
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- HHS Author Manuscripts

Neurobiology of gender identity and sexual orientation
Sexual identity and sexual orientation are independent components of a person’s sexual identity. These dimensions are most often in harmony with each other and with an individual’s genital sex, although not always. The present review discusses the relationship of sexual identity and sexual orientation to prenatal factors that act to shape the development of the brain and the expression of sexual behaviours in animals and humans. One major influence discussed relates to organisational effects that the early hormone environment exerts on both gender identity and sexual orientation. Evidence that gender identity and sexual orientation are masculinised by prenatal exposure to testosterone and feminised in it absence is drawn from basic research in animals, correlations of biometric indices of androgen exposure and studies of clinical conditions associated with disorders in sexual development. There are, however, important exceptions to this theory that have yet to be resolved. Family and twin studies indicate that genes play a role, although no specific candidate genes have been identified. Evidence that relates to the number of older brothers implicates maternal immune responses as a contributing factor for male sexual orientation. It remains speculative how these influences might relate to each other and interact with postnatal socialisation. Nonetheless, despite the many challenges to research in this area, existing empirical evidence makes it clear that there is a significant biological contribution to the development of an individual’s sexual identity and sexual orientation.
1 |. INTRODUCTION
Gender identity and sexual orientation are fundamental independent characteristics of an individual’s sexual identity. 1 Gender identity refers to a person’s innermost concept of self as male, female or something else and can be the same or different from one’s physical sex. 2 Sexual orientation refers to an enduring pattern of emotional, romantic and/or sexual attractions to men, women or both sexes. 3 Both gender identity and sexual orientation are characterised by obvious sex differences. Most genetic females identify as such and are attracted to males (ie, androphilic) and most genetic males identify as males and are attracted to females (ie, gynophilic). The existence of these dramatic sex differences suggest that gonadal hormones, particularly testosterone, might be involved, given that testosterone plays an important role in the development of most, behavioural sex differences in other species. Here, a review is provided of the evidence that testosterone influences human gender identity and sexual orientation. The review begins by summarising the available information on sex hormones and brain development in other species that forms the underpinnings of the hypothesis suggesting that these human behaviours are programmed by the prenatal hormone environment, and it will also consider contributions from genes. This is followed by a critical evaluation of the evidence in humans and relevant animal models that relates sexual identity and sexual orientation to the influences that genes and hormones have over brain development.
2 |. HORMONES, GENES AND SEXUAL DIFFERENTIATION OF THE BRAIN AND BEHAVIOUR
The empirical basis for hypothesising that gonadal hormones influence gender identity and sexual orientation is based on animal experiments involving manipulations of hormones during prenatal and early neonatal development. It is accepted dogma that testes develop from the embryonic gonad under the influence of a cascade of genes that begins with the expression of the sex-determining gene SRY on the Y chromosome. 4 , 5 Before this time, the embryonic gonad is “indifferent”, meaning that it has the potential to develop into either a testis or an ovary. Likewise, the early embryo has 2 systems of ducts associated with urogenital differentiation, Wolffian and Müllerian ducts, which are capable of developing into the male and female tubular reproductive tracts, respectively. Once the testes develop, they begin producing 2 hormones, testosterone and anti-Müllerian hormone (AMH). In rats, this occurs around day 16–17 of gestation, whereas, in humans, it occurs at about 7–8 weeks of gestation. 6 Testosterone and one of its derivatives, dihydrotestosterone, induce the differentiation of other organs in the male reproductive system, whereas AMH causes the degeneration of the Müllerian ducts. Female ovaries develop under the influence of a competing set of genes that are influenced by expression of DAX1 on the X chromosome and act antagonistically to SRY. The female reproductive tract in the embryo develops in the absence of androgens and later matures under the influence hormones produced by the ovary, in particular oestradiol.
Analogous processes occur during early development for sexual differentiation of the mammalian brain and behaviour. According to the classical or organisational theory, 7 , 8 prenatal and neonatal exposure to testosterone causes male-typical development (masculinisation), whereas female-typical development (feminisation) occurs in the relative absence of testosterone. Masculinisation involves permanent neural changes induced by steroid hormones and differs from the more transient activational effects observed after puberty. These effects typically occur during a brief critical period in development when the brain is most sensitive to testosterone or its metabolite oestradiol. In rats, the formation of oestradiol in the brain by aromatisation of circulating testosterone is the most important mechanism for the masculinisation of the brain; 9 however, as shown below, testosterone probably acts directly without conversion to oestradiol to influence human gender identity and sexual orientation. The times when testosterone triggers brain sexual differentiation in different species correspond to periods when testosterone is most elevated in males compared to females. In rodents and other altricial species, this occurs largely during the first 5 days after birth, whereas, in humans, the elevation in testosterone occurs between months 2 and 6 of pregnancy and then again from 1 to 3 months postnatally. 6 During these times, testosterone levels in the circulation are much higher in males than in females. These foetal and neonatal peaks of testosterone, together with functional steroid receptor activity, are considered to program the male brain both phenotypically and neurologically. In animal models, programming or organising actions are linked to direct effects on the various aspects of neural development that influence cell survival, neuronal connectivity and neurochemical specification. 10 Many of these effects occur well after the initial hormone exposure and have recently been linked to epigenetic mechanisms. 11
The regional brain differences that result from the interaction between hormones and developing brain cells are assumed to be the major basis of sex differences in a wide spectrum of adult behaviours, such as sexual behaviour, aggression and cognition, as well as gender identity and sexual orientation. Factors that interfere with the interactions between hormones and the developing brain systems during gestation may permanently influence later behaviour. Studies in sheep and primates have clearly demonstrated that sexual differentiation of the genitals takes places earlier in development and is separate from sexual differentiation of the brain and behaviour. 12 , 13 In humans, the genitals differentiate in the first trimester of pregnancy, whereas brain differentiation is considered to start in the second trimester. Usually, the processes are coordinated and the sex of the genitals and brain correspond. However, it is hypothetically possible that, in rare cases, these events could be influenced independently of each other and result in people who identify with a gender different from their physical sex. A similar reasoning has been invoked to explain the role of prenatal hormones on sexual orientation.
