses, problems, and issues.” [ 13 ] A nursing diagnosis is the nurse’s clinical judgment about the client's response to actual or potential health conditions or needs. Nursing diagnoses are the bases for the nurse’s care plan and are different than medical diagnoses. [ 14 ]
The “Diagnosis” component of the nursing process is further described in the “ Diagnosis ” section of this chapter.
Outcomes Identification
The “Outcomes Identification” Standard of Practice is defined as, “The registered nurse identifies expected outcomes for a plan individualized to the health care consumer or the situation.” [ 15 ] The nurse sets measurable and achievable short- and long-term goals and specific outcomes in collaboration with the patient based on their assessment data and nursing diagnoses.
The “Outcomes Identification” component of the nursing process is further described in the “ Outcomes Identification ” section of this chapter.
The “Planning” Standard of Practice is defined as, “The registered nurse develops a collaborative plan encompassing strategies to achieve expected outcomes.” [ 16 ] Assessment data, diagnoses, and goals are used to select evidence-based nursing interventions customized to each patient’s needs and concerns. Goals, expected outcomes, and nursing interventions are documented in the patient’s nursing care plan so that nurses, as well as other health professionals, have access to it for continuity of care. [ 17 ]
The “Planning” component of the nursing process is further described in the “ Planning ” section of this chapter.
NURSING CARE PLANS
Creating nursing care plans is a part of the “Planning” step of the nursing process. A nursing care plan is a type of documentation that demonstrates the individualized planning and delivery of nursing care for each specific patient using the nursing process. Registered nurses (RNs) create nursing care plans so that the care provided to the patient across shifts is consistent among health care personnel. Some interventions can be delegated to Licensed Practical Nurses (LPNs) or trained Unlicensed Assistive Personnel (UAPs) with the RN’s supervision. Developing nursing care plans and implementing appropriate delegation are further discussed under the “ Planning ” and “ Implementing ” sections of this chapter.
Implementation
The “Implementation” Standard of Practice is defined as, “The nurse implements the identified plan.” [ 18 ] Nursing interventions are implemented or delegated with supervision according to the care plan to assure continuity of care across multiple nurses and health professionals caring for the patient. Interventions are also documented in the patient’s electronic medical record as they are completed. [ 19 ]
The “Implementation” Standard of Professional Practice also includes the subcategories “Coordination of Care” and “Health Teaching and Health Promotion” to promote health and a safe environment. [ 20 ]
The “Implementation” component of the nursing process is further described in the “ Implementation ” section of this chapter.
The “Evaluation” Standard of Practice is defined as, “The registered nurse evaluates progress toward attainment of goals and outcomes.” [ 21 ] During evaluation, nurses assess the patient and compare the findings against the initial assessment to determine the effectiveness of the interventions and overall nursing care plan. Both the patient’s status and the effectiveness of the nursing care must be continuously evaluated and modified as needed. [ 22 ]
The “Evaluation” component of the nursing process is further described in the “ Evaluation ” section of this chapter.
Benefits of Using the Nursing Process
Using the nursing process has many benefits for nurses, patients, and other members of the health care team. The benefits of using the nursing process include the following:
- Promotes quality patient care
- Decreases omissions and duplications
- Provides a guide for all staff involved to provide consistent and responsive care
- Encourages collaborative management of a patient’s health care problems
- Improves patient safety
- Improves patient satisfaction
- Identifies a patient’s goals and strategies to attain them
- Increases the likelihood of achieving positive patient outcomes
- Saves time, energy, and frustration by creating a care plan or path to follow
By using these components of the nursing process as a critical thinking model, nurses plan interventions customized to the patient’s needs, plan outcomes and interventions, and determine whether those actions are effective in meeting the patient’s needs. In the remaining sections of this chapter, we will take an in-depth look at each of these components of the nursing process. Using the nursing process and implementing evidence-based practices are referred to as the “science of nursing.” Let’s review concepts related to the “art of nursing” while providing holistic care in a caring manner using the nursing process.
Holistic Nursing Care
The American Nurses Association (ANA) recently updated the definition of nursing as, “Nursing integrates the art and science of caring and focuses on the protection, promotion, and optimization of health and human functioning; prevention of illness and injury; facilitation of healing; and alleviation of suffering through compassionate presence. Nursing is the diagnosis and treatment of human responses and advocacy in the care of individuals, families, groups, communities, and populations in the recognition of the connection of all humanity.” [ 23 ]
The ANA further describes nursing is a learned profession built on a core body of knowledge that integrates both the art and science of nursing. The art of nursing is defined as, “Unconditionally accepting the humanity of others, respecting their need for dignity and worth, while providing compassionate, comforting care.” [ 24 ]
Nurses care for individuals holistically, including their emotional, spiritual, psychosocial, cultural, and physical needs. They consider problems, issues, and needs that the person experiences as a part of a family and a community as they use the nursing process. Review a scenario illustrating holistic nursing care provided to a patient and their family in the following box.
Holistic Nursing Care Scenario
A single mother brings her child to the emergency room for ear pain and a fever. The physician diagnoses the child with an ear infection and prescribes an antibiotic. The mother is advised to make a follow-up appointment with their primary provider in two weeks. While providing discharge teaching, the nurse discovers that the family is unable to afford the expensive antibiotic prescribed and cannot find a primary care provider in their community they can reach by a bus route. The nurse asks a social worker to speak with the mother about affordable health insurance options and available providers in her community and follows up with the prescribing physician to obtain a prescription for a less expensive generic antibiotic. In this manner, the nurse provides holistic care and advocates for improved health for the child and their family.
Review how to provide culturally responsive care and reduce health disparities in the “ Diverse Patients ” chapter.
Caring and the nursing process.
The American Nurses Association (ANA) states, “The act of caring is foundational to the practice of nursing.” [ 25 ] Successful use of the nursing process requires the development of a care relationship with the patient. A care relationship is a mutual relationship that requires the development of trust between both parties. This trust is often referred to as the development of rapport and underlies the art of nursing. While establishing a caring relationship, the whole person is assessed, including the individual’s beliefs, values, and attitudes, while also acknowledging the vulnerability and dignity of the patient and family. Assessing and caring for the whole person takes into account the physical, mental, emotional, and spiritual aspects of being a human being. [ 26 ] Caring interventions can be demonstrated in simple gestures such as active listening, making eye contact, touching, and verbal reassurances while also respecting and being sensitive to the care recipient’s cultural beliefs and meanings associated with caring behaviors. [ 27 ] See Figure 4.4 [ 28 ] for an image of a nurse using touch as a therapeutic communication technique to communicate caring.
Touch as a Therapeutic Communication Technique
Review how to communicate with patients using therapeutic communication techniques like active listening in the “ Communication ” chapter.
Dr. Jean Watson is a nurse theorist who has published many works on the art and science of caring in the nursing profession. Her theory of human caring sought to balance the cure orientation of medicine, giving nursing its unique disciplinary, scientific, and professional standing with itself and the public. Dr. Watson’s caring philosophy encourages nurses to be authentically present with their patients while creating a healing environment. [ 29 ]
Read more about Dr. Watson’s theory of caring at the Watson Caring Science Institute .
Now that we have discussed basic concepts related to the nursing process, let’s look more deeply at each component of the nursing process in the following sections.
4.3. ASSESSMENT
Assessment is the first step of the nursing process (and the first Standard of Practice set by the American Nurses Association). This standard is defined as, “The registered nurse collects pertinent data and information relative to the health care consumer’s health or the situation.” This includes collecting “pertinent data related to the health and quality of life in a systematic, ongoing manner, with compassion and respect for the wholeness, inherent dignity, worth, and unique attributes of every person, including but not limited to, demographics, environmental and occupational exposures, social determinants of health, health disparities, physical, functional, psychosocial, emotional, cognitive, spiritual/transpersonal, sexual, sociocultural, age-related, environmental, and lifestyle/economic assessments.” [ 1 ]
Nurses assess patients to gather clues, make generalizations, and diagnose human responses to health conditions and life processes. Patient data is considered either subjective or objective, and it can be collected from multiple sources.
Subjective Assessment Data
Subjective data is information obtained from the patient and/or family members and offers important cues from their perspectives. When documenting subjective data stated by a patient, it should be in quotation marks and start with verbiage such as, The patient reports. It is vital for the nurse to establish rapport with a patient to obtain accurate, valuable subjective data regarding the mental, emotional, and spiritual aspects of their condition.
There are two types of subjective information, primary and secondary. Primary data is information provided directly by the patient. Patients are the best source of information about their bodies and feelings, and the nurse who actively listens to a patient will often learn valuable information while also promoting a sense of well-being. Information collected from a family member, chart, or other sources is known as secondary data . Family members can provide important information, especially for individuals with memory impairments, infants, children, or when patients are unable to speak for themselves.
See Figure 4.5 [ 2 ] for an illustration of a nurse obtaining subjective data and establishing rapport after obtaining permission from the patient to sit on the bed.
Example. An example of documented subjective data obtained from a patient assessment is, “The patient reports, ‘My pain is a level 2 on a 1-10 scale.’”
Objective Assessment Data
Objective data is anything that you can observe through your sense of hearing, sight, smell, and touch while assessing the patient. Objective data is reproducible, meaning another person can easily obtain the same data. Examples of objective data are vital signs, physical examination findings, and laboratory results. See Figure 4.6 [ 3 ] for an image of a nurse performing a physical examination.
Physical Examination
Example. An example of documented objective data is, “The patient’s radial pulse is 58 and regular, and their skin feels warm and dry.”
Sources of Assessment Data
There are three sources of assessment data: interview, physical examination, and review of laboratory or diagnostic test results.
Interviewing
Interviewing includes asking the patient questions, listening, and observing verbal and nonverbal communication. Reviewing the chart prior to interviewing the patient may eliminate redundancy in the interview process and allows the nurse to hone in on the most significant areas of concern or need for clarification. However, if information in the chart does not make sense or is incomplete, the nurse should use the interview process to verify data with the patient.
After performing patient identification, the best way to initiate a caring relationship is to introduce yourself to the patient and explain your role. Share the purpose of your interview and the approximate time it will take. When beginning an interview, it may be helpful to start with questions related to the patient’s medical diagnoses to gather information about how they have affected the patient’s functioning, relationships, and lifestyle. Listen carefully and ask for clarification when something isn’t clear to you. Patients may not volunteer important information because they don’t realize it is important for their care. By using critical thinking and active listening, you may discover valuable cues that are important to provide safe, quality nursing care. Sometimes nursing students can feel uncomfortable having difficult conversations or asking personal questions due to generational or other cultural differences. Don’t shy away from asking about information that is important to know for safe patient care. Most patients will be grateful that you cared enough to ask and listen.
Be alert and attentive to how the patient answers questions, as well as when they do not answer a question. Nonverbal communication and body language can be cues to important information that requires further investigation. A keen sense of observation is important. To avoid making inappropriate inferences , the nurse should validate any cues. For example, a nurse may make an inference that a patient is depressed when the patient avoids making eye contact during an interview. However, upon further questioning, the nurse may discover that the patient’s cultural background believes direct eye contact to be disrespectful and this is why they are avoiding eye contact. To read more information about communicating with patients, review the “ Communication ” chapter of this book.
A physical examination is a systematic data collection method of the body that uses the techniques of inspection, auscultation, palpation, and percussion. Inspection is the observation of a patient’s anatomical structures. Auscultation is listening to sounds, such as heart, lung, and bowel sounds, created by organs using a stethoscope. Palpation is the use of touch to evaluate organs for size, location, or tenderness. Percussion is an advanced physical examination technique typically performed by providers where body parts are tapped with fingers to determine their size and if fluid is present. Detailed physical examination procedures of various body systems can be found in the Open RN Nursing Skills textbook with a head-to-toe checklist in Appendix C . Physical examination also includes the collection and analysis of vital signs.
Registered Nurses (RNs) complete the initial physical examination and analyze the findings as part of the nursing process. Collection of follow-up physical examination data can be delegated to Licensed Practical Nurses/Licensed Vocational Nurses (LPNs/LVNs) , or measurements such as vital signs and weight may be delegated to trained Unlicensed Assistive Personnel (UAP) when appropriate to do so. However, the RN remains responsible for supervising these tasks, analyzing the findings, and ensuring they are documented .
A physical examination can be performed as a comprehensive, head-to-toe assessment or as a focused assessment related to a particular condition or problem. Assessment data is documented in the patient’s Electronic Medical Record (EMR) , an electronic version of the patient’s medical chart.
Reviewing Laboratory and Diagnostic Test Results
Reviewing laboratory and diagnostic test results provides relevant and useful information related to the needs of the patient. Understanding how normal and abnormal results affect patient care is important when implementing the nursing care plan and administering provider prescriptions. If results cause concern, it is the nurse’s responsibility to notify the provider and verify the appropriateness of prescriptions based on the patient’s current status before implementing them.
Types of Assessments
Several types of nursing assessment are used in clinical practice:
- Primary Survey: Used during every patient encounter to briefly evaluate level of consciousness, airway, breathing, and circulation and implement emergency care if needed.
- Admission Assessment: A comprehensive assessment completed when a patient is admitted to a facility that involves assessing a large amount of information using an organized approach.
- Ongoing Assessment: In acute care agencies such as hospitals, a head-to-toe assessment is completed and documented at least once every shift. Any changes in patient condition are reported to the health care provider.
- Focused Assessment: Focused assessments are used to reevaluate the status of a previously diagnosed problem.
- Time-lapsed Reassessment: Time-lapsed reassessments are used in long-term care facilities when three or more months have elapsed since the previous assessment to evaluate progress on previously identified outcomes. [ 4 ]
Putting It Together
Review Scenario C in the following box to apply concepts of assessment to a patient scenario.
Scenario C [5]

Ms. J. is a 74-year-old woman who is admitted directly to the medical unit after visiting her physician because of shortness of breath, increased swelling in her ankles and calves, and fatigue. Her medical history includes hypertension (30 years), coronary artery disease (18 years), heart failure (2 years), and type 2 diabetes (14 years). She takes 81 mg of aspirin every day, metoprolol 50 mg twice a day, furosemide 40 mg every day, and metformin 2,000 mg every day.
Ms. J.’s vital sign values on admission were as follows:
- Blood Pressure: 162/96 mm Hg
- Heart Rate: 88 beats/min
- Oxygen Saturation: 91% on room air
- Respiratory Rate: 28 breaths/minute
- Temperature: 97.8 degrees F orally
Her weight is up 10 pounds since the last office visit three weeks prior. The patient states, “I am so short of breath” and “My ankles are so swollen I have to wear my house slippers.” Ms. J. also shares, “I am so tired and weak that I can’t get out of the house to shop for groceries,” and “Sometimes I’m afraid to get out of bed because I get so dizzy.” She confides, “I would like to learn more about my health so I can take better care of myself.”
The physical assessment findings of Ms. J. are bilateral basilar crackles in the lungs and bilateral 2+ pitting edema of the ankles and feet. Laboratory results indicate a decreased serum potassium level of 3.4 mEq/L.
As the nurse completes the physical assessment, the patient’s daughter enters the room. She confides, “We are so worried about mom living at home by herself when she is so tired all the time!”
Critical Thinking Questions
Identify subjective data.
Identify objective data.
Provide an example of secondary data.
Answers are located in the Answer Key at the end of the book.
4.4. DIAGNOSIS
Diagnosis is the second step of the nursing process (and the second Standard of Practice set by the American Nurses Association). This standard is defined as, “The registered nurse analyzes assessment data to determine actual or potential diagnoses, problems, and issues.” The RN “prioritizes diagnoses, problems, and issues based on mutually established goals to meet the needs of the health care consumer across the health–illness continuum and the care continuum.” Diagnoses, problems, strengths, and issues are documented in a manner that facilitates the development of expected outcomes and a collaborative plan. [ 1 ]
Analyzing Assessment Data
After collection of assessment data, the registered nurse analyzes the data to form generalizations and create hypotheses for nursing diagnoses. Steps for analyzing assessment data include performing data analysis, clustering of information, identifying hypotheses for potential nursing diagnosis, performing additional in-depth assessment as needed, and establishing nursing diagnosis statements. The nursing diagnoses are then prioritized and drive the nursing care plan. [ 2 ]
Performing Data Analysis
After nurses collect assessment data from a patient, they use their nursing knowledge to analyze that data to determine if it is “expected” or “unexpected” or “normal” or “abnormal” for that patient according to their age, development, and baseline status. From there, nurses determine what data are “clinically relevant” as they prioritize their nursing care. [ 3 ]
Example. In Scenario C in the “Assessment” section of this chapter, the nurse analyzes the vital signs data and determines the blood pressure, heart rate, and respiratory rate are elevated, and the oxygen saturation is decreased for this patient. These findings are considered “relevant cues.”
Clustering Information/Seeing Patterns/Making Hypotheses
After analyzing the data and determining relevant cues, the nurse clusters data into patterns. Assessment frameworks such as Gordon’s Functional Health Patterns assist nurses in clustering information according to evidence-based patterns of human responses. See the box below for an outline of Gordon’s Functional Health Patterns. [ 4 ] Concepts related to many of these patterns will be discussed in chapters later in this book.
Example. Refer to Scenario C of the “Assessment” section of this chapter. The nurse clusters the following relevant cues: elevated blood pressure, elevated respiratory rate, crackles in the lungs, weight gain, worsening edema, shortness of breath, a medical history of heart failure, and currently prescribed a diuretic medication. These cues are clustered into a generalization/pattern of fluid balance, which can be classified under Gordon’s Nutritional-Metabolic Functional Health Pattern. The nurse makes a hypothesis that the patient has excess fluid volume present.
Gordon’s Functional Health Patterns [ 5 ]
Health Perception-Health Management: A patient’s perception of their health and well-being and how it is managed
Nutritional-Metabolic: Food and fluid consumption relative to metabolic need
Elimination: Excretory function, including bowel, bladder, and skin
Activity-Exercise: Exercise and daily activities
Sleep-Rest: Sleep, rest, and daily activities
Cognitive-Perceptual: Perception and cognition
Self-perception and Self-concept: Self-concept and perception of self-worth, self-competency, body image, and mood state
Role-Relationship: Role engagements and relationships
Sexuality-Reproductive: Reproduction and satisfaction or dissatisfaction with sexuality
Coping-Stress Tolerance: Coping and effectiveness in terms of stress tolerance
Value-Belief: Values, beliefs (including spiritual beliefs), and goals that guide choices and decisions
Identifying Nursing Diagnoses
After the nurse has analyzed and clustered the data from the patient assessment, the next step is to begin to answer the question, “What are my patient’s human responses (i.e., nursing diagnoses)?” A nursing diagnosis is defined as, “A clinical judgment concerning a human response to health conditions/life processes, or a vulnerability for that response, by an individual, family, group, or community.” [ 6 ] Nursing diagnoses are customized to each patient and drive the development of the nursing care plan. The nurse should refer to a care planning resource and review the definitions and defining characteristics of the hypothesized nursing diagnoses to determine if additional in-depth assessment is needed before selecting the most accurate nursing diagnosis.
Nursing diagnoses are developed by nurses, for use by nurses. For example, NANDA International (NANDA-I) is a global professional nursing organization that develops nursing terminology that names actual or potential human responses to health problems and life processes based on research findings. [ 7 ] Currently, there are over 220 NANDA-I nursing diagnoses developed by nurses around the world. This list is continuously updated, with new nursing diagnoses added and old nursing diagnoses retired that no longer have supporting evidence. A list of commonly used NANDA-I diagnoses are listed in Appendix A . For a full list of NANDA-I nursing diagnoses, refer to a current nursing care plan reference.
NANDA-I nursing diagnoses are grouped into 13 domains that assist the nurse in selecting diagnoses based on the patterns of clustered data. These domains are similar to Gordon’s Functional Health Patterns and include health promotion, nutrition, elimination and exchange, activity/rest, perception/cognition, self-perception, role relationship, sexuality, coping/stress tolerance, life principles, safety/protection, comfort, and growth/development.
Knowledge regarding specific NANDA-I nursing diagnoses is not assessed on the NCLEX. However, analyzing cues and creating hypotheses are part of the measurement model used to assess a candidate’s clinical judgment. Read more about the NCLEX and Next Generation NCLEX in the “ Scope of Practice ” chapter.
Nursing diagnoses vs. medical diagnoses.
You may be asking yourself, “How are nursing diagnoses different from medical diagnoses?” Medical diagnoses focus on diseases or other medical problems that have been identified by the physician, physician’s assistant, or advanced nurse practitioner. Nursing diagnoses focus on the human response to health conditions and life processes and are made independently by RNs. Patients with the same medical diagnosis will often respond differently to that diagnosis and thus have different nursing diagnoses. For example, two patients have the same medical diagnosis of heart failure. However, one patient may be interested in learning more information about the condition and the medications used to treat it, whereas another patient may be experiencing anxiety when thinking about the effects this medical diagnosis will have on their family. The nurse must consider these different responses when creating the nursing care plan. Nursing diagnoses consider the patient’s and family’s needs, attitudes, strengths, challenges, and resources as a customized nursing care plan is created to provide holistic and individualized care for each patient.
Example. A medical diagnosis identified for Ms. J. in Scenario C in the “Assessment” section is heart failure. This cannot be used as a nursing diagnosis, but it can be considered as an “associated condition” when creating hypotheses for nursing diagnoses. Associated conditions are medical diagnoses, injuries, procedures, medical devices, or pharmacological agents that are not independently modifiable by the nurse, but support accuracy in nursing diagnosis. The nursing diagnosis in Scenario C will be related to the patient’s response to heart failure.
Additional Definitions Used in NANDA-I Nursing Diagnoses
The following definitions of patient, age, and time are used in association with NANDA-I nursing diagnoses:
The NANDA-I definition of a “patient” includes:
- Individual: a single human being distinct from others (i.e., a person).
- Caregiver: a family member or helper who regularly looks after a child or a sick, elderly, or disabled person.
- Family: two or more people having continuous or sustained relationships, perceiving reciprocal obligations, sensing common meaning, and sharing certain obligations toward others; related by blood and/or choice.
- Group: a number of people with shared characteristics generally referred to as an ethnic group.
- Community: a group of people living in the same locale under the same governance. Examples include neighborhoods and cities. [ 8 ]
The age of the person who is the subject of the diagnosis is defined by the following terms: [ 9 ]
- Fetus: an unborn human more than eight weeks after conception, until birth.
- Neonate: a person less than 28 days of age.
- Infant: a person greater than 28 days and less than 1 year of age.
- Child: a person aged 1 to 9 years
- Adolescent: a person aged 10 to 19 years
- Adult: a person older than 19 years of age unless national law defines a person as being an adult at an earlier age.
- Older adult: a person greater than 65 years of age.
The duration of the diagnosis is defined by the following terms: [ 10 ]
- Acute: lasting less than 3 months.
- Chronic: lasting greater than 3 months.
- Intermittent: stopping or starting again at intervals
- Continuous: uninterrupted, going on without stop.
New Terms Used in 2018-2020 NANDA-I Diagnoses
The 2018-2020 edition of Nursing Diagnoses includes two new terms to assist in creating nursing diagnoses: at-risk populations and associated conditions. [ 11 ]
At-Risk Populations are groups of people who share a characteristic that causes each member to be susceptible to a particular human response, such as demographics, health/family history, stages of growth/development, or exposure to certain events/experiences.
Associated Conditions are medical diagnoses, injuries, procedures, medical devices, or pharmacological agents. These conditions are not independently modifiable by the nurse, but support accuracy in nursing diagnosis [ 12 ]
Types of Nursing Diagnoses
There are four types of NANDA-I nursing diagnoses: [ 13 ]
- Problem-Focused
- Health Promotion – Wellness
A problem-focused nursing diagnosis is a “clinical judgment concerning an undesirable human response to health condition/life processes that exist in an individual, family, group, or community.” [ 14 ] To make an accurate problem-focused diagnosis, related factors and defining characteristics must be present. Related factors (also called etiology) are causes that contribute to the diagnosis. Defining characteristics are cues, signs, and symptoms that cluster into patterns. [ 15 ]
A health promotion-wellness nursing diagnosis is “a clinical judgment concerning motivation and desire to increase well-being and to actualize human health potential.” These responses are expressed by the patient’s readiness to enhance specific health behaviors. [ 16 ] A health promotion-wellness diagnosis is used when the patient is willing to improve a lack of knowledge, coping, or other identified need.
A risk nursing diagnosis is “a clinical judgment concerning the vulnerability of an individual, family, group, or community for developing an undesirable human response to health conditions/life processes.” [ 17 ] A risk nursing diagnosis must be supported by risk factors that contribute to the increased vulnerability. A risk nursing diagnosis is different from the problem-focused diagnosis in that the problem has not yet actually occurred. Problem diagnoses should not be automatically viewed as more important than risk diagnoses because sometimes a risk diagnosis can have the highest priority for a patient. [ 18 ]
A syndrome diagnosis is a “clinical judgment concerning a specific cluster of nursing diagnoses that occur together, and are best addressed together and through similar interventions.” [ 19 ]
Establishing Nursing Diagnosis Statements
When using NANDA-I nursing diagnoses, NANDA-I recommends the structure of a nursing diagnosis should be a statement that includes the nursing diagnosis and related factors as exhibited by defining characteristics . The accuracy of the nursing diagnosis is validated when a nurse is able to clearly link the defining characteristics, related factors, and/or risk factors found during the patient’s assessment. [ 20 ]
To create a nursing diagnosis statement, the registered nurse completes the following steps. After analyzing the patient’s subjective and objective data and clustering the data into patterns, the nurse generates hypotheses for nursing diagnoses based on how the patterns meet defining characteristics of a nursing diagnosis. Defining characteristics is the terminology used for observable signs and symptoms related to a nursing diagnosis. [ 21 ] Defining characteristics are included in care planning resources for each nursing diagnosis, along with a definition of that diagnosis, so the nurse can select the most accurate diagnosis. For example, objective and subjective data such as weight, height, and dietary intake can be clustered together as defining characteristics for the nursing diagnosis of nutritional status.
When creating a nursing diagnosis statement, the nurse also identifies the cause of the problem for that specific patient. Related factors is the terminology used for the underlying causes (etiology) of a patient’s problem or situation. Related factors should not be a medical diagnosis, but instead should be attributed to the underlying pathophysiology that the nurse can treat. When possible, the nursing interventions planned for each nursing diagnosis should attempt to modify or remove these related factors that are the underlying cause of the nursing diagnosis. [ 22 ]
Creating nursing diagnosis statements has traditionally been referred to as “using PES format.” The PES mnemonic no longer applies to the current terminology used by NANDA-I, but the components of a nursing diagnosis statement remain the same. A nursing diagnosis statement should contain the problem, related factors, and defining characteristics. These terms fit under the former PES format in this manner:
Problem (P) – the patient p roblem (i.e., the nursing diagnosis)
Etiology (E) – related factors (i.e., the e tiology/cause) of the nursing diagnosis; phrased as “related to” or “R/T”
Signs and Symptoms (S) – defining characteristics manifested by the patient (i.e., the s igns and s ymptoms/subjective and objective data) that led to the identification of that nursing diagnosis for the patient; phrased with “as manifested by” or “as evidenced by.”
Examples of different types of nursing diagnoses are further explained below.
Problem-Focused Nursing Diagnosis
A problem-focused nursing diagnosis contains all three components of the PES format :
Problem (P) – statement of the patient response (nursing diagnosis)
Etiology (E) – related factors contributing to the nursing diagnosis
Signs and Symptoms (S) – defining characteristics manifested by that patient
SAMPLE PROBLEM-FOCUSED NURSING DIAGNOSIS STATEMENT
Refer to Scenario C of the “Assessment” section of this chapter. The cluster of data for Ms. J. (elevated blood pressure, elevated respiratory rate, crackles in the lungs, weight gain, worsening edema, and shortness of breath) are defining characteristics for the NANDA-I Nursing Diagnosis Excess Fluid Volume . The NANDA-I definition of Excess Fluid Volume is “surplus intake and/or retention of fluid.” The related factor (etiology) of the problem is that the patient has excessive fluid intake. [ 23 ]
The components of a problem-focused nursing diagnosis statement for Ms. J. would be:
Fluid Volume Excess
Related to excessive fluid intake
As manifested by bilateral basilar crackles in the lungs, bilateral 2+ pitting edema of the ankles and feet, increased weight of 10 pounds, and the patient reports, “ My ankles are so swollen .”
A correctly written problem-focused nursing diagnosis statement for Ms. J. would look like this:
Fluid Volume Excess related to excessive fluid intake as manifested by bilateral basilar crackles in the lungs, bilateral 2+ pitting edema of the ankles and feet, an increase weight of 10 pounds, and the patient reports, “My ankles are so swollen.”
Health-Promotion Nursing Diagnosis
A health-promotion nursing diagnosis statement contains the problem (P) and the defining characteristics (S). The defining characteristics component of a health-promotion nursing diagnosis statement should begin with the phrase “expresses desire to enhance”: [ 24 ]
Signs and Symptoms (S) – the patient’s expressed desire to enhance
SAMPLE HEALTH-PROMOTION NURSING DIAGNOSIS STATEMENT
Refer to Scenario C in the “Assessment” section of this chapter. Ms. J. demonstrates a readiness to improve her health status when she told the nurse that she would like to “learn more about my health so I can take better care of myself.” This statement is a defining characteristic of the NANDA-I nursing diagnosis Readiness for Enhanced Health Management , which is defined as “a pattern of regulating and integrating into daily living a therapeutic regimen for the treatment of illness and its sequelae, which can be strengthened.” [ 25 ]
The components of a health-promotion nursing diagnosis for Ms. J. would be:
Problem (P): Readiness for Enhanced Health Management
Symptoms (S): Expressed desire to “learn more about my health so I can take better care of myself.”