Although the role of gonadal steroids in the sexual differentiation of reproductive brain function and behaviour is undeniable, males and females also carry a different complement of genes encoded on their sex chromosomes that also influence sexual differentiation of the brain. 14 – 16 As will be discussed, family and twin studies suggest that there is a genetic component to gender identity and sexual orientation at least in some individuals. However, the nature of any genetic predisposition is unknown. The genetic component could be coding directly for these traits or, alternatively, could influence hormonal mechanisms by determining levels of hormones, receptors or enzymes. Genetic factors and hormones could also make separate yet complementary or antagonistic contributions. It should be noted that, although the early hormone environment appears to influence gender identity and sexual orientation, hormone levels in adulthood do not. There are no reports indicating that androgen levels differ as a function of gender identity or sexual orientation or that treatment with exogenous hormones alters these traits in either sex.
3 |. GENDER IDENTITY
The establishment of gender identity is a complex phenomenon and the diversity of gender expression argues against a simple or unitary explanation. For this reason, the extent to which it is determined by social vs biological (ie, genes and hormones) factors continues to be debated vigorously. 17 The biological basis of gender identity cannot be modelled in animals and is best studied in people who identify with a gender that is different from the sex of their genitals, in particular transsexual people. Several extensive reviews by Dick Swaab and coworkers elaborate the current evidence for an array of prenatal factors that influence gender identity, including genes and hormones. 18 – 20
3.1 |. Genes
Evidence of a genetic contribution to transsexuality is very limited. 21 There are few reports of family and twin studies of transsexuals but none offer clear support for the involvement of genetic factors. 22 – 24 Polymorphisms in sex hormone-related genes for synthetic enzymes and receptors have been studied based on the assumption that these may be involved in gender identity development. An increased incidence of an A2 allele polymorphism for CYP17A1 (ie, 17ɑ-hydroxylase/17, 20 lyase, the enzyme catalysing testosterone synthesis) was found in female-to-male (FtM) but not in male-to-female (MtF) transsexuals. 25 No associations were found between a 5ɑ-reductase (ie, the enzyme converting testosterone to the more potent dihydrotestosterone) gene polymorphism in either MtF or FtM transsexuals. 26 There are also conflicting reports of associations between polymorphisms in the androgen receptor, oestrogen receptor β and CYP19 (ie, aromatase, the enzymes catalysing oestradiol synthesis). 27 – 29 A recent study using deep sequencing detected three low allele frequency gene mutants (i.e., FBXO38 [chr5:147774428; T>G], SMOC2 [chr6:169051385; A>G] and TDRP [chr8:442616; A>G]) between monozygotic twins discordant for gender dysphoria. 30 Further investigations including functional analysis and epidemiological analysis are needed to confirm the significance of the mutations found in this study. Overall, these genetic studies are inconclusive and a role for genes in gender identity remains unsettled.
3.2 |. Hormones
The evidence that prenatal hormones affect the development of gender identity is stronger but far from proven. One indication that exposure to prenatal testosterone has permanent effects on gender identity comes from the unfortunate case of David Reimer. 31 As an infant, Reimer underwent a faulty circumcision and was surgically reassigned, given hormone treatments and raised as a girl. He was never happy living as a girl and, years later, when he found out what happened to him, he transitioned to living as a man. However, for at least the first 8 months of life, this child was reared as a boy and it is not possible to know what impact rearing had on his dissatisfaction with a female sex assignment. 1 Other clinical studies have reported that male gender identity emerges in some XY children born with poorly formed or ambiguous genitals as a result of cloacal exstrophy, 5ɑ-reductase or 17β-hydroxysteroid dehydrogenase deficiency and raised as girls from birth. 32 , 33 All of these individuals were exposed to testosterone prenatally emphasising a potential role for androgens in gender development and raising doubts that children are psychosexually neutral at birth. 20 On the other hand, XY individuals born with an androgen receptor mutation causing complete androgen insensitivity are phenotypically female, identify as female and are most often androphilic, indicating that androgens act directly on the brain without the need for aromatisation to oestradiol. 34
3.3 |. Neuroanatomy
Further evidence that the organisational hormone theory applies to development of gender identity comes from observations that structural and functional brain characteristics are more similar between transgender people and control subjects with the same gender identity than between individuals sharing their biological sex. This includes local differences in the number of neurones and volume of subcortical nuclei such as the bed nucleus of the stria terminalis, 35 , 36 numbers of kisspeptin and neurokinin B neurones in the infundibulum, 37 , 38 structural differences of gray 39 , 40 and white matter microstructure, 41 – 43 neural responses to sexually-relevant odours 44 , 45 and visuospatial functioning. 46 However, in some cases, the interpretation of these studies is complicated by hormone treatments, small sample sizes and a failure to disentangle correlates of sexual orientation from gender identity. 47 The fact that these differences extend beyond brain areas and circuits classically associated with sexual and endocrine functions raises the possibility that transsexuality is also associated with changes in cerebral networks involved in self-perception.