A correctly written health-promotion nursing diagnosis statement for Ms. J. would look like this:
Enhanced Readiness for Health Promotion as manifested by expressed desire to “learn more about my health so I can take better care of myself.”
Risk Nursing Diagnosis
A risk nursing diagnosis should be supported by evidence of the patient’s risk factors for developing that problem. Different experts recommend different phrasing. NANDA-I 2018-2020 recommends using the phrase “as evidenced by” to refer to the risk factors for developing that problem. [ 26 ]
A risk diagnosis consists of the following:
As Evidenced By – Risk factors for developing the problem
SAMPLE RISK DIAGNOSIS STATEMENT
Refer to Scenario C in the “Assessment” section of this chapter. Ms. J. has an increased risk of falling due to vulnerability from the dizziness and weakness she is experiencing. The NANDA-I definition of Risk for Falls is “increased susceptibility to falling, which may cause physical harm and compromise health.” [ 27 ]
The components of a risk diagnosis statement for Ms. J. would be:
Problem (P) – Risk for Falls
As Evidenced By – Dizziness and decreased lower extremity strength
A correctly written risk nursing diagnosis statement for Ms. J. would look like this:
Risk for Falls as evidenced by dizziness and decreased lower extremity strength.
Syndrome Diagnosis
A syndrome is a cluster of nursing diagnoses that occur together and are best addressed together and through similar interventions. To create a syndrome diagnosis, two or more nursing diagnoses must be used as defining characteristics (S) that create a syndrome. Related factors may be used if they add clarity to the definition, but are not required. [ 28 ]
A syndrome statement consists of these items:
Problem (P) – the syndrome
Signs and Symptoms (S) – the defining characteristics are two or more similar nursing diagnoses
SAMPLE SYNDROME DIAGNOSIS STATEMENT
Refer to Scenario C in the “Assessment” section of this chapter. Clustering the data for Ms. J. identifies several similar NANDA-I nursing diagnoses that can be categorized as a syndrome . For example, Activity Intolerance is defined as “insufficient physiological or psychological energy to endure or complete required or desired daily activities.” Social Isolation is defined as “aloneness experienced by the individual and perceived as imposed by others and as a negative or threatening state.” These diagnoses can be included under the the NANDA-I syndrome named Risk for Frail Elderly Syndrome. This syndrome is defined as a “dynamic state of unstable equilibrium that affects the older individual experiencing deterioration in one or more domains of health (physical, functional, psychological, or social) and leads to increased susceptibility to adverse health effects, in particular disability.” [ 29 ]
The components of a syndrome nursing diagnosis for Ms. J. would be:
– Risk for Frail Elderly Syndrome
– The nursing diagnoses of Activity Intolerance and Social Isolation
Additional related factor: Fear of falling
A correctly written syndrome diagnosis statement for Ms. J. would look like this:
Risk for Frail Elderly Syndrome related to activity intolerance, social isolation, and fear of falling
Prioritization
After identifying nursing diagnoses, the next step is prioritization according to the specific needs of the patient. Nurses prioritize their actions while providing patient care multiple times every day. Prioritization is the process that identifies the most significant nursing problems, as well as the most important interventions, in the nursing care plan.
It is essential that life-threatening concerns and crises are identified immediately and addressed quickly. Depending on the severity of a problem, the steps of the nursing process may be performed in a matter of seconds for life-threatening concerns. In critical situations, the steps of the nursing process are performed through rapid clinical judgment. Nurses must recognize cues signaling a change in patient condition, apply evidence-based practices in a crisis, and communicate effectively with interprofessional team members. Most patient situations fall somewhere between a crisis and routine care.
There are several concepts used to prioritize, including Maslow’s Hierarchy of Needs, the “ABCs” (Airway, Breathing and Circulation), and acute, uncompensated conditions. See the infographic in Figure 4.7 [30] on The How To of Prioritization .
The How To of Prioritization
Maslow’s Hierarchy of Needs is used to categorize the most urgent patient needs. The bottom levels of the pyramid represent the top priority needs of physiological needs intertwined with safety. See Figure 4.8 [31] for an image of Maslow’s Hierarchy of Needs. You may be asking yourself, “What about the ABCs – isn’t airway the most important?” The answer to that question is “it depends on the situation and the associated safety considerations.” Consider this scenario – you are driving home after a lovely picnic in the country and come across a fiery car crash. As you approach the car, you see that the passenger is not breathing. Using Maslow’s Hierarchy of Needs to prioritize your actions, you remove the passenger from the car first due to safety even though he is not breathing. After ensuring safety and calling for help, you follow the steps to perform cardiopulmonary resuscitation (CPR) to establish circulation, airway, and breathing until help arrives.
Maslow’s Hierarchy of Needs
In addition to using Maslow’s Hierarchy of Needs and the ABCs of airway, breathing, and circulation, the nurse also considers if the patient’s condition is an acute or chronic problem. Acute, uncompensated conditions generally require priority interventions over chronic conditions. Additionally, actual problems generally receive priority over potential problems, but risk problems sometimes receive priority depending on the patient vulnerability and risk factors.
Example. Refer to Scenario C in the “Assessment” section of this chapter. Four types of nursing diagnoses were identified for Ms. J.: Fluid Volume Excess, Enhanced Readiness for Health Promotion, Risk for Falls , and Risk for Frail Elderly Syndrome . The top priority diagnosis is Fluid Volume Excess because it affects the physiological needs of breathing, homeostasis, and excretion. However, the Risk for Falls diagnosis comes in a close second because of safety implications and potential injury that could occur if the patient fell.
American Nurses Association. (2021). Nursing: Scope and standards of practice (4th ed.). American Nurses Association. ↵
Herdman, T. H., & Kamitsuru, S. (Eds.). (2018). Nursing diagnoses: Definitions and classification, 2018-2020 . Thieme Publishers New York. ↵
Herdman, T. H., & Kamitsuru, S. (Eds.). (2018). Nursing diagnoses: Definitions and classification, 2018-2020. Thieme Publishers New York. ↵
Gordon, M. (2008). Assess notes: Nursing assessment and diagnostic reasoning. F.A. Davis Company. ↵
NANDA International. (n.d.). Glossary of terms . https://nanda .org/nanda-i-resources /glossary-of-terms / ↵
NANDA International. (n.d.). Glossary of terms . https://nanda .org/nanda-i-resources /glossary-of-terms/ ↵
NANDA International. (n.d.). Glossary of terms. https://nanda .org/nanda-i-resources /glossary-of-terms/ ↵
“The How To of Prioritization” by Valerie Palarski for Chippewa Valley Technical College is licensed under CC BY 4.0 ↵
“ Maslow's hierarchy of needs.svg ” by J. Finkelstein is licensed under CC BY-SA 3.0 ↵
4.5. OUTCOME IDENTIFICATION
Outcome Identification is the third step of the nursing process (and the third Standard of Practice set by the American Nurses Association). This standard is defined as, “The registered nurse identifies expected outcomes for a plan individualized to the health care consumer or the situation.” The RN collaborates with the health care consumer, interprofessional team, and others to identify expected outcomes integrating the health care consumer’s culture, values, and ethical considerations. Expected outcomes are documented as measurable goals with a time frame for attainment. [ 1 ]
An outcome is a “measurable behavior demonstrated by the patient responsive to nursing interventions.” [ 2 ] Outcomes should be identified before nursing interventions are planned. After nursing interventions are implemented, the nurse will evaluate if the outcomes were met in the time frame indicated for that patient.
Outcome identification includes setting short- and long-term goals and then creating specific expected outcome statements for each nursing diagnosis.
Short-Term and Long-Term Goals
Nursing care should always be individualized and patient-centered. No two people are the same, and neither should nursing care plans be the same for two people. Goals and outcomes should be tailored specifically to each patient’s needs, values, and cultural beliefs. Patients and family members should be included in the goal-setting process when feasible. Involving patients and family members promotes awareness of identified needs, ensures realistic goals, and motivates their participation in the treatment plan to achieve the mutually agreed upon goals and live life to the fullest with their current condition.
The nursing care plan is a road map used to guide patient care so that all health care providers are moving toward the same patient goals. Goals are broad statements of purpose that describe the overall aim of care. Goals can be short- or long-term. The time frame for short- and long-term goals is dependent on the setting in which the care is provided. For example, in a critical care area, a short-term goal might be set to be achieved within an 8-hour nursing shift, and a long-term goal might be in 24 hours. In contrast, in an outpatient setting, a short-term goal might be set to be achieved within one month and a long-term goal might be within six months.
A nursing goal is the overall direction in which the patient must progress to improve the problem/nursing diagnosis and is often the opposite of the problem.
Example. Refer to Scenario C in the “Assessment” section of this chapter. Ms. J. had a priority nursing diagnosis of Fluid Volume Excess. A broad goal would be, “ Ms. J. will achieve a state of fluid balance. ”
Expected Outcomes
Goals are broad, general statements, but outcomes are specific and measurable. Expected outcomes are statements of measurable action for the patient within a specific time frame that are responsive to nursing interventions. Nurses may create expected outcomes independently or refer to classification systems for assistance. Just as NANDA-I creates and revises standardized nursing diagnoses, a similar classification and standardization process exists for expected nursing outcomes. The Nursing Outcomes Classification (NOC) is a list of over 330 nursing outcomes designed to coordinate with established NANDA-I diagnoses. [ 3 ]
Patient-Centered
Outcome statements are always patient-centered. They should be developed in collaboration with the patient and individualized to meet a patient’s unique needs, values, and cultural beliefs. They should start with the phrase “The patient will…” Outcome statements should be directed at resolving the defining characteristics for that nursing diagnosis. Additionally, the outcome must be something the patient is willing to cooperate in achieving.
Outcome statements should contain five components easily remembered using the “SMART” mnemonic: [ 4 ]
- M easurable
- A ttainable/Action oriented
- R elevant/Realistic
See Figure 4.9 [ 5 ] for an image of the SMART components of outcome statements. Each of these components is further described in the following subsections.
SMART Components of Outcome Statements
Outcome statements should state precisely what is to be accomplished. See the following examples:
- Not specific: “The patient will increase the amount of exercise.”
- Specific: “The patient will participate in a bicycling exercise session daily for 30 minutes.”
Additionally, only one action should be included in each expected outcome. See the following examples:
- “The patient will walk 50 feet three times a day with standby assistance of one and will shower in the morning until discharge” is actually two goals written as one. The outcome of ambulation should be separate from showering for precise evaluation. For instance, the patient could shower but not ambulate, which would make this outcome statement very difficult to effectively evaluate.
- Suggested revision is to create two outcomes statements so each can be measured: The patient will walk 50 feet three times a day with standby assistance of one until discharge. The patient will shower every morning until discharge.
Measurable outcomes have numeric parameters or other concrete methods of judging whether the outcome was met. It is important to use objective data to measure outcomes. If terms like “acceptable” or “normal” are used in an outcome statement, it is difficult to determine whether the outcome is attained. Refer to Figure 4.10 [ 6 ] for examples of verbs that are measurable and not measurable in outcome statements.
Figure 4.10
Measurable Outcomes
See the following examples:
- Not measurable: “The patient will drink adequate fluid amounts every shift.”
- Measurable: “The patient will drink 24 ounces of fluids during every day shift (0600-1400).”
Action-Oriented and Attainable
Outcome statements should be written so that there is a clear action to be taken by the patient or significant others. This means that the outcome statement should include a verb. Refer to Figure 4.11 [ 7 ] for examples of action verbs.
Figure 4.11
Action Verbs
- Not action-oriented: “The patient will get increased physical activity.”
- Action-oriented: “The patient will list three types of aerobic activity that he would enjoy completing every week.”
Realistic and Relevant
Realistic outcomes consider the patient’s physical and mental condition; their cultural and spiritual values, beliefs, and preferences; and their socioeconomic status in terms of their ability to attain these outcomes. Consideration should be also given to disease processes and the effects of conditions such as pain and decreased mobility on the patient’s ability to reach expected outcomes. Other barriers to outcome attainment may be related to health literacy or lack of available resources. Outcomes should always be reevaluated and revised for attainability as needed. If an outcome is not attained, it is commonly because the original time frame was too ambitious or the outcome was not realistic for the patient.
- Not realistic: “The patient will jog one mile every day when starting the exercise program.”
- Realistic: “The patient will walk ½ mile three times a week for two weeks.”
Time Limited
Outcome statements should include a time frame for evaluation. The time frame depends on the intervention and the patient’s current condition. Some outcomes may need to be evaluated every shift, whereas other outcomes may be evaluated daily, weekly, or monthly. During the evaluation phase of the nursing process, the outcomes will be assessed according to the time frame specified for evaluation. If it has not been met, the nursing care plan should be revised.
- Not time limited: “The patient will stop smoking cigarettes.”
- Time limited: “The patient will complete the smoking cessation plan by December 12, 2021.”
In Scenario C in Box 4.3, Ms. J.’s priority nursing diagnosis statement was Fluid Volume Excess related to excess fluid intake as manifested by bilateral basilar crackles in the lungs, bilateral 2+ pitting edema of the ankles and feet, an increase weight of 10 pounds, and the patient reports, “My ankles are so swollen.” An example of an expected outcome meeting SMART criteria for Ms. J. is, “The patient will have clear bilateral lung sounds within the next 24 hours.”
4.6. PLANNING
Planning is the fourth step of the nursing process (and the fourth Standard of Practice set by the American Nurses Association). This standard is defined as, “The registered nurse develops a collaborative plan encompassing strategies to achieve expected outcomes.” The RN develops an individualized, holistic, evidence-based plan in partnership with the health care consumer, family, significant others, and interprofessional team. Elements of the plan are prioritized. The plan is modified according to the ongoing assessment of the health care consumer’s response and other indicators. The plan is documented using standardized language or terminology. [ 1 ]
After expected outcomes are identified, the nurse begins planning nursing interventions to implement. Nursing interventions are evidence-based actions that the nurse performs to achieve patient outcomes. Just as a provider makes medical diagnoses and writes prescriptions to improve the patient’s medical condition, a nurse formulates nursing diagnoses and plans nursing interventions to resolve patient problems. Nursing interventions should focus on eliminating or reducing the related factors (etiology) of the nursing diagnoses when possible. [ 2 ] Nursing interventions, goals, and expected outcomes are written in the nursing care plan for continuity of care across shifts, nurses, and health professionals.
Planning Nursing Interventions
You might be asking yourself, “How do I know what evidence-based nursing interventions to include in the nursing care plan?” There are several sources that nurses and nursing students can use to select nursing interventions. Many agencies have care planning tools and references included in the electronic health record that are easily documented in the patient chart. Nurses can also refer to other care planning books our sources such as the Nursing Interventions Classification (NIC) system. Based on research and input from the nursing profession, NIC categorizes and describes nursing interventions that are constantly evaluated and updated. Interventions included in NIC are considered evidence-based nursing practices. The nurse is responsible for using clinical judgment to make decisions about which interventions are best suited to meet an individualized patient’s needs. [ 3 ]
Direct and Indirect Care
Nursing interventions are considered direct care or indirect care. Direct care refers to interventions that are carried out by having personal contact with patients. Examples of direct care interventions are wound care, repositioning, and ambulation. Indirect care interventions are performed when the nurse provides assistance in a setting other than with the patient. Examples of indirect care interventions are attending care conferences, documenting, and communicating about patient care with other providers.
Classification of Nursing Interventions
There are three types of nursing interventions: independent, dependent, and collaborative. (See Figure 4.12 [ 4 ] for an image of a nurse collaborating with the health care team when planning interventions.)
Figure 4.12
Collaborative nursing interventions, independent nursing interventions.
Any intervention that the nurse can independently provide without obtaining a prescription is considered an independent nursing intervention . An example of an independent nursing intervention is when the nurses monitor the patient’s 24-hour intake/output record for trends because of a risk for imbalanced fluid volume. Another example of independent nursing interventions is the therapeutic communication that a nurse uses to assist patients to cope with a new medical diagnosis.
Example. Refer to Scenario C in the “Assessment” section of this chapter. Ms. J. was diagnosed with Fluid Volume Excess . An example of an evidence-based independent nursing intervention is, “The nurse will reposition the patient with dependent edema frequently, as appropriate.” [ 5 ] The nurse would individualize this evidence-based intervention to the patient and agency policy by stating, “The nurse will reposition the patient every 2 hours.”
Dependent Nursing Interventions
Dependent nursing interventions require a prescription before they can be performed. Prescriptions are orders, interventions, remedies, or treatments ordered or directed by an authorized primary health care provider. [ 6 ] A primary health care provider is a member of the health care team (usually a physician, advanced practice nurse, or physician’s assistant) who is licensed and authorized to formulate prescriptions on behalf of the client. For example, administering medication is a dependent nursing intervention. The nurse incorporates dependent interventions into the patient’s overall care plan by associating each intervention with the appropriate nursing diagnosis.
Example. Refer to Scenario C in the “Assessment” section of this chapter. Ms. J. was diagnosed with Fluid Volume Excess . An example of a dependent nursing intervention is, “The nurse will administer scheduled diuretics as prescribed.”
Collaborative nursing interventions are actions that the nurse carries out in collaboration with other health team members, such as physicians, social workers, respiratory therapists, physical therapists, and occupational therapists. These actions are developed in consultation with other health care professionals and incorporate their professional viewpoint. [ 7 ]
Example. Refer to Scenario C in the “Assessment” section of this chapter. Ms. J. was diagnosed with Fluid Volume Excess . An example of a collaborative nursing intervention is consulting with a respiratory therapist when the patient has deteriorating oxygen saturation levels. The respiratory therapist plans oxygen therapy and obtains a prescription from the provider. The nurse would document “ The nurse will manage oxygen therapy in collaboration with the respiratory therapist ” in the care plan.
Individualization of Interventions
It is vital for the planned interventions to be individualized to the patient to be successful. For example, adding prune juice to the breakfast meal of a patient with constipation will only work if the patient likes to drink the prune juice. If the patient does not like prune juice, then this intervention should not be included in the care plan. Collaboration with the patient, family members, significant others, and the interprofessional team is essential for selecting effective interventions. The number of interventions included in a nursing care plan is not a hard and fast rule, but enough quality, individualized interventions should be planned to meet the identified outcomes for that patient.
Creating Nursing Care Plans
Nursing care plans are created by registered nurses (RNs). Documentation of individualized nursing care plans are legally required in long-term care facilities by the Centers for Medicare and Medicaid Services (CMS) and in hospitals by The Joint Commission. CMS guidelines state, “Residents and their representative(s) must be afforded the opportunity to participate in their care planning process and to be included in decisions and changes in care, treatment, and/or interventions. This applies both to initial decisions about care and treatment, as well as the refusal of care or treatment. Facility staff must support and encourage participation in the care planning process. This may include ensuring that residents, families, or representatives understand the comprehensive care planning process, holding care planning meetings at the time of day when a resident is functioning best and patient representatives can be present, providing sufficient notice in advance of the meeting, scheduling these meetings to accommodate a resident’s representative (such as conducting the meeting in-person, via a conference call, or video conferencing), and planning enough time for information exchange and decision-making. A resident has the right to select or refuse specific treatment options before the care plan is instituted.” [ 8 ] The Joint Commission conceptualizes the care planning process as the structuring framework for coordinating communication that will result in safe and effective care. [ 9 ]
Many facilities have established standardized nursing care plans with lists of possible interventions that can be customized for each specific patient. Other facilities require the nurse to develop each care plan independently. Whatever the format, nursing care plans should be individualized to meet the specific and unique needs of each patient. See Figure 4.13 [ 10 ] for an image of a standardized care plan.
Figure 4.13
Standardized Care Plan
Nursing care plans created in nursing school can also be in various formats such as concept maps or tables. Some are fun and creative, while others are more formal. Appendix B contains a template that can be used for creating nursing care plans.
4.7. IMPLEMENTATION OF INTERVENTIONS
Implementation is the fifth step of the nursing process (and the fifth Standard of Practice set by the American Nurses Association). This standard is defined as, “The registered nurse implements the identified plan.” The RN may delegate planned interventions after considering the circumstance, person, task, communication, supervision, and evaluation, as well as the state Nurse Practice Act, federal regulation, and agency policy. [ 1 ]
Implementation of interventions requires the RN to use critical thinking and clinical judgment. After the initial plan of care is developed, continual reassessment of the patient is necessary to detect any changes in the patient’s condition requiring modification of the plan. The need for continual patient reassessment underscores the dynamic nature of the nursing process and is crucial to providing safe care.
During the implementation phase of the nursing process, the nurse prioritizes planned interventions, assesses patient safety while implementing interventions, delegates interventions as appropriate, and documents interventions performed.
Prioritizing Implementation of Interventions
Prioritizing implementation of interventions follows a similar method as to prioritizing nursing diagnoses. Maslow’s Hierarchy of Needs and the ABCs of airway, breathing, and circulation are used to establish top priority interventions. When possible, least invasive actions are usually preferred due to the risk of injury from invasive options. Read more about methods for prioritization under the “ Diagnosis ” subsection of this chapter.
The potential impact on future events, especially if a task is not completed at a certain time, is also included when prioritizing nursing interventions. For example, if a patient is scheduled to undergo a surgical procedure later in the day, the nurse prioritizes initiating a NPO (nothing by mouth) prescription prior to completing pre-op patient education about the procedure. The rationale for this decision is that if the patient ate food or drank water, the surgery time would be delayed. Knowing and understanding the patient’s purpose for care, current situation, and expected outcomes are necessary to accurately prioritize interventions.
Patient Safety
It is essential to consider patient safety when implementing interventions. At times, patients may experience a change in condition that makes a planned nursing intervention or provider prescription no longer safe to implement. For example, an established nursing care plan for a patient states, “The nurse will ambulate the patient 100 feet three times daily.” However, during assessment this morning, the patient reports feeling dizzy today, and their blood pressure is 90/60. Using critical thinking and clinical judgment, the nurse decides to not implement the planned intervention of ambulating the patient. This decision and supporting assessment findings should be documented in the patient’s chart and also communicated during the shift handoff report, along with appropriate notification of the provider of the patient’s change in condition.
Implementing interventions goes far beyond implementing provider prescriptions and completing tasks identified on the nursing care plan and must focus on patient safety. As front-line providers, nurses are in the position to stop errors before they reach the patient. [ 2 ]
In 2000 the Institute of Medicine (IOM) issued a groundbreaking report titled To Err Is Human: Building a Safer Health System . The report stated that as many as 98,000 people die in U.S. hospitals each year as a result of preventable medical errors. To Err Is Human broke the silence that previously surrounded the consequences of medical errors and set a national agenda for reducing medical errors and improving patient safety through the design of a safer health system. [ 3 ] In 2007 the IOM published a follow-up report titled Preventing Medication Errors and reported that more than 1.5 million Americans are injured every year in American hospitals, and the average hospitalized patient experiences at least one medication error each day. This report emphasized actions that health care systems could take to improve medication safety. [ 4 ]
Read additional information about specific actions that nurses can take to prevent medication errors; go to the “Preventing Medication Errors” section of the “ Legal/Ethical” chapter of the Open RN Nursing Pharmacology textbook.
In an article released by the Robert Wood Johnson Foundation, errors involving nurses that endanger patient safety cover broad territory. This territory spans “wrong site, wrong patient, wrong procedure” errors, medication mistakes, failures to follow procedures that prevent central line bloodstream and other infections, errors that allow unsupervised patients to fall, and more. Some errors can be traced to shifts that are too long that leave nurses fatigued, some result from flawed systems that do not allow for adequate safety checks, and others are caused by interruptions to nurses while they are trying to administer medications or provide other care. [ 5 ]
The Quality and Safety Education for Nurses (QSEN) project began in 2005 to assist in preparing future nurses to continuously improve the quality and safety of the health care systems in which they work. The vision of the QSEN project is to “inspire health care professionals to put quality and safety as core values to guide their work.” [ 6 ] Nurses and nursing students are expected to participate in quality improvement (QI) initiatives by identifying gaps where change is needed and assisting in implementing initiatives to resolve these gaps. Quality improvement is defined as, “The combined and unceasing efforts of everyone – health care professionals, patients and their families, researchers, payers, planners and educators – to make the changes that will lead to better patient outcomes (health), better system performance (care), and better professional development (learning).” [ 7 ]
Delegation of Interventions
While implementing interventions, RNs may elect to delegate nursing tasks. Delegation is defined by the American Nurses Association as, “The assignment of the performance of activities or tasks related to patient care to unlicensed assistive personnel or licensed practical nurses (LPNs) while retaining accountability for the outcome.” [ 8 ] RNs are accountable for determining the appropriateness of the delegated task according to condition of the patient and the circumstance; the communication provided to an appropriately trained LPN or UAP; the level of supervision provided; and the evaluation and documentation of the task completed. The RN must also be aware of the state Nurse Practice Act, federal regulations, and agency policy before delegating. The RN cannot delegate responsibilities requiring clinical judgment. [ 9 ] See the following box for information regarding legal requirements associated with delegation according to the Wisconsin Nurse Practice Act.
Delegation According to the Wisconsin Nurse Practice Act
During the supervision and direction of delegated acts a Registered Nurse shall do all of the following:
Delegate tasks commensurate with educational preparation and demonstrated abilities of the person supervised.
Provide direction and assistance to those supervised.
Observe and monitor the activities of those supervised.
Evaluate the effectiveness of acts performed under supervision. [ 10 ]
The standard of practice for Licensed Practical Nurses in Wisconsin states, “In the performance of acts in basic patient situations, the LPN. shall, under the general supervision of an RN or the direction of a provider:
Accept only patient care assignments which the LPN is competent to perform.
Provide basic nursing care. Basic nursing care is defined as care that can be performed following a defined nursing procedure with minimal modification in which the responses of the patient to the nursing care are predictable.
Record nursing care given and report to the appropriate person changes in the condition of a patient.
Consult with a provider in cases where an LPN knows or should know a delegated act may harm a patient.
Perform the following other acts when applicable:
Assist with the collection of data.
Assist with the development and revision of a nursing care plan.
Reinforce the teaching provided by an RN provider and provide basic health care instruction.
Participate with other health team members in meeting basic patient needs.” [ 11 ]
Read additional details about the scope of practice of registered nurses (RNs) and licensed practical nurses (LPNs) in Wisconsin’s Nurse Practice Act in Chapter N 6 Standards of Practice .
Read more about the American Nurses Association’s Principles of Delegation.
Table 4.7 outlines general guidelines for delegating nursing tasks in the state of Wisconsin according to the role of the health care team member.
General Guidelines for Delegating Nursing Tasks
Documentation of Interventions
As interventions are performed, they must be documented in the patient’s record in a timely manner. As previously discussed in the “Ethical and Legal Issues” subsection of the “ Basic Concepts ” section, lack of documentation is considered a failure to communicate and a basis for legal action. A basic rule of thumb is if an intervention is not documented, it is considered not done in a court of law. It is also important to document administration of medication and other interventions in a timely manner to prevent errors that can occur due to delayed documentation time.
Coordination of Care and Health Teaching/Health Promotion
ANA’s Standard of Professional Practice for Implementation also includes the standards 5A Coordination of Care and 5B Health Teaching and Health Promotion . [ 12 ] Coordination of Care includes competencies such as organizing the components of the plan, engaging the patient in self-care to achieve goals, and advocating for the delivery of dignified and holistic care by the interprofessional team. Health Teaching and Health Promotion is defined as, “Employing strategies to teach and promote health and wellness.” [ 13 ] Patient education is an important component of nursing care and should be included during every patient encounter. For example, patient education may include teaching about side effects while administering medications or teaching patients how to self-manage their conditions at home.
Refer to Scenario C in the “Assessment” section of this chapter. The nurse implemented the nursing care plan documented in Appendix C. Interventions related to breathing were prioritized. Administration of the diuretic medication was completed first, and lung sounds were monitored frequently for the remainder of the shift. Weighing the patient before breakfast was delegated to the CNA. The patient was educated about her medications and methods to use to reduce peripheral edema at home. All interventions were documented in the electronic medical record (EMR).
4.8. EVALUATION
Evaluation is the sixth step of the nursing process (and the sixth Standard of Practice set by the American Nurses Association). This standard is defined as, “The registered nurse evaluates progress toward attainment of goals and outcomes.” [ 1 ] Both the patient status and the effectiveness of the nursing care must be continuously evaluated and the care plan modified as needed. [ 2 ]
Evaluation focuses on the effectiveness of the nursing interventions by reviewing the expected outcomes to determine if they were met by the time frames indicated. During the evaluation phase, nurses use critical thinking to analyze reassessment data and determine if a patient’s expected outcomes have been met, partially met, or not met by the time frames established. If outcomes are not met or only partially met by the time frame indicated, the care plan should be revised. Reassessment should occur every time the nurse interacts with a patient, discusses the care plan with others on the interprofessional team, or reviews updated laboratory or diagnostic test results. Nursing care plans should be updated as higher priority goals emerge. The results of the evaluation must be documented in the patient’s medical record.
Ideally, when the planned interventions are implemented, the patient will respond positively and the expected outcomes are achieved. However, when interventions do not assist in progressing the patient toward the expected outcomes, the nursing care plan must be revised to more effectively address the needs of the patient. These questions can be used as a guide when revising the nursing care plan:
- Did anything unanticipated occur?