4 |. SEXUAL ORIENTATION
Research over several decades has demonstrated that sexual orientation ranges along a continuum, from exclusive attraction to the opposite sex to exclusive attraction to the same sex. 48 However, sexual orientation is usually discussed in terms of 3 categories: heterosexual (having emotional, romantic or sexual attractions to members of the other sex), homosexual (having emotional, romantic or sexual attractions to members of one’s own sex) and bisexual (having emotional, romantic or sexual attractions to both men and women). Most people experience little or no sense of choice about their sexual orientation. There is no scientifically convincing research to show that therapy aimed at changing sexual orientation (ie, reparative or conversion therapy) is safe or effective. 3 The origin of sexual orientation is far from being understood, although there is no proof that it is affected by social factors after birth. On the other hand, a large amount of empirical data suggests that genes and hormones are important regulators of sexual orientation. 49 – 51 Useful animal models and experimental paradigms in animals have helped frame questions and propose hypotheses relevant to human sexual orientation.
4.1 |. Animal studies
Sexual partner preference is one of the most sexually dimorphic behaviours observed in animals and humans. Typically, males choose to mate with females and females choose to mate with males. Sexual partner preferences can be studied in animals by using sexual partner preference tests and recording the amount of time spent alone or interacting with the same or opposite sex stimulus animal. Although imperfect, tests of sexual partner preference or mate choice in animals have been used to model human sexual orientation. As reviewed comprehensively by Adkins-Regan 52 and Henley et al, 53 studies demonstrate that perinatal sex steroids have a large impact on organising mate choice in several species of animals, including birds, mice, rats, hamsters, ferrets and pigs. In particular, perinatal exposure to testosterone or its metabolite oestradiol programs male-typical (ie, gynophilic) partner preferences and neonatal deprivation of testosterone attenuates the preference that adult males show typically. In the absence of high concentrations of sex steroid levels or receptor-mediated activity during development, a female-typical (ie, androphilic) sexual preference for male sex partners develops.
Sexually dimorphic neural groups in the medial preoptic area of rats and ferrets have been associated with sexual partner preferences. In male rats, a positive correlation was demonstrated between the volume of the sexual dimorphic nucleus of the preoptic area (SDN) and the animal’s preference for a receptive female, 54 although this was not replicated in a recent study. 55 Furthermore, in both rats and ferrets, destruction of the SDN caused males to show either neutral or androphilic preferences. 56
Naturally occurring same-sex interactions involving genital arousal have been reported in hundreds of animal species; however, they often appear to be motivated by purposes other than sex and may serve to facilitate other social goals. 57 , 58 Exclusive and enduring same-sex orientation is, however, extremely rare among animals and has only been documented conclusively and studied systematically in certain breeds of domestic sheep. 59 , 60 Approximately 6% to 8% of Western-breed domestic rams choose to exclusively court and mount other rams, but never ewes, when given a choice. No social factors, such as the general practice of rearing in same sex groups or an animal’s dominance rank, were found to affect sexual partner preferences in rams. Consistent with the organisational theory of sexual differentiation, sheep have an ovine sexually dimorphic preoptic nucleus (oSDN) that is larger and contains more neurones in female-oriented (gynophilic) rams than in male-oriented rams (androphilic) and ewes (androphilic). 61 Thus, morphological features of the oSDN correlate with a sheep’s sexual partner preference. The oSDN already exists and is larger in males than in females before sheep are born, suggesting that it could play a causal role in behaviour. 62 The oSDN differentiates under the influence of prenatal testosterone after the male genitals develop, but is unaffected by hormone treatment in adulthood. 63 Appropriately timed experimental exposure of female lamb foetuses to testosterone can alter oSDN size independently of genetic and phenotypic sex. 13 However, males appear to be resistant to suppression of the action of androgen during gestation because the foetal hypothalamic-pituitary-axis is active in the second trimester (term pregnancy approximately 150 days) and mitigates against changes in circulating testosterone that could disrupt brain masculinisation. 64 These data suggest that, in sheep, brain sexual differentiation is initiated during gestation by central mechanisms acting through gonadotrophin-releasing hormone neurones to stimulate and maintain the foetal testicular testosterone synthesis needed to masculinise the oSDN and behaviour. More research is required to understand the parameters of oSDN development and to causally relate its function to sexual partner preferences in sheep. Nonetheless, when considered together, the body of animal research strongly indicates that male-typical partner preferences are controlled at least in part by the neural groups in the preoptic area that differentiate under the influence of pre- and perinatal sex steroids.
4.2 |. Human studies
4.2.1 |. genes.
Evidence from family and twin studies suggests that there is a moderate genetic component to sexual orientation. 50 One recent study estimated that approximately 40% of the variance in sexual orientation in men is controlled by genes, whereas, in women, the estimate is approximately 20%. 65 In 1993, Hamer et al 66 published the first genetic linkage study that suggested a specific stretch of the X chromosome called Xq28 holds a gene or genes that predispose a man to being homosexual. These results were consistent with the observations that, when there is male homosexuality in a family, there is a greater probability of homosexual males on the mother’s side of the family than on the father’s side. The study was criticised for containing only 38 pairs of gay brothers and the original finding was not replicated by an independent group. 67 Larger genome-wide scans support an association with Xq28 and also found associations with chromosome 7 and 8, 68 , 69 although this has also been disputed. 70 Scientists at the personal genomics company 23andme performed the only genome-wide association study of sexual orientation that looked within the general population. 71 The results were presented at the Annual Meeting of the American Society for Human Genetics in 2012, although they have not yet been published in a peer-reviewed journal. Although no genetic loci reaching genome-wide significance for homosexuality among men or women, the genetic marker closest to significance was located in the same region of chromosome 8 in men as that implicated in linkage studies. Other molecular genetic evidence suggests that epigenetic factors could influence male sexual orientation, although this has yet to be demonstrated. 72 , 73
4.2.2 |. Hormones
The leading biological theory of sexual orientation in humans, as in animals, draws on the application of the organisational theory of sexual differentiation. However, this theory cannot be directly tested because it is not ethical to experimentally administer hormones to pregnant women and test their effect on the sexual orientation of their children. Naturally occurring and iatrogenic disorders of sex development that involve dramatic alterations in hormone action or exposure lend some support to a role for prenatal hormones, although these cases are extremely rare and often difficult to interpret. 74 Despite these limitations, two clinical conditions are presented briefly that lend some support for the organisational theory. More comprehensive presentations of the clinical evidence on this topic can be found in several excellent reviews. 74 – 76
Women born with congenital adrenal hyperplasia (CAH) and exposed to abnormally high levels of androgens in utero show masculinised genitals, play behaviour and aggression. 74 , 77 They also are less likely to be exclusively heterosexual and report more same-sex activity than unaffected women, which suggests that typical female sexual development is disrupted. Although it appears plausible that these behavioural traits are mediated through effects of elevated androgens on the brain, it is also possible that the sexuality of CAH women may have also been impacted by the physical and psychological consequences of living with genital anomalies or more nuanced effects of socialisation. 78 There is also evidence for prenatal androgen effects on sexual orientation in XY individuals born with cloacal exstrophy. It was reported originally that a significant number of these individuals eventually adopt a male gender identity even though they had been surgically reassigned and raised as girls. Follow-up studies found that almost all of them were attracted to females (i.e. gynophilic). 33 , 50 The outcomes reported for both of these conditions are consistent with the idea that prenatal testosterone programs male-typical sexual orientation in adults. However, effects on sexual orientation were not observed across the board in all individuals with these conditions, indicating that hormones cannot be the only factor involved.
4.2.3 |. Neuroanatomy
Additional evidence that supports a prenatal organisational theory of sexual orientation is derived from the study of anatomical and physiological traits that are known to be sexually dimorphic in humans and are shown to be similar between individuals sharing the same sexual attraction. Neuroanatomical differences based on sexual orientation in human males have been found. LeVay 79 reported that the third interstitial nucleus of the anterior hypothalamus (INAH3) in homosexual men is smaller than in heterosexual men and has a similar size in homosexual men and women. Based on its position and cytoarchitecture, INAH3 resembles the sheep oSDN, which has similar differences in volume and cell density correlated with sexual partner preference. This similarity suggests that a relevant neural circuit is conserved between species. A recent review and meta-analysis of neuroimaging data from human subjects with diverse sexual interests during sexual stimulation also support the conclusion that elements of the anterior and preoptic area of the hypothalamus is part of a core neural circuit for sexual preferences. 80
Other neural and somatic biomarkers of prenatal androgen exposure have also been investigated. McFadden 81 reported that functional properties of the inner ear, measured as otoacoustic emissions (OAEs), and of the auditory brain circuits, measured as auditory evoked potentials (AEPs), differ between the sexes and between heterosexual and homosexual individuals. OAEs and AEPs are usually stronger in heterosexual women than in heterosexual men and are masculinised in lesbians, consistent with the prenatal hormone theory. However, OAEs were not different in homosexual males and AEPs appear to be hyper-masculinised. The second digit to fourth digit (2D:4D) ratio, which is the length of the second digit (index finger) relative to that of the fourth digit (ring finger), is another measure that has been used as a proxy for prenatal androgen exposure. The 2D:4D ratio is generally smaller in men than in women, 82 , 83 although the validity of this measure as a marker influenced by only prenatal androgen exposure has been questioned. 84 Nonetheless, numerous studies have reported that the 2D:4D ratio is also on average smaller in lesbians than in hetero-sexual women, a finding that has been extensively replicated 85 and suggests the testosterone plays a role in female sexual orientation. Similar to OAEs, digit ratios do not appear to be feminised in homosexual men and, similar to AEPs, may even be hyper-masculinised. The lack of evidence for reduced androgen exposure in homosexual men (based on OAEs, AEPs and digit ratios) led Breedlove 85 to speculate that there may be as yet undiscovered brain-specific reductions in androgen responses in male foetuses that grow up to be homosexual. No variations in the human androgen receptor or the aromatase gene were found that relate to variations in sexual orientation. 86 , 87 However, Balthazart and Court 88 provided suggestions for other genes located in the Xq28 region of the X-chromosome that should be explored and it remains possible that expression levels of steroid hormone response pathway genes could be regulated epigenetically (11).