- Has the patient’s condition changed?
- Were the expected outcomes and their time frames realistic?
- Are the nursing diagnoses accurate for this patient at this time?
- Are the planned interventions appropriately focused on supporting outcome attainment?
- What barriers were experienced as interventions were implemented?
- Does ongoing assessment data indicate the need to revise diagnoses, outcome criteria, planned interventions, or implementation strategies?
- Are different interventions required?
Refer to Scenario C in the “Assessment” section of this chapter and Appendix C . The nurse evaluates the patient’s progress toward achieving the expected outcomes.
For the nursing diagnosis Fluid Volume Excess , the nurse evaluated the four expected outcomes to determine if they were met during the time frames indicated:
The patient will report decreased dyspnea within the next 8 hours.
The patient will have clear lung sounds within the next 24 hours.
The patient will have decreased edema within the next 24 hours.
The patient’s weight will return to baseline by discharge.
Evaluation of the patient condition on Day 1 included the following data: “ The patient reported decreased shortness of breath, and there were no longer crackles in the lower bases of the lungs. Weight decreased by 1 kg, but 2+ edema continued in ankles and calves .” Based on this data, the nurse evaluated the expected outcomes as “ Partially Met ” and revised the care plan with two new interventions:
Request prescription for TED hose from provider.
Elevate patient’s legs when sitting in chair.
For the second nursing diagnosis, Risk for Falls , the nurse evaluated the outcome criteria as “ Met ” based on the evaluation, “ The patient verbalizes understanding and is appropriately calling for assistance when getting out of bed. No falls have occurred. ”
The nurse will continue to reassess the patient’s progress according to the care plan during hospitalization and make revisions to the care plan as needed. Evaluation of the care plan is documented in the patient’s medical record.
4.9. SUMMARY OF THE NURSING PROCESS
You have now learned how to perform each step of the nursing process according to the ANA Standards of Professional Nursing Practice. Critical thinking, clinical reasoning, and clinical judgment are used when assessing the patient, creating a nursing care plan, and implementing interventions. Frequent reassessment, with revisions to the care plan as needed, is important to help the patient achieve expected outcomes. Throughout the entire nursing process, the patient always remains the cornerstone of nursing care. Providing individualized, patient-centered care and evaluating whether that care has been successful in achieving patient outcomes are essential for providing safe, professional nursing practice.
Video Review of Creating a Sample Care Plan [ 1 ]

4.10. LEARNING ACTIVITIES
Learning activities.
(Answers to “Learning Activities” can be found in the “Answer Key” at the end of the book. Answers to interactive activity elements will be provided within the element as immediate feedback.)
Instructions: Apply what you’ve learned in this chapter by creating a nursing care plan using the following scenario. Use the template in Appendix B as a guide.
The client, Mark S., is a 57-year-old male who was admitted to the hospital with “severe” abdominal pain that was unable to be managed in the Emergency Department. The physician has informed Mark that he will need to undergo some diagnostic tests. The tests are scheduled for the morning.
After receiving the news about his condition and the need for diagnostic tests, Mark begins to pace the floor. He continues to pace constantly. He keeps asking the nurse the same question (“How long will the tests take?”) about his tests over and over again. The patient also remarked, “I’m so uptight I will never be able to sleep tonight.” The nurse observes that the client avoids eye contact during their interactions and that he continually fidgets with the call light. His eyes keep darting around the room. He appears tense and has a strained expression on his face. He states, “My mouth is so dry.” The nurse observes his vital signs to be: T 98, P 104, R 30, BP 180/96. The nurse notes that his skin feels sweaty (diaphoretic) and cool to the touch.
Critical Thinking Activity:
Group (cluster) the subjective and objective data.
Create a problem-focused nursing diagnosis (hypothesis).
Develop a broad goal and then identify an expected outcome in “SMART” format.
Outline three interventions for the nursing diagnosis to meet the goal. Cite an evidence-based source.
Imagine that you implemented the interventions that you identified. Evaluate the degree to which the expected outcome was achieved: Met – Partially Met – Not Met.

- IV GLOSSARY
The act or process of pleading for, supporting, or recommending a cause or course of action. [ 1 ]
Unconditionally acceptance of the humanity of others, respecting their need for dignity and worth, while providing compassionate, comforting care. [ 2 ]
Groups of people who share a characteristic that causes each member to be susceptible to a particular human response, such as demographics, health/family history, stages of growth/development, or exposure to certain events/experiences. [ 3 ]
Medical diagnoses, injuries, procedures, medical devices, or pharmacological agents. These conditions are not independently modifiable by the nurse, but support accuracy in nursing diagnosis. [ 4 ]
Care that can be performed following a defined nursing procedure with minimal modification in which the responses of the patient to the nursing care are predictable. [ 5 ]
A relationship described as one in which the whole person is assessed while balancing the vulnerability and dignity of the patient and family. [ 6 ]
Individual, family, or group, which includes significant others and populations. [ 7 ]
The observed outcome of critical thinking and decision-making. It is an iterative process that uses nursing knowledge to observe and access presenting situations, identify a prioritized client concern, and generate the best possible evidence-based solutions in order to deliver safe client care. [ 8 ]
A complex cognitive process that uses formal and informal thinking strategies to gather and analyze patient information, evaluate the significance of this information, and weigh alternative actions. [ 9 ]
Grouping data into similar domains or patterns.
Nursing interventions that require cooperation among health care professionals and unlicensed assistive personnel (UAP).
While implementing interventions during the nursing process, includes components such as organizing the components of the plan with input from the health care consumer, engaging the patient in self-care to achieve goals, and advocating for the delivery of dignified and person-centered care by the interprofessional team. [ 10 ]
Reasoning about clinical issues such as teamwork, collaboration, and streamlining workflow. [ 11 ]
Subjective or objective data that gives the nurse a hint or indication of a potential problem, process, or disorder.
“Top-down thinking” or moving from the general to the specific. Deductive reasoning relies on a general statement or hypothesis—sometimes called a premise or standard—that is held to be true. The premise is used to reach a specific, logical conclusion.
Observable cues/inferences that cluster as manifestations of a problem-focused, health-promotion diagnosis, or syndrome. This does not only imply those things that the nurse can see, but also things that are seen, heard (e.g., the patient/family tells us), touched, or smelled. [ 12 ]
The assignment of the performance of activities or tasks related to patient care to unlicensed assistive personnel while retaining accountability for the outcome. [ 13 ]
Interventions that require a prescription from a physician, advanced practice nurse, or physician’s assistant.
Interventions that are carried out by having personal contact with a patient.
An electronic version of the patient’s medical record.
A lifelong problem-solving approach that integrates the best evidence from well-designed research studies and evidence-based theories; clinical expertise and evidence from assessment of the health care consumer’s history and condition, as well as health care resources; and patient, family, group, community, and population preferences and values. [ 14 ]
Statements of measurable action for the patient within a specific time frame and in response to nursing interventions. “SMART” outcome statements are specific, measurable, action-oriented, realistic, and include a time frame.
An evidence-based assessment framework for identifying patient problems and risks during the assessment phase of the nursing process.
A judgment formed from a set of facts, cues, and observations.
Broad statements of purpose that describe the aim of nursing care.
Employing strategies to teach and promote health and wellness. [ 15 ]
Any intervention that the nurse can provide without obtaining a prescription or consulting anyone else.
Interventions performed by the nurse in a setting other than directly with the patient. An example of indirect care is creating a nursing care plan.
A type of reasoning that involves forming generalizations based on specific incidents.
Interpretations or conclusions based on cues, personal experiences, preferences, or generalizations.
Nurses who have had specific training and passed a licensing exam. The training is generally less than that of a Registered Nurse. The scope of practice of an LPN/LVN is determined by the facility and the state’s Nurse Practice Act.
A disease or illness diagnosed by a physician or advanced health care provider such as a nurse practitioner or physician’s assistant. Medical diagnoses are a result of clustering signs and symptoms to determine what is medically affecting an individual.
Nursing integrates the art and science of caring and focuses on the protection, promotion, and optimization of health and human functioning; prevention of illness and injury; facilitation of healing; and alleviation of suffering through compassionate presence. Nursing is the diagnosis and treatment of human responses and advocacy in the care of individuals, families, groups, communities, and populations in the recognition of the connection of all humanity. [ 16 ]
Specific documentation of the planning and delivery of nursing care that is required by The Joint Commission.
A systematic approach to patient-centered care with steps including assessment, diagnosis, outcome identification, planning, implementation, and evaluation; otherwise known by the mnemonic “ADOPIE.”
Data that the nurse can see, touch, smell, or hear or is reproducible such as vital signs. Laboratory and diagnostic results are also considered objective data.
A measurable behavior demonstrated by the patient that is responsive to nursing interventions. [ 17 ]
The format of a nursing diagnosis statement that includes:
Problem (P) – statement of the patient problem (i.e., the nursing diagnosis)
Etiology (E) – related factors (etiology) contributing to the cause of the nursing diagnosis
Signs and Symptoms (S) – defining characteristics manifested by the patient of that nursing diagnosis
Orders, interventions, remedies, or treatments ordered or directed by an authorized primary health care provider. [ 18 ]
Information collected from the patient.
Member of the health care team (usually a medical physician, nurse practitioner, etc.) licensed and authorized to formulate prescriptions on behalf of the client. [ 19 ]
The skillful process of deciding which actions to complete first, second, or third for optimal patient outcomes and to improve patient safety.
The “combined and unceasing efforts of everyone — health care professionals, patients and their families, researchers, payers, planners, and educators — to make the changes that will lead to better patient outcomes (health), better system performance (care), and better professional development (learning).” [ 20 ]
Developing a relationship of mutual trust and understanding.
A nurse who has had a designated amount of education and training in nursing and is licensed by a state Board of Nursing.
The underlying cause (etiology) of a nursing diagnosis when creating a PES statement.
Patients have the right to determine what will be done with and to their own person.
Principles and procedures in the discovery of knowledge involving the recognition and formulation of a problem, the collection of data, and the formulation and testing of a hypothesis.
Information collected from sources other than the patient.
Data that the patient or family reports or data that the nurse makes as an inference, conclusion, or assumption, such as “The patient appears anxious.”
Any unlicensed personnel trained to function in a supportive role, regardless of title, to whom a nursing responsibility may be delegated. [ 21 ]
Obtaining Subjective Data in a Care Relationship
Licensed under a Creative Commons Attribution 4.0 International License. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/ .
- Cite this Page Open Resources for Nursing (Open RN); Ernstmeyer K, Christman E, editors. Nursing Fundamentals [Internet]. Eau Claire (WI): Chippewa Valley Technical College; 2021. Chapter 4 Nursing Process.
- PDF version of this title (216M)
In this Page
- NURSING PROCESS INTRODUCTION
- BASIC CONCEPTS
- OUTCOME IDENTIFICATION
- IMPLEMENTATION OF INTERVENTIONS
- SUMMARY OF THE NURSING PROCESS
- LEARNING ACTIVITIES
Other titles in this collection
- Open RN OER Textbooks
Related Items in Bookshelf
- All Textbooks
Bulk Download
- Bulk download content from FTP
Related information
- PMC PubMed Central citations
- PubMed Links to PubMed
Recent Activity
- Chapter 4 Nursing Process - Nursing Fundamentals Chapter 4 Nursing Process - Nursing Fundamentals
Your browsing activity is empty.
Activity recording is turned off.
Turn recording back on
Connect with NLM
National Library of Medicine 8600 Rockville Pike Bethesda, MD 20894
Web Policies FOIA HHS Vulnerability Disclosure
Help Accessibility Careers
How to develop a solid hypothesis in a nursing paper?

The hypothesis is an integral part of any research paper. It is especially important in nursing essays where students have to put forth their arguments in a logical way. With a solid hypothesis, you can provide insight into the topic in a myriad of ways
But before we get into the technicalities of the subject, let’s clear a few essential points first. What is the hypothesis? And why do we need them? Well, a hypothesis is a statement used to highlight a research question and propose an appropriate solution for it.
The primary feature of any hypothesis is that is must be testable. Your entire nursing paper develops on either trying to prove or disprove this first statement. Read on to know more about hypothesis development and how to integrate it in your essay.

Elements of a testable hypothesis
A simple hypothesis has the following parts- cause, effect, and rationale. The purpose refers to problem statement that leads to the thesis. It forms the “if” part of the hypothesis, the premise upon which you base your argument. This section should come first in the hypothesis statement wherein you explain the purpose of the research
The “effect” forms the “then” aspect of the report. In layman terms, this section refers to the consequences of probable results that follow the causes. We can also understand the effect as the solution to the problem posed by the “cause.”
The rationale is the most critical part of the hypothesis, wherein you rationally defend your arguments. This is the section where you try to prove or disprove your theory, thereby elaborating on the key points of your research.
Structuring your hypothesis
The hypothesis forms the crux of any nursing essay or scientific research, for that matter. It comes at the very beginning of your paper, even before the introduction para. It sets your research in a specific context, giving you the space to outline the intent and purpose of the article.
Every hypothesis consists of two elements- facts and variables. Facts refer to the unchanging facts and figures in the nursing essay. This information referred to in “Facts” remain constant throughout the piece. With variables, you can change the data as an when necessary. The variable data also apply to assumptions that we take before beginning any nursing paper.
Furthermore, the variables can be divided into two categories- dependent and independent. Independent variables are separate entities in their own right or the cause. The depended variables refer to the effect.
Here is a stepwise guide to structure your hypothesis .
Step 1: Theory construction
Theory construction is the first step to building the hypothesis. This is where you decide upon the topic of research and the various sources used for the study. The scientific enquiry is also the part where you check the credibility of the information presented.
There are various topics that you can base your nursing essay on. Most research papers take a specific case/instance, which can be either real or fictional. Here are a few questions you should ask before arriving at the hypothesis .
- What subject or area of research do you plan to cover?
- What is the basic premise of the case?
- What is the case/instance all about?
- What is the cause behind this?
- What are its immediate and long-term effects?
- How would you justify the results to the reader?
These are some of the questions the hypothesis and your paper aim to answer. Feel free to expand on this list and customize it as per your research. In this section, you try to look at the case from multiple perspectives. It gives you a more in-depth insight into the subject, making your essay holistic and credible.

Step 2: Empirical data collection
Empirical data collection is when you try to gather all your resources and studies. No research paper is ever written in isolation. Of course, you have to refer to other scholars and research studies done in the past
You must cite all these references in the nursing essay. I recommend students to follow the APA or Harvard in-text referencing as they’re ideal for stat-based papers. You can consult your peers or professors in case of any confusion.
This is also the section where you state the key takeaways from the hypothesis. Ensure that all the data you present is verified, authentic and error-free. It adds credibility to your research, building confidence in the reader to trust your analysis.
I also suggest students apply a few nursing theories and concepts relevant to your paper. Also, keep the hypothesis in the present tense.