4.2.4 |. Maternal immune response
Homosexual men have, on average, a greater number of older brothers than do heterosexual men, a well-known finding that has been called the fraternal birth order (FBO) effect. 89 Accordingly, the incidence of homosexuality increases by approximately 33% with each older brother. 90 The FBO effect has been confirmed many times, including by independent investigators and in non-Western sample populations. The leading hypothesis to explain this phenomenon posits that some mothers develop antibodies against a Y-linked factor important for male brain development, and that the response increases incrementally with each male gestation leading, in turn, to the alteration of brain structures underlying sexual orientation in later-born boys. In support of the immune hypothesis, Bogaert et al 91 demonstrated recently that mothers of homosexual sons, particularly those with older brothers, have higher antibody titers to neurolignin 4 (NLGN4Y), an extracellular protein involved in synaptic functioning and presumed to play a role in foetal brain development.
5 |. CONCLUSIONS
The data summarised in the present review suggest that both gender identity and sexual orientation are significantly influenced by events occurring during the early developmental period when the brain is differentiating under the influence of gonadal steroid hormones, genes and maternal factors. However, our current understanding of these factors is far from complete and the results are not always consistent. Animal studies form both the theoretical underpinnings of the prenatal hormone hypothesis and provide causal evidence for the effect of prenatal hormones on sexual orientation as modelled by tests of sexual partner preferences, although they do not translate to gender identity.
Sexual differentiation of the genitals takes place before sexual differentiation of the brain, making it possible that they are not always congruent. Structural and functional differences of hypothalamic nuclei and other brain areas differ in relation to sexual identity and sexual orientation, indicating that these traits develop independently. This may be a result of differing hormone sensitivities and/or separate critical periods, although this remains to be explored. Most findings are consistent with a predisposing influence of hormones or genes, rather than a determining influence. For example, only some people exposed to atypical hormone environments prenatally show altered gender identity or sexual orientation, whereas many do not. Family and twin studies indicate that genes play a role, but no specific candidate genes have been identified. Evidence that relates to the number of older brothers implicates maternal immune responses as a contributing factor for male sexual orientation. All of these mechanisms rely on correlations and our current understanding suffers from many limitations in the data, such as a reliance on retrospective clinical studies of individuals with rare conditions, small study populations sizes, biases in recruiting subjects, too much reliance on studies of male homosexuals, and the assumption that sexuality is easily categorised and binary. Moreover, none of the biological factors identified so far can explain all of the variances in sexual identity or orientation, nor is it known whether or how these factors may interact. Despite these limitations, the existing empirical evidence makes it clear that there is a significant biological contribution to the development of an individual’s sexual identity and sexual orientation.
ACKNOWLEDGEMENTS
I thank Charles Estill, Robert Shapiro and Fred Stormshak for their thoughtful comments on this review. This work was supported by NIH R01OD011047.
Funding information
This work was supported by NIH R01OD011047 (CER)
CONFLICT OF INTERESTS
The author declares that there are no conflicts of interest.
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- My Bibliography
- Collections
- Citation manager
Save citation to file
Email citation, add to collections.
- Create a new collection
- Add to an existing collection
Add to My Bibliography
Your saved search, create a file for external citation management software, your rss feed.
- Search in PubMed
- Search in NLM Catalog
- Add to Search
Gender identity development in children and young people: A systematic review of longitudinal studies
Affiliations.
- 1 Research and Development Unit, Tavistock and Portman NHS Foundation Trust, London, UK.
- 2 Gender Identity Development Service, Tavistock and Portman NHS Foundation Trust, London, UK.
- 3 Division of Psychiatry, University College London, UK.
- 4 Research Department of Clinical, Educational and Health Psychology, University College London, UK.
- PMID: 33827265
- DOI: 10.1177/13591045211002620
Background: Children are presenting in greater numbers to gender clinics around the world. Prospective longitudinal research is important to better understand outcomes and trajectories for these children. This systematic review aims to identify, describe and critically evaluate longitudinal studies in the field.
Method: Five electronic databases were systematically searched from January 2000 to February 2020. Peer-reviewed articles assessing gender identity and psychosocial outcomes for children and young people (<18 years) with gender diverse identification were included.
Results: Nine articles from seven longitudinal studies were identified. The majority were assessed as being of moderate quality. Four studies were undertaken in the Netherlands, two in North America and one in the UK. The majority of studies had small samples, with only two studies including more than 100 participants and attrition was moderate to high, due to participants lost to follow-up. Outcomes of interest focused predominantly on gender identity over time and emotional and behavioural functioning.
Conclusions: Larger scale and higher quality longitudinal research on gender identity development in children is needed. Some externally funded longitudinal studies are currently in progress internationally. Findings from these studies will enhance understanding of outcomes over time in relation to gender identity development in children and young people.
Keywords: Gender identity; children and young people; gender dysphoria; longitudinal; outcomes; prospective.
PubMed Disclaimer
Similar articles
- Beverage Consumption and Growth, Size, Body Composition, and Risk of Overweight and Obesity: A Systematic Review [Internet]. Mayer-Davis E, Leidy H, Mattes R, Naimi T, Novotny R, Schneeman B, Kingshipp BJ, Spill M, Cole NC, Bahnfleth CL, Butera G, Terry N, Obbagy J. Mayer-Davis E, et al. Alexandria (VA): USDA Nutrition Evidence Systematic Review; 2020 Jul. Alexandria (VA): USDA Nutrition Evidence Systematic Review; 2020 Jul. PMID: 35349233 Free Books & Documents. Review.
- Longitudinal Outcomes of Gender Identity in Children (LOGIC): study protocol for a retrospective analysis of the characteristics and outcomes of children referred to specialist gender services in the UK and the Netherlands. Kennedy E, Lane C, Stynes H, Ranieri V, Spinner L, Carmichael P, Omar R, Vickerstaff V, Hunter R, Senior R, Butler G, Baron-Cohen S, de Graaf N, Steensma TD, de Vries A, Young B, King M. Kennedy E, et al. BMJ Open. 2021 Nov 10;11(11):e054895. doi: 10.1136/bmjopen-2021-054895. BMJ Open. 2021. PMID: 34758999 Free PMC article.
- Longitudinal outcomes of gender identity in children (LOGIC): a study protocol for a prospective longitudinal qualitative study of the experiences and well-being of families referred to the UK Gender Identity Development Service. McKay K, Kennedy E, Lane C, Wright T, Young B. McKay K, et al. BMJ Open. 2021 Nov 3;11(11):e047875. doi: 10.1136/bmjopen-2020-047875. BMJ Open. 2021. PMID: 34732477 Free PMC article.
- Longitudinal Outcomes of Gender Identity in Children (LOGIC): protocol for a prospective longitudinal cohort study of children referred to the UK gender identity development service. Kennedy E, Spinner L, Lane C, Stynes H, Ranieri V, Carmichael P, Omar R, Vickerstaff V, Hunter R, Wright T, Senior R, Butler G, Baron-Cohen S, Young B, King M. Kennedy E, et al. BMJ Open. 2021 Sep 7;11(9):e045628. doi: 10.1136/bmjopen-2020-045628. BMJ Open. 2021. PMID: 34493504 Free PMC article.
- IMPRoving Outcomes for children exposed to domestic ViolencE (IMPROVE): an evidence synthesis. Howarth E, Moore THM, Welton NJ, Lewis N, Stanley N, MacMillan H, Shaw A, Hester M, Bryden P, Feder G. Howarth E, et al. Southampton (UK): NIHR Journals Library; 2016 Dec. Southampton (UK): NIHR Journals Library; 2016 Dec. PMID: 27977089 Free Books & Documents. Review.
- Early Female Transgender Identity after Prenatal Exposure to Diethylstilbestrol: Report from a French National Diethylstilbestrol (DES) Cohort. Gaspari L, Soyer-Gobillard MO, Kerlin S, Paris F, Sultan C. Gaspari L, et al. J Xenobiot. 2024 Jan 12;14(1):166-175. doi: 10.3390/jox14010010. J Xenobiot. 2024. PMID: 38249107 Free PMC article.
- Consistency of gender identity and preferences across time: An exploration among cisgender and transgender children. Hässler T, Glazier JJ, Olson KR. Hässler T, et al. Dev Psychol. 2022 Nov;58(11):2184-2196. doi: 10.1037/dev0001419. Epub 2022 Aug 11. Dev Psychol. 2022. PMID: 35951394 Free PMC article.
Publication types
- Search in MeSH
LinkOut - more resources
Full text sources.
- Ovid Technologies, Inc.
Other Literature Sources
- scite Smart Citations

- Citation Manager
NCBI Literature Resources
MeSH PMC Bookshelf Disclaimer
The PubMed wordmark and PubMed logo are registered trademarks of the U.S. Department of Health and Human Services (HHS). Unauthorized use of these marks is strictly prohibited.
Diverse Gender Identity Development: A Qualitative Synthesis and Development of a New Contemporary Framework
- Original Article
- Published: 11 December 2023
- Volume 90 , pages 1–18, ( 2024 )
Cite this article

- Molly Speechley ORCID: orcid.org/0000-0003-4056-5404 1 ,
- Jaimee Stuart ORCID: orcid.org/0000-0002-4376-1913 2 &
- Kathryn L. Modecki ORCID: orcid.org/0000-0002-9937-9748 3
878 Accesses
6 Altmetric
Explore all metrics
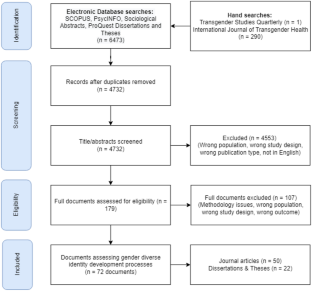
Traditional models of gender identity development for individuals who do not identify with their assigned birth sex have generally treated medical intervention as normative, and non-binary identification as relatively rare. However, changing demographics within gender diverse populations have highlighted the need for an updated framework of gender identity development. To address this gap in the research, this study systematically reviewed the qualitative literature assessing the lived experiences of identity development of over 1,758 gender diverse individuals, across 72 studies. Reflexive thematic analysis of excerpts were synthesised to produce a novel, integrative perspective on identity development, referred to as the Diverse Gender Identity Framework. The framework is inclusive of binary and non-binary identities and characterises the distinctive identity processes individuals undergo across development.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Subscribe and save.
- Get 10 units per month
- Download Article/Chapter or Ebook
- 1 Unit = 1 Article or 1 Chapter
- Cancel anytime
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
Similar content being viewed by others

Gender Identity as a Social Developmental Process

“Like a Constantly Flowing River”: Gender Identity Flexibility Among Nonbinary Transgender Individuals

Not by Convention: Working with People on the Sexual and Gender Continuum
Baker, G. (2014). Adult transgender perspectives on identity development [Doctoral dissertation, Walden University].