Step 3: Conceptualization
This is the part where you arrange the different aspects of the hypothesis in an orderly way. Here you try to answer the four basic questions, applicable to every research project.
What: it refers to the fundamental question of- what is this paper all about. Here you talk about the critical points of the nursing case/idea and how it affects the industry
How: it refers to the technical aspects of the hypothesis. Here you talk about the research methodology and how you plan to prove or disprove the hypothesis
When: it sets your paper in a particular context. With the “when” question, you add relevance to your research. A hypothesis is built around limited information, the rest are but suppositions derived from these facts.
Why: it is the most critical aspect of the hypothesis that aims to delve into the reasons for writing this paper. This is where you outline the necessity of the research and how it adds value to the nursing community.
The research hypothesis usually deals with two or more variables
Step 4: Practical application
Practical application is crucial because it tests the effectiveness of your hypothesis. Without this step, your hypothesis loses any validity and remains but a mere assumption. There are two ways to test a theory – pure research and applied method.
The pure research method is where you collect all the information and review it academically. It is suitable for nursing students who want to analyze and interpret research studies in multiple ways. It also gives you more flexibility to delve into advance research if necessary.
The applied research method is set in the more practical ground. This is where you try to apply the data collected in the pure research section and apply it to realistic scenarios. Now, the practical application deals with both these aspects.
Here, the student learns how the theoretical aspects of nursing are used to improve everyday efficiency. The nursing student is usually interested in pure research, while the practitioner is concerned with the practical application.

Step 5: Conclusion and counterpoints
The last section of the hypothesis structure is where one presents counterpoints to refute your arguments. It is only fair that you give a complete view of the nursing subject. Think about all the possible critical alternatives that you can come up with.
In this section, I advise students to use a lot of infographics and stats to present a solid case. Your paper is but an extension of the hypothesis. It sets the ground for further research and opens new areas of exploration.
The conclusion is where you try to tie the loose ends together and reinstate your arguments. A hypothesis and its final analysis usually take a few paras. You can position it after the abstract section of the paper.
Types of hypothesis
There are seven different types of theory , each following a separate structure and format. However, for the sake of convenience, I will focus on the three major types that you can use in your nursing essay.
Keep the hypothesis in the present tense.
Research hypothesis
The research hypothesis is usually applied to scientific papers. Here, students must provide substantial data to back up their claims and perceptions. Also, the language of the research hypothesis is more academic and pronounced.
The research hypothesis usually deals with two or more variables, and the student must find ways to connect them using stats.
Null hypothesis
The null hypothesis is when the student must prove the absence of a connection between the two proposed variables. In this case, the two or more variables bear no logical relationship. And as a student, you must try to prove the same with stats and in-depth research.

Alternative hypothesis
An alternative hypothesis is when the research hypothesis fails to prove your line of argument. With the alternative explanation, you present the substitute. Ensure that you provide enough testing and results to prove it.
Quick links and references
I have curated a list of reading material and reference reading that you can check out. These sources were taken from the govt. Websites and university platforms. You can cite this for your paper for extra brownie points
Hypothesis structure
Hypothesis format guidelines
Nursing essay format
APA in-text referencing
Harvard reference guide
Citation generator- citethisforme
The Bottom Line
Hypothesis improves the arguments posed in any nursing essay. It sets the foundation for your research, giving you ample space to expand into the subject. With the hypothesis, you state the multiple variables and the connection between them.

Learn How To Write Better Assignments For Your University Course

Have a language expert improve your writing
Run a free plagiarism check in 10 minutes, generate accurate citations for free.
- Knowledge Base
- Null and Alternative Hypotheses | Definitions & Examples
Null & Alternative Hypotheses | Definitions, Templates & Examples
Published on May 6, 2022 by Shaun Turney . Revised on June 22, 2023.
The null and alternative hypotheses are two competing claims that researchers weigh evidence for and against using a statistical test :
- Null hypothesis ( H 0 ): There’s no effect in the population .
- Alternative hypothesis ( H a or H 1 ) : There’s an effect in the population.
Table of contents
Answering your research question with hypotheses, what is a null hypothesis, what is an alternative hypothesis, similarities and differences between null and alternative hypotheses, how to write null and alternative hypotheses, other interesting articles, frequently asked questions.
The null and alternative hypotheses offer competing answers to your research question . When the research question asks “Does the independent variable affect the dependent variable?”:
- The null hypothesis ( H 0 ) answers “No, there’s no effect in the population.”
- The alternative hypothesis ( H a ) answers “Yes, there is an effect in the population.”
The null and alternative are always claims about the population. That’s because the goal of hypothesis testing is to make inferences about a population based on a sample . Often, we infer whether there’s an effect in the population by looking at differences between groups or relationships between variables in the sample. It’s critical for your research to write strong hypotheses .
You can use a statistical test to decide whether the evidence favors the null or alternative hypothesis. Each type of statistical test comes with a specific way of phrasing the null and alternative hypothesis. However, the hypotheses can also be phrased in a general way that applies to any test.
Here's why students love Scribbr's proofreading services
Discover proofreading & editing
The null hypothesis is the claim that there’s no effect in the population.
If the sample provides enough evidence against the claim that there’s no effect in the population ( p ≤ α), then we can reject the null hypothesis . Otherwise, we fail to reject the null hypothesis.
Although “fail to reject” may sound awkward, it’s the only wording that statisticians accept . Be careful not to say you “prove” or “accept” the null hypothesis.
Null hypotheses often include phrases such as “no effect,” “no difference,” or “no relationship.” When written in mathematical terms, they always include an equality (usually =, but sometimes ≥ or ≤).
You can never know with complete certainty whether there is an effect in the population. Some percentage of the time, your inference about the population will be incorrect. When you incorrectly reject the null hypothesis, it’s called a type I error . When you incorrectly fail to reject it, it’s a type II error.
Examples of null hypotheses
The table below gives examples of research questions and null hypotheses. There’s always more than one way to answer a research question, but these null hypotheses can help you get started.
| ( ) | ||
| Does tooth flossing affect the number of cavities? | Tooth flossing has on the number of cavities. | test: The mean number of cavities per person does not differ between the flossing group (µ ) and the non-flossing group (µ ) in the population; µ = µ . |
| Does the amount of text highlighted in the textbook affect exam scores? | The amount of text highlighted in the textbook has on exam scores. | : There is no relationship between the amount of text highlighted and exam scores in the population; β = 0. |
| Does daily meditation decrease the incidence of depression? | Daily meditation the incidence of depression.* | test: The proportion of people with depression in the daily-meditation group ( ) is greater than or equal to the no-meditation group ( ) in the population; ≥ . |
*Note that some researchers prefer to always write the null hypothesis in terms of “no effect” and “=”. It would be fine to say that daily meditation has no effect on the incidence of depression and p 1 = p 2 .
The alternative hypothesis ( H a ) is the other answer to your research question . It claims that there’s an effect in the population.
Often, your alternative hypothesis is the same as your research hypothesis. In other words, it’s the claim that you expect or hope will be true.
The alternative hypothesis is the complement to the null hypothesis. Null and alternative hypotheses are exhaustive, meaning that together they cover every possible outcome. They are also mutually exclusive, meaning that only one can be true at a time.
Alternative hypotheses often include phrases such as “an effect,” “a difference,” or “a relationship.” When alternative hypotheses are written in mathematical terms, they always include an inequality (usually ≠, but sometimes < or >). As with null hypotheses, there are many acceptable ways to phrase an alternative hypothesis.
Examples of alternative hypotheses
The table below gives examples of research questions and alternative hypotheses to help you get started with formulating your own.
| Does tooth flossing affect the number of cavities? | Tooth flossing has an on the number of cavities. | test: The mean number of cavities per person differs between the flossing group (µ ) and the non-flossing group (µ ) in the population; µ ≠ µ . |
| Does the amount of text highlighted in a textbook affect exam scores? | The amount of text highlighted in the textbook has an on exam scores. | : There is a relationship between the amount of text highlighted and exam scores in the population; β ≠ 0. |
| Does daily meditation decrease the incidence of depression? | Daily meditation the incidence of depression. | test: The proportion of people with depression in the daily-meditation group ( ) is less than the no-meditation group ( ) in the population; < . |
Null and alternative hypotheses are similar in some ways:
- They’re both answers to the research question.
- They both make claims about the population.
- They’re both evaluated by statistical tests.
However, there are important differences between the two types of hypotheses, summarized in the following table.
| A claim that there is in the population. | A claim that there is in the population. | |
|
| ||
| Equality symbol (=, ≥, or ≤) | Inequality symbol (≠, <, or >) | |
| Rejected | Supported | |
| Failed to reject | Not supported |
To help you write your hypotheses, you can use the template sentences below. If you know which statistical test you’re going to use, you can use the test-specific template sentences. Otherwise, you can use the general template sentences.
General template sentences
The only thing you need to know to use these general template sentences are your dependent and independent variables. To write your research question, null hypothesis, and alternative hypothesis, fill in the following sentences with your variables:
Does independent variable affect dependent variable ?
- Null hypothesis ( H 0 ): Independent variable does not affect dependent variable.
- Alternative hypothesis ( H a ): Independent variable affects dependent variable.
Test-specific template sentences
Once you know the statistical test you’ll be using, you can write your hypotheses in a more precise and mathematical way specific to the test you chose. The table below provides template sentences for common statistical tests.
| ( ) | ||
| test
with two groups | The mean dependent variable does not differ between group 1 (µ ) and group 2 (µ ) in the population; µ = µ . | The mean dependent variable differs between group 1 (µ ) and group 2 (µ ) in the population; µ ≠ µ . |
| with three groups | The mean dependent variable does not differ between group 1 (µ ), group 2 (µ ), and group 3 (µ ) in the population; µ = µ = µ . | The mean dependent variable of group 1 (µ ), group 2 (µ ), and group 3 (µ ) are not all equal in the population. |
| There is no correlation between independent variable and dependent variable in the population; ρ = 0. | There is a correlation between independent variable and dependent variable in the population; ρ ≠ 0. | |
| There is no relationship between independent variable and dependent variable in the population; β = 0. | There is a relationship between independent variable and dependent variable in the population; β ≠ 0. | |
| Two-proportions test | The dependent variable expressed as a proportion does not differ between group 1 ( ) and group 2 ( ) in the population; = . | The dependent variable expressed as a proportion differs between group 1 ( ) and group 2 ( ) in the population; ≠ . |
Note: The template sentences above assume that you’re performing one-tailed tests . One-tailed tests are appropriate for most studies.
If you want to know more about statistics , methodology , or research bias , make sure to check out some of our other articles with explanations and examples.
- Normal distribution
- Descriptive statistics
- Measures of central tendency
- Correlation coefficient
Methodology
- Cluster sampling
- Stratified sampling
- Types of interviews
- Cohort study
- Thematic analysis
Research bias
- Implicit bias
- Cognitive bias
- Survivorship bias
- Availability heuristic
- Nonresponse bias
- Regression to the mean
Hypothesis testing is a formal procedure for investigating our ideas about the world using statistics. It is used by scientists to test specific predictions, called hypotheses , by calculating how likely it is that a pattern or relationship between variables could have arisen by chance.
Null and alternative hypotheses are used in statistical hypothesis testing . The null hypothesis of a test always predicts no effect or no relationship between variables, while the alternative hypothesis states your research prediction of an effect or relationship.
The null hypothesis is often abbreviated as H 0 . When the null hypothesis is written using mathematical symbols, it always includes an equality symbol (usually =, but sometimes ≥ or ≤).
The alternative hypothesis is often abbreviated as H a or H 1 . When the alternative hypothesis is written using mathematical symbols, it always includes an inequality symbol (usually ≠, but sometimes < or >).
A research hypothesis is your proposed answer to your research question. The research hypothesis usually includes an explanation (“ x affects y because …”).
A statistical hypothesis, on the other hand, is a mathematical statement about a population parameter. Statistical hypotheses always come in pairs: the null and alternative hypotheses . In a well-designed study , the statistical hypotheses correspond logically to the research hypothesis.
Cite this Scribbr article
If you want to cite this source, you can copy and paste the citation or click the “Cite this Scribbr article” button to automatically add the citation to our free Citation Generator.
Turney, S. (2023, June 22). Null & Alternative Hypotheses | Definitions, Templates & Examples. Scribbr. Retrieved June 24, 2024, from https://www.scribbr.com/statistics/null-and-alternative-hypotheses/
Is this article helpful?

Shaun Turney
Other students also liked, inferential statistics | an easy introduction & examples, hypothesis testing | a step-by-step guide with easy examples, type i & type ii errors | differences, examples, visualizations, what is your plagiarism score.
Simple Hypothesis
Ai generator.

Venturing into the realm of scientific inquiry, the hypothesis stands as a beacon, guiding researchers towards answers. A simple hypothesis, crisp and to the point, paves the way for clear testing and straightforward results. But how does one draft such a potent statement? And what makes it so effective? Join us as we demystify the art of creating simple hypothesis statements and share invaluable tips to refine your approach.”
What is an example of a Simple hypothesis statement?
A simple hypothesis statement typically specifies a relationship or difference between two variables. Here’s an example:
Caffeine Consumption and Alertness: Consuming caffeine increases a person’s alertness.
In this example, the two variables are “caffeine consumption” and “alertness.” The hypothesis simply posits that there’s a direct relationship between these two variables, indicating that as one (caffeine consumption) increases, the other (alertness) does as well.
100 Simple Hypothesis Statement Examples

Size: 166 KB
Simple hypothesis statements act as the backbone of research, succinctly proposing a direct relationship or difference between two variables. These straightforward declarations pave the way for clear testing and results, offering a digestible insight into expected outcomes.
- Sunlight and Plant Growth : Exposure to sunlight increases plant growth.
- Reading and Vocabulary Expansion : Regular reading leads to an expanded vocabulary.
- Exercise and Heart Health : Engaging in exercise improves heart health.
- Sugar Intake and Energy Levels : Consuming sugar temporarily boosts energy levels.
- Hydration and Skin Health : Drinking water improves skin hydration.
- Meditation and Stress Reduction : Practicing meditation reduces stress levels.
- Music and Productivity : Listening to music enhances work productivity.
- Sleep Duration and Cognitive Functions : Getting adequate sleep improves cognitive functions.
- Fertilizer and Crop Yield : Using fertilizers increases crop yields.
- Probiotics and Gut Health : Consuming probiotics enhances gut health.
- Screen Time and Eye Strain : Prolonged screen time leads to increased eye strain.
- Social Media Usage and Loneliness : Frequent social media use is linked to feelings of loneliness.
- Carbon Emissions and Global Warming : Higher carbon emissions contribute to global warming.
- Vitamin C and Immunity : Consuming vitamin C boosts immune functions.
- Artificial Lights and Sleep Quality : Exposure to artificial lights at night reduces sleep quality.