Balius, A. (2018). “I want to be who I am”: Stories of rejecting binary gender [Master’s thesis, University of South Florida]. https://www.proquest.com/docview/2093878022
Beagan, B. L., de Souza, L., Godbout, C., Hamilton, L., MacLeod, J., Paynter, E., & Tobin, A. (2012). “This is the biggest thing you’ll ever do in your life”: Exploring the occupations of transgendered people. Journal of Occupational Science, 19 (3), 226–240. https://doi.org/10.1080/14427591.2012.659169
Article Google Scholar
Bem, S. L. (1981). Gender schema theory: A cognitive account of sex typing. Psychological Review, 88 (4), 354–364. https://doi.org/10.1037/0033-295X.88.4.354
Bockting, W. O., & Coleman, E. (2007). Developmental stages of the transgender coming out process: Toward an integrated identity. In R. Ettner, S. Monstrey, & A. E. Eyler (Eds.), Principles of transgender medicine and surgery (pp. 185–208). Routledge.
Google Scholar
Boddington, E. (2016). A qualitative exploration of gender identity in young people who identify as neither male nor female [Doctoral dissertation, University of East London]. https://repository.uel.ac.uk/item/85119
Bradford, N. J., & Syed, M. (2019). Transnormativity and transgender identity development: A master narrative approach. Sex Roles, 81 (5–6), 306–325. https://doi.org/10.1007/s11199-018-0992-7
Bradford, N. J., Rider, G. N., Catalpa, J. M., Morrow, Q. J., Berg, D. R., Spencer, K. G., & McGuire, J. K. (2019). Creating gender: A thematic analysis of genderqueer narratives. International Journal of Transgenderism, 20 (2–3), 155–168. https://doi.org/10.1080/15532739.2018.1474516
Article PubMed Google Scholar
Braun, V., & Clarke, V. (2021). Thematic analysis: A practical guide . Sage.
Brown, C., Dashjian, L. T., Acosta, T. J., Mueller, C. T., Kizer, B. E., & Trangsrud, H. B. (2013). Learning from the life experiences of male-to-female transsexuals. Journal of GLBT Family Studies, 9 (2), 105–128. https://doi.org/10.1080/1550428X.2013.765247
Carlile, A., Butteriss, E., & Sansfaçon, A. P. (2021). “It’s like my kid came back overnight”: Experiences of trans and non-binary young people and their families seeking, finding and engaging with clinical care in England. International Journal of Transgender Health, 22 (4), 412–424. https://doi.org/10.1080/26895269.2020.1870188
Article PubMed PubMed Central Google Scholar
Clark, B. A., Veale, J. F., Townsend, M., Frohard-Dourlent, H., & Saewyc, E. (2018). Non-binary youth: Access to gender-affirming primary health care. International Journal of Transgenderism, 19 (2), 158–169. https://doi.org/10.1080/15532739.2017.1394954
Coleman, E. (1982). Developmental stages of the coming out process. Journal of Homosexuality, 7 (2–3), 31–43. https://doi.org/10.1300/J082v07n02_06
Coleman, E., Radix, A. E., Bouman, W. P., Brown, G. R., de Vries, A. L. C., Deutsch, M. B., Ettner, R., Fraser, L., Goodman, M., Green, J., Hancock, A. B., Johnson, T. W., Karasic, D. H., Knudson, G. A., Leibowitz, S. F., Meyer-Bahlburg, H. F. L., Monstrey, S. J., Motmans, J., Nahata, L., & Arcelus, J. (2022). Standards of care for the health of transgender and gender diverse people, version 8. International Journal of Transgender Health, 23 (S1), S1–S259. https://doi.org/10.1080/26895269.2022.2100644
Critical Appraisal Skills Programme. (2019). CASP qualitative checklist . Critical Appraisal Skills Programme. https://casp-uk.net/casp-tools-checklists/
Crocetti, E., Rubini, M., Luyckx, K., & Meeus, W. (2008). Identity formation in early and middle adolescents from various ethnic groups: From three dimensions to five statuses. Journal of Youth and Adolescence, 37 (8), 983–996. https://doi.org/10.1007/s10964-007-9222-2
Devor, A. H. (2004). Witnessing and mirroring: A fourteen stage model of transsexual identity formation. Journal of Gay and Lesbian Psychotherapy, 8 (1–2), 41–67. https://doi.org/10.1300/J236v08n01_05
Downing, J. B. (2013). Trans identity construction: Reconstituting the body, gender, and sex [Doctoral dissertation, Clark University]. https://www.proquest.com/docview/1334957140
Ehrhardt, A. A., Grisanti, G., & McCauley, E. A. (1979). Female-to-male transsexuals compared to lesbians: Behavioral patterns of childhood and adolescent development. Archives of Sexual Behavior, 8 (6), 481–490. https://doi.org/10.1007/BF01541415
Eisenberg, E., & Zervoulis, K. (2020). All flowers bloom differently: An interpretative phenomenological analysis of the experiences of adult transgender women. Psychology and Sexuality, 11 (1–2), 120–134. https://doi.org/10.1080/19419899.2019.1661278
Evans, J. L. (2010). Genderqueer identity and self-perception [Doctoral dissertation, Alliant International University]. https://www.proquest.com/docview/745602050
Gagné, P., Tewksbury, R., & McGaughey, D. (1997). Coming out and crossing over identity formation and proclamation in a transgender community. Gender and Society, 11 (4), 478–508. https://doi.org/10.1177/089124397011004006