- Yoga and Flexibility : Regular yoga practice increases flexibility.
- Chocolate Consumption and Mood : Eating chocolate elevates mood.
- Brushing and Dental Health : Regular brushing reduces dental cavities.
- Temperature and Metabolism Rate : Cold environments accelerate metabolism.
- Pet Ownership and Happiness : Having a pet contributes to increased happiness levels.
- Puzzles and Brain Activity : Solving puzzles activates brain functions.
- Green Tea and Weight Loss : Drinking green tea aids in weight loss.
- Salt Intake and Blood Pressure : Consuming high amounts of salt raises blood pressure.
- Indoor Plants and Air Quality : Having indoor plants improves air quality.
- Antibiotics and Bacterial Infections : Taking antibiotics reduces bacterial infections.
- Laughter and Endorphin Release : Engaging in laughter releases endorphins.
- Gaming and Hand-Eye Coordination : Playing video games improves hand-eye coordination.
- Washing Hands and Germ Spread : Regular hand washing reduces the spread of germs.
- Spicy Foods and Metabolism : Consuming spicy foods boosts metabolism.
- Journaling and Emotional Health : Maintaining a journal aids emotional well-being.
- Urban Areas and Noise Pollution : Urban regions are associated with higher noise pollution.
- Physical Activity and Bone Density : Regular physical activity strengthens bone density.
- Aloe Vera and Skin Soothing : Applying aloe vera soothes skin irritations.
- Alcohol Consumption and Reaction Time : Drinking alcohol slows down reaction time.
- Bird Watching and Patience : Engaging in bird watching cultivates patience.
- Cycling and Leg Strength : Regular cycling enhances leg muscle strength.
- Public Speaking and Confidence : Practicing public speaking boosts confidence.
- Dancing and Cardiovascular Health : Dancing regularly improves cardiovascular health.
- Acupuncture and Pain Relief : Undergoing acupuncture reduces pain.
- Caloric Restriction and Lifespan : Reducing caloric intake is linked to extended lifespan.
- Olive Oil and Heart Health : Consuming olive oil promotes heart health.
- Mindfulness and Attention Span : Practicing mindfulness increases attention span.
- Bilingualism and Cognitive Flexibility : Being bilingual enhances cognitive flexibility.
- Heavy Metals and Water Toxicity : Presence of heavy metals increases water toxicity.
- Mountain Climbing and Stamina : Engaging in mountain climbing builds stamina.
- Urbanization and Wildlife Displacement : Increased urbanization leads to wildlife displacement.
- Mentoring and Career Progression : Having a mentor accelerates career progression.
- Organic Farming and Soil Health : Practicing organic farming enhances soil health.
- Red Wine and Antioxidant Intake : Consuming red wine increases antioxidant intake.
- Studying Abroad and Cultural Awareness : Studying abroad enhances cultural awareness.
- E-books and Reading Duration : Using e-books extends reading duration.
- Swimming and Lung Capacity : Regular swimming increases lung capacity.
- Deforestation and Carbon Dioxide Levels : Deforestation raises carbon dioxide levels.
- Fast Food and Obesity : Frequent fast food consumption is linked to obesity.
- Classical Music and Infant Sleep : Playing classical music improves infant sleep duration.
- Microplastics and Marine Pollution : The presence of microplastics heightens marine pollution.
- Afforestation and Rainfall : Increasing forest cover can lead to higher rainfall.
- Gratitude Journaling and Positivity : Maintaining a gratitude journal boosts feelings of positivity.
- Singing and Lung Function : Regular singing enhances lung function.
- Noise Pollution and Stress : Exposure to noise pollution increases stress levels.
- Rural Living and Mental Peace : Living in rural areas promotes mental peace.
- Soft Drinks and Bone Density : Consuming soft drinks decreases bone density.
- Travel and Open-mindedness : Traveling frequently fosters open-mindedness.
- Digital Learning and Student Engagement : Digital learning tools increase student engagement.
- Plastic Usage and Land Pollution : Increased plastic usage contributes to land pollution.
- Stretching and Muscle Flexibility : Daily stretching improves muscle flexibility.
- Wine Consumption and Gut Health : Moderate wine consumption benefits gut health.
- Homework and Academic Achievement : Regular homework boosts academic achievement.
- Raw Foods and Digestive Health : Consuming raw foods aids digestive health.
- High Heels and Posture : Wearing high heels affects posture negatively.
- Therapy and Mental Well-being : Engaging in therapy promotes mental well-being.
- Fast Charging and Battery Lifespan : Using fast charging can reduce battery lifespan.
- Pottery and Hand Dexterity : Practicing pottery improves hand dexterity.
- Group Study and Retention : Studying in groups enhances information retention.
- Red Meat and Cholesterol Levels : Consuming red meat increases cholesterol levels.
- Kombucha and Gut Flora : Drinking kombucha benefits gut flora.
- Night Driving and Accident Risk : Driving at night increases the risk of accidents.
- Karaoke and Social Bonding : Engaging in karaoke fosters social bonding.
- Balanced Diet and Energy Levels : Following a balanced diet boosts energy levels.
- Multitasking and Task Efficiency : Multitasking reduces task efficiency.
- Gardening and Stress Relief : Regular gardening acts as a stress reliever.
- Digital Detox and Sleep Quality : Undertaking a digital detox improves sleep quality.
- Massage and Muscle Relaxation : Getting massages aids muscle relaxation.
- Animal Therapy and Emotional Healing : Engaging with animals accelerates emotional healing.
- Crafting and Creativity : Regular crafting activities enhance creativity.
- Organ Donation and Life-saving : Organ donation can be life-saving.
- Bamboo Products and Sustainability : Using bamboo products promotes sustainability.
- Weight Training and Muscle Mass : Engaging in weight training increases muscle mass.
- Fermented Foods and Digestion : Consuming fermented foods aids digestion.
- Outdoor Activities and Vitamin D Levels : Engaging in outdoor activities boosts Vitamin D levels.
- Smoking and Lung Health : Regular smoking deteriorates lung health.
- Feedback and Performance Improvement : Receiving feedback improves performance.
- Adventure Sports and Risk-taking Ability : Engaging in adventure sports enhances risk-taking ability.
- Coding and Logical Thinking : Learning to code promotes logical thinking.
- Chocolate and Antioxidant Levels : Eating dark chocolate boosts antioxidant levels.
- Vegetarian Diet and Heart Health : Following a vegetarian diet improves heart health.
- Deep Breathing and Relaxation : Practicing deep breathing induces relaxation.
- Natural Light and Productivity : Exposure to natural light enhances productivity.
- Green Spaces and Mental Health : Access to green spaces boosts mental well-being.
- Recycling and Resource Conservation : Regular recycling promotes resource conservation.
Simple Hypothesis Statement Examples for Kids
Kids often view the world with endless curiosity. Simplified hypotheses allow them to test their surroundings and grasp scientific methods. These Hypothesis for kids statements, tailored for young inquisitors, provide clear cause-and-effect scenarios to foster their learning.
- Ice Melting : Placing ice in the sun will make it melt faster than in the shade.
- Plant Growth : Plants kept near the window grow taller than plants in dark corners.
- Pet’s Activity : Dogs are more active during the day than at night.
- Toy Durability : Soft toys tear more easily than hard plastic toys.
- Sleep Patterns : Going to bed late makes you feel more tired the next morning.
- Food Preference : Cats prefer fish-flavored food over chicken-flavored food.
- Shadow Formation : Standing against the light creates longer shadows during the evening.
- Bubble Size : Using more soap in water creates bigger bubbles.
- Learning Speed : Kids remember rhymes faster with music than without.
- Color Attraction : Brightly colored toys attract more attention than dull-colored ones.
Simple Hypothesis Statement Examples for Research Paper
In academic settings, crafting a straightforward hypothesis helps anchor a research paper, allowing readers to quickly understand the focal point. Here are concise research hypothesis statements ideal for academic exploration.
- Diet and Cholesterol : A Mediterranean diet lowers cholesterol levels more effectively than a Western diet.
- Urban Development : Rapid urbanization leads to increased air pollution.
- Language Acquisition : Immersion learning accelerates second language acquisition compared to classroom learning.
- Climate Change : Increasing global temperatures directly correlate with rising sea levels.
- Digital Learning : Online education reduces classroom engagement levels.
- Consumer Behavior : Discount offers increase sales during festive seasons.
- Migration Patterns : Economic downturns in a region trigger increased migration.
- Environmental Conservation : Protected wildlife zones reduce species extinction rates.
- Cultural Influence : Exposure to global media diminishes local cultural practices.
- Public Health : Regular public health campaigns reduce the spread of infectious diseases.
Simple Hypothesis Statement Examples for Nursing
In nursing, hypotheses aim to shed light on patient care, health outcomes, and the intricacies of the medical field. These focused statements offer directions for nursing research and practice.
- Post-Operative Recovery : Patients with post-operative physiotherapy recover faster than those without.
- Pain Management : Music therapy reduces the need for pain medication in chronic pain patients.
- Infant Care : Skin-to-skin contact immediately after birth strengthens mother-infant bonding.
- Elderly Health : Regular social interactions decrease the onset of dementia in the elderly.
- Disease Awareness : Regular health check-ups reduce late-stage disease diagnoses.
- Mental Health : Group therapy sessions enhance coping mechanisms for depression patients.
- Patient Satisfaction : Nurse-patient ratios are directly proportional to patient satisfaction rates.
- Medication Adherence : Simplified medication regimens increase adherence in elderly patients.
- Diet and Recovery : High protein diets speed up wound healing in hospitalized patients.
- Sleep and Health : Night-shift workers report higher levels of fatigue than day-shift workers.
Simple Hypothesis Statement Examples in Psychology
Psychology delves deep into the human psyche. Simple pyschology hypothesis in this domain assist in understanding behavioral patterns, cognitive functions, and emotional dynamics. Here are statements reflective of common psychological queries.
- Child Behavior : Children exposed to violent media exhibit more aggressive behaviors.
- Memory and Age : Memory recall decreases with advancing age.
- Group Dynamics : Individuals in larger groups are less likely to exhibit helping behaviors.
- Stress and Performance : Moderate levels of stress enhance performance on cognitive tasks.
- Mood and Perception : Positive moods increase the likelihood of optimistic future expectations.
- Learning Styles : Visual learners retain graphic information better than auditory information.
- Emotions and Decision Making : Intense emotions impair rational decision-making processes.
- Peer Pressure : Adolescents are more likely to engage in risk-taking behaviors under peer influence.
- Personality and Career Choices : Introverts are more drawn to independent job roles than extroverts.
- Dream Patterns : Exposure to traumatic events increases the frequency of nightmares.
Simple Hypothesis Statement Examples for Research
Effective research begins with a precise hypothesis. These straightforward declarations guide the investigative journey, providing clarity in discerning outcomes and assessing implications.
- Technology and Employment : Automation in industries leads to a reduction in manual jobs.
- Marketing Techniques : Influencer marketing garners more engagement than traditional advertising.
- Environmental Initiatives : Implementing green technologies reduces corporate carbon footprints.
- Dietary Habits : Vegan diets result in lower carbon footprints than omnivorous diets.
- Economic Policies : Tax breaks for the middle class stimulate economic growth.
- Educational Systems : Student-led learning methods increase long-term knowledge retention.
- Public Policies : Urban green spaces correlate with reduced crime rates.
- Cultural Shifts : Increased global travel promotes intercultural understanding and tolerance.
- Health Trends : Veganism leads to reduced risks of heart-related diseases.
- Digital Consumption : Increased screen time is linked to declining mental well-being.
Simple vs Complex Hypothesis example
When it comes to scientific research, hypotheses play a pivotal role in guiding investigations. At the core, a hypothesis is a statement about a potential relationship between variables, or an explanation of an occurrence, which is testable. Based on their structural and conceptual nature, hypotheses can be categorized into simple and complex.
A simple hypothesis is a statement that explains the relationship between two variables – one independent variable and one dependent variable. Because it explains the expected relationship in the simplest form, it’s straightforward to test.
Example: Drinking caffeine improves short-term memory.
In this example:
- Independent Variable : Caffeine consumption
- Dependent Variable : Short-term memory
Complex Hypothesis
A complex good hypothesis , in contrast, deals with the relationship between two or more independent variables and two or more dependent variables. This means it’s multidimensional and requires more intricate testing procedures.
Example: Consuming caffeine and sugar together improves short-term memory and reaction time better than consuming either alone.
- Independent Variables : Caffeine consumption and sugar consumption
- Dependent Variables : Short-term memory and reaction time
How do you write a Simple hypothesis statement? – A Step by Step Guide
Step 1: identify your research question.
Every hypothesis stems from a research question. For instance, “Does sunlight affect plant growth?” From this, you can create your hypothesis.
Step 2: Determine the Variables
Every hypothesis has two essential variables:
- Independent Variable : The cause or reason. (Sunlight in our example)
- Dependent Variable : The effect or outcome. (Plant growth in our example)
Step 3: Formulate the Relationship
Specify the expected relationship between the independent and dependent variable. It might be a positive correlation, negative correlation, or no correlation.
Step 4: Keep It Testable
Ensure your hypothesis can be tested empirically. It should be specific enough that experiments or observations can prove or disprove it.
Step 5: Write the Statement
Now, construct your statement. For our example, a potential hypothesis might be: Exposing plants to more sunlight will result in faster growth.
Tips for Writing Simple Hypothesis
- Stay Focused : Stick to one specific relationship between an independent and dependent variable. Avoid including multiple causes or effects to keep it simple.
- Be Clear & Concise : Use clear, straightforward language. Avoid jargon unless it’s necessary for specificity.
- Ensure It’s Testable : A hypothesis is only useful if you can test it. Avoid abstract or overly broad statements.
- Base on Existing Research : While your hypothesis will guide new research, it should be grounded in existing theories or observations.
- Avoid Bias : Ensure your hypothesis doesn’t show any personal beliefs or inclinations. It should be neutral.
- Revisit & Refine : After writing, revisit your hypothesis. Does it still align with your research question? Is there a clearer way to phrase it?
- Stay Open to Changes : Based on the results of your tests or experiments, be prepared to change or adjust your hypothesis.
Remember, a hypothesis is an educated guess. It’s not a definitive explanation, but rather a proposed one, and its primary purpose is to guide your research. Whether your hypothesis gets supported or refuted, the insights you gain are invaluable.
Text prompt
- Instructive
- Professional
10 Examples of Public speaking
20 Examples of Gas lighting
Home » Northern Arizona University » How Do You Write A Nursing Hypothesis?
How Do You Write A Nursing Hypothesis?
Table of Contents
How do you write a hypothesis example?
Usually, you’ll want to form your hypothesis as a statement, not a question. For example: If I raise the temperature of a cup of water, then the amount of sugar that can be dissolved in it will be increased.
What is a hypothesis in nursing research?
A hypothesis is a statement of the researcher’s expectation or prediction about relationship among study variables . The research process begins and ends with the hypothesis. It is core to the entire procedure and, therefore, is of the utmost importance.
What is hypothesis example?
Examples of Hypotheses “ Students who eat breakfast will perform better on a math exam than students who do not eat breakfast .” “Students who experience test anxiety prior to an English exam will get higher scores than students who do not experience test anxiety.”
How do you formulate a hypotheses?
How to Formulate an Effective Research Hypothesis
- State the problem that you are trying to solve. Make sure that the hypothesis clearly defines the topic and the focus of the experiment.
- Try to write the hypothesis as an if-then statement.
- Define the variables.
What are the 3 required parts of a hypothesis?
A hypothesis is a prediction you create prior to running an experiment. The common format is: If [CAUSE], then [EFFECT], because [RATIONALE]. In the world of experience optimization, strong hypotheses consist of three distinct parts: a definition of the problem, a proposed solution, and a result .
Which statement is the best example of a hypothesis?
The best example of a hypothesis is If a plant receives water, then it will grow faster . Explanation: In the scientific method of research, a hypothesis can be described as a tentative statement that can be proved right or wrong. A hypothesis can be tested through experiments and the results can be deduced from it.
What is an example of hypothesis testing in nursing?
For example, suppose a doctor believes that a new drug is able to reduce blood pressure in obese patients. To test this, he may measure the blood pressure of 40 patients before and after using the new drug for one month.
What is a hypothesis in healthcare?
[hi-poth´ĕ-sis] a supposition that appears to explain a group of phenomena and is advanced as a bases for further investigation . alternative hypothesis the hypothesis that is formulated as an opposite to the null hypothesis in a statistical test.
What is a simple hypothesis?
Simple hypotheses are ones which give probabilities to potential observations . The contrast here is with complex hypotheses, also known as models, which are sets of simple hypotheses such that knowing that some member of the set is true (but not which) is insufficient to specify probabilities of data points.
What are 5 characteristics of a good hypothesis?
A good hypothesis possesses the following certain attributes.
- Power of Prediction. One of the valuable attribute of a good hypothesis is to predict for future.
- Closest to observable things.
- Simplicity.
- Testability.
- Relevant to Problem.
- Relevant to available Techniques.
What is an example of a hypothesis question?
For example, let’s say you have a bad breakout the morning after eating a lot of greasy food. You may wonder if there is a correlation between eating greasy food and getting pimples. You propose the hypothesis: Eating greasy food causes pimples.
What makes a good hypothesis?
Criteria for good hypotheses be as brief and clear as possible; state an expected relationship or difference between two or more variables; be testable; and. be grounded in past knowledge, gained from the literature review or from theory.
How do you state a hypothesis introduction?
The first few paragraphs of a journal article serve to introduce the topic, to provide the author’s hypothesis or thesis, and to indicate why the research was done . A thesis or hypothesis is not always clearly labled; you may need to read through the introductory paragraphs to determine what the authors are proposing.
Is a hypothesis always a question?
What is a hypothesis? A hypothesis is a statement that can be proved or disproved. A research question can be made into a hypothesis by changing it into a statement .
Do hypothesis have to be if then?
The hypothesis is often written using the words “IF” and “THEN.” For example, “If I do not study, then I will fail the test.” The “if’ and “then” statements reflect your independent and dependent variables. The hypothesis should relate back to your original question and must be testable.
Which of the following is the best example of a strong hypothesis?
Answer and Explanation: Answer: c. Plants that get less light will grow less . A strong hypothesis defines the variable that can be measured and the relationship between…
How do you write a hypothesis for a research proposal?
- Variables in hypotheses. Hypotheses propose a relationship between two or more variables.
- Ask a question. Writing a hypothesis begins with a research question that you want to answer.
- Do some preliminary research.
- Formulate your hypothesis.
- Refine your hypothesis.
- Phrase your hypothesis in three ways.
- Write a null hypothesis.
Which of the following is the best example of a scientific question?
A good scientific question is: “ What effect does the pH of water have on radish seed germination? ” Good scientific questions are defined, measurable, and controllable.
What are the 7 steps in hypothesis testing?
1.2 – The 7 Step Process of Statistical Hypothesis Testing
- Step 1: State the Null Hypothesis.
- Step 2: State the Alternative Hypothesis.
- Step 3: Set.
- Step 4: Collect Data.
- Step 5: Calculate a test statistic.
- Step 6: Construct Acceptance / Rejection regions.
- Step 7: Based on steps 5 and 6, draw a conclusion about.
Why is hypothesis important in nursing?
Implications for practice: Hypothesis testing strengthens the quality of the quantitative studies, increases the generality of findings and provides dependable knowledge . This is particularly true for quantitative studies that aim to explore, explain and predict/control phenomena and/or test theories.

By Cary Hardy
Hi there! I'm Cary Hardy, an education expert and consultant. I've worked with students of all ages and backgrounds, and I love helping them unlock their full potential. I'm also a big believer in lifelong learning- there's always something new to learn!
I got my start in education as a teacher, working with students in grades K-12. After several years of teaching, I transitioned into the world of educational consulting. I've since worked with schools and districts all over the country, helping them improve their curriculums and instruction methods.
I'm passionate about helping people achieve their dreams, and I believe that education is the key to unlocking everyone's potential. Thanks for reading!
You might also like:
Does nau have frat houses, what is considered northern arizona, what is in northwestern arizona.
Nurse-to-Patient Ratio: Hypothesis Test Study
A hypothesis test study allows determining if a hypothesis is true based on research findings. For example, concluding whether an increased nurse-to-patient ratio results in improved patient health outcomes would help make decisions about the desired staffing levels (Giuliano, Danesh, & Funk, 2016). The present paper will describe a study to test the proposed hypothesis.
Prior to beginning the study, it is essential to identify the research and null hypotheses. The research hypothesis is that an increased nurse-to-patient ratio results in a decreased rate of readmissions. The null hypothesis is that there is no correlation between the nurse-to-patient ratio and readmissions rate. The independent variable in the proposed study is the nurse-to-patient ratio, whereas the dependent variable is the rate of readmissions at 30 days after discharge.
To test the hypothesis, it would be necessary to study readmission rates at two separate acute care hospitals with different nurse staffing levels. The data should be recorded for at least three months to make viable conclusions. It is expected that the difference in 30-day readmission rates would be comparable to those in nurse-to-patient ratios. For instance, if Hospital 1 has a 20% higher nurse-to-patient ratio than Hospital 2, it can be guessed that the readmissions rate in Hospital 1 will be 15-20% lower than in Hospital 2.
The outcomes of this hypothesis test study could help in administrative decision-making and patient advocacy. If the null hypothesis were rejected, it would mean that a higher nurse-to-patient ratio contributes to patient health and improves patient safety. Nurses would be able to use these results to show hospital leaders that it is critical to increasing the number of nurses employed to enhance patient outcomes.
Giuliano, K. K., Danesh, V., & Funk, M. (2016). The relationship between nurse staffing and 30-day readmission for adults with heart failure. The Journal of Nursing Administration, 46(1), 25-29.
Cite this paper
- Chicago (N-B)
- Chicago (A-D)
StudyCorgi. (2021, July 9). Nurse-to-Patient Ratio: Hypothesis Test Study. https://studycorgi.com/nurse-to-patient-ratio-hypothesis-test-study/
"Nurse-to-Patient Ratio: Hypothesis Test Study." StudyCorgi , 9 July 2021, studycorgi.com/nurse-to-patient-ratio-hypothesis-test-study/.
StudyCorgi . (2021) 'Nurse-to-Patient Ratio: Hypothesis Test Study'. 9 July.
1. StudyCorgi . "Nurse-to-Patient Ratio: Hypothesis Test Study." July 9, 2021. https://studycorgi.com/nurse-to-patient-ratio-hypothesis-test-study/.
Bibliography
StudyCorgi . "Nurse-to-Patient Ratio: Hypothesis Test Study." July 9, 2021. https://studycorgi.com/nurse-to-patient-ratio-hypothesis-test-study/.
StudyCorgi . 2021. "Nurse-to-Patient Ratio: Hypothesis Test Study." July 9, 2021. https://studycorgi.com/nurse-to-patient-ratio-hypothesis-test-study/.
This paper, “Nurse-to-Patient Ratio: Hypothesis Test Study”, was written and voluntary submitted to our free essay database by a straight-A student. Please ensure you properly reference the paper if you're using it to write your assignment.
Before publication, the StudyCorgi editorial team proofread and checked the paper to make sure it meets the highest standards in terms of grammar, punctuation, style, fact accuracy, copyright issues, and inclusive language. Last updated: November 11, 2023 .
If you are the author of this paper and no longer wish to have it published on StudyCorgi, request the removal . Please use the “ Donate your paper ” form to submit an essay.
COMMENTS
So, Nurse Jory's research purpose is "The purpose of this research study is to explore barriers to appointment attendance.". After the research problem and purpose statement comes the research hypothesis, by identifying the research variables. Research variables are the concepts that are measured, manipulated, or controlled in a study.
Open Resources for Nursing (Open RN) ... They can see how certain objects or events form a pattern (i.e., generalization) that indicates a common problem (i.e., hypothesis). Example: A nurse assesses a patient and finds the surgical incision site is red, warm, and tender to the touch. The nurse recognizes these cues form a pattern of signs of ...
An example of a hypothesis is below. Research Hypothesis: Drug 23 will significantly reduce symptoms associated with Disease A compared to Drug 22. ... Nursing, Allied Health, and Interprofessional Team Interventions. All physicians, nurses, pharmacists, and other healthcare professionals should strive to understand the concepts in this chapter ...
Are you a nursing student and need to write a #nursing #hypothesis for your assignment?Here are 3 main steps to follow. In brief, a nursing diagnosis is a cl...
Associative hypothesis Categorical variable Causal hypothesis Complex hypothesis Confounding variable Continuous variable. Chapter Objectives. At the conclusion of this chapter, the learner will be able to. 1. Discuss processes involved in identifying a researchable problem in . nursing practice. 2. Write an effective problem statement. 3.
Developing a hypothesis (with example) Step 1. Ask a question. Writing a hypothesis begins with a research question that you want to answer. The question should be focused, specific, and researchable within the constraints of your project. Example: Research question.
Directional hypothesis: Specifies not only the existence but also the expected direction of the relationship between the dependent (outcome) and the independent (intervention) variables. You will also see this called "One-tailed hypothesis". Example: Depression scores will decrease following a 6-week intervention.
©Kaiser Permanente Northern and Southern California Nursing Research Research Aims, Purpose, and Hypotheses 19 [email protected] ©2010 Kaiser Permanente Southern & Northern California Nursing Research Hypothesis •A hypothesis is a formal statement of the expected relationship between two or more variables in a specified population.
The P value is the probability that the results of a study are caused by chance alone. To better understand this definition, consider the role of chance. The concept of chance is illustrated with every flip of a coin. The true probability of obtaining heads in any single flip is 0.5, meaning that heads would come up in half of the flips and ...
example, that cigarette smoking (IV) can lead to both lung cancer (DV 1) and coronary disorders (DV 2). Complex hypotheses are common in studies that try to assess the effect of a nursing intervention on multiple outcomes. Example of a Complex Hypothesis—Multiple Dependent Variables: Grey and colleagues
Nursing theories help bedside nurses evaluate patient care and base nursing interventions on the evaluation of the findings. The theories can also provide nurses with the rationale to make certain decisions. An example of a nursing theory in use is seen in the care of a Jehovah's Witnesses patient that does not believe in blood transfusions.
Grand Nursing Theories. Grand theories are abstract, broad in scope, and complex, therefore requiring further research for clarification. Grand nursing theories do not guide specific nursing interventions but rather provide a general framework and nursing ideas.; Grand nursing theorists develop their works based on their own experiences and their time, explaining why there is so much variation ...
A hypothesis is a tentative statement about the relationship between two or more variables. It is a specific, testable prediction about what you expect to happen in a study. It is a preliminary answer to your question that helps guide the research process. Consider a study designed to examine the relationship between sleep deprivation and test ...
3. Simple hypothesis. A simple hypothesis is a statement made to reflect the relation between exactly two variables. One independent and one dependent. Consider the example, "Smoking is a prominent cause of lung cancer." The dependent variable, lung cancer, is dependent on the independent variable, smoking. 4.
A hypothesis is a proposed explanation for a situation. It attempts to explain the "why" behind the problem that is occurring. If a "why" is identified, then a solution can begin to be explored. ... Another example of independent nursing interventions is the therapeutic communication that a nurse uses to assist patients to cope with a ...
Download to read offline. 1. Formulating hypothesis Maria Carmela L. Domocmat, MSN, RN Assistant Professor, Northern Luzon Adventist College. 2. Hypothesis is your prediction of the relationship you expect to find. A tentative prediction about the relationship between two or more variables. 10/2/2014 Maria Carmela L. Domocmat, RN, MSN. 3.
Oct 16, 2023, 15:55 PM. <4-minute read> Teaching nursing students to prioritize hypotheses is an essential step for nurse educators as they develop clinical judgment skills in new nurses. Learn how interactive resources can help. Developing strong clinical judgment skills in nursing students is a primary focus for all nurse educators because it ...
Structuring your hypothesis. The hypothesis forms the crux of any nursing essay or scientific research, for that matter. It comes at the very beginning of your paper, even before the introduction para. It sets your research in a specific context, giving you the space to outline the intent and purpose of the article.
The alternative hypothesis (H a) is the other answer to your research question. It claims that there's an effect in the population. Often, your alternative hypothesis is the same as your research hypothesis. In other words, it's the claim that you expect or hope will be true. The alternative hypothesis is the complement to the null hypothesis.
Based on urgency and risk, which hypothesis would the nurse rank as the priority? Risk for Activity Intolerance; supporting data: increased fatigue, difficulty breathing, dyspnea Self-Care Deficit; supporting data: inability to ambulate autonomously, inability to bathe independently Hypervolemia; supporting data: coarse crackles, dyspnea, 2+ edema, hypertension, heart failure diagnosis Urinary ...
Simple Hypothesis Statement Examples for Nursing. In nursing, hypotheses aim to shed light on patient care, health outcomes, and the intricacies of the medical field. These focused statements offer directions for nursing research and practice. Post-Operative Recovery: Patients with post-operative physiotherapy recover faster than those without.
The hypothesis is often written using the words "IF" and "THEN.". For example, "If I do not study, then I will fail the test.". The "if' and "then" statements reflect your independent and dependent variables. The hypothesis should relate back to your original question and must be testable. Recent post: What Are Examples Of ...
Words: 279 Pages: 1. A hypothesis test study allows determining if a hypothesis is true based on research findings. For example, concluding whether an increased nurse-to-patient ratio results in improved patient health outcomes would help make decisions about the desired staffing levels (Giuliano, Danesh, & Funk, 2016).