Goldberg, A. E., & Kuvalanka, K. A. (2018). Navigating identity development and community belonging when “there are only two boxes to check”: An exploratory study of nonbinary trans college students. Journal of LGBT Youth, 15 (2), 106–131. https://doi.org/10.1080/19361653.2018.1429979
Goodman, M., Adams, N., Corneil, T., Kreukels, B., Motmans, J., & Coleman, E. (2019). Size and distribution of transgender and gender nonconforming populations. Endocrinology and Metabolism Clinics of North America, 48 (2), 303–321. https://doi.org/10.1016/j.ecl.2019.01.001
Graham, L. F., Crissman, H. P., Tocco, J., Hughes, L. A., Snow, R. C., & Padilla, M. B. (2014). Interpersonal relationships and social support in transitioning narratives of Black transgender women in Detroit. International Journal of Transgenderism, 15 (2), 100–113. https://doi.org/10.1080/15532739.2014.937042
Gridley, S. J., Crouch, J. M., Evans, Y., Eng, W., Antoon, E., Lyapustina, M., Schimmel-Bristow, A., Woodward, J., Dundon, K., Schaff, R. N., McCarty, C., Ahrens, K., & Breland, D. J. (2016). Youth and caregiver perspectives on barriers to gender-affirming health care for transgender youth. Journal of Adolescent Health, 59 (3), 254–261. https://doi.org/10.1016/j.jadohealth.2016.03.017
Gülgöz, S., Glazier, J. J., Enright, E. A., Alonso, D. J., Durwood, L. J., Fast, A. A., Lowe, R., Ji, C., Heer, J., Martin, C. L., & Olson, K. R. (2019). Similarity in transgender and cisgender children’s gender development. Proceedings of the National Academy of Sciences of the United States of America, 116 (49), 24480–24485. https://doi.org/10.1073/pnas.1909367116
Hawkins, L. A. (2009). Gender identity development among transgender youth: A qualitative analysis of contributing factors [Doctoral dissertation, Widener University]. https://www.proquest.com/docview/305248568
Johnson, A. H. (2016). Transnormativity: A new concept and its validation through documentary film about transgender men. Sociological Inquiry, 86 (4), 465–491. https://doi.org/10.1111/soin.12127
Kalra, G. (2012). Hijras: The unique transgender culture of India. International Journal of Culture and Mental Health, 5 (2), 121–126. https://doi.org/10.1080/17542863.2011.570915
Katz-Wise, S. L., & Budge, S. L. (2015). Cognitive and interpersonal identity processes related to mid-life gender transitioning in transgender women. Counselling Psychology Quarterly, 28 (2), 150–174. https://doi.org/10.1080/09515070.2014.993305
Kennedy, N. (2022). Deferral: The sociology of young trans people’s epiphanies and coming out. Journal of LGBT Youth, 19 (1), 53–75. https://doi.org/10.1080/19361653.2020.1816244
Laljer, D. (2017). Comparing media usage of binary and non-binary transgender individuals when discovering and describing gender identity [Master’s thesis, University of North Texas]. https://www.proquest.com/docview/2009056791
Lambrou, N. H. (2018). Trans masculine identities: Making meaning in gender and transition [Doctoral dissertation, The University of Wisconsis-Milwaukee]. https://www.proquest.com/docview/2108647669
le Roux, N. (2013). Gender variance in childhood/adolescence: Gender identity journeys not involving physical intervention [Doctoral dissertation, University of East London]. https://repository.uel.ac.uk/item/85vvw
Lev, A. I. (2004). Transgender emergence: A developmental process. In T. Trepper (Ed.), Transgender emergence : Therapeutic guidelines for working with gender-variant people and their families (pp. 229–269). The Haworth Clinical Practice Press.
Levitt, H. M. (2019). A psychosocial genealogy of LGBTQ+ gender: An empirically based theory of gender and gender identity cultures. Psychology of Women Quarterly, 43 (3), 275–297. https://doi.org/10.1177/0361684319834641
Losty, M., & O’Connor, J. (2018). Falling outside of the ‘nice little binary box’: A psychoanalytic exploration of the non-binary gender identity. Psychoanalytic Psychotherapy, 32 (1), 40–60. https://doi.org/10.1080/02668734.2017.1384933
Marcia, J. E. (1966). Development and validation of ego-identity status. Journal of Personality and Social Psychology, 3 (5), 551–558.
Matsuno, E., Bricker, N. L., Savarese, E., Mohr, R., & Balsam, K. F. (2022). “The default is just going to be getting misgendered”: Minority stress experiences among nonbinary adults. Psychology of Sexual Orientation and Gender Diversity . https://doi.org/10.1037/sgd0000607
McCarthy, L. (2003). Off that spectrum entirely: A study of female-bodied transgender-identified individuals [Doctoral dissertation, University of Massachusetts Amherst]. https://www.proquest.com/docview/305322146
Medico, D., Pullen Sansfaçon, A., Zufferey, A., Galantino, G., Bosom, M., & Suerich-Gulick, F. (2020). Pathways to gender affirmation in trans youth: A qualitative and participative study with youth and their parents. Clinical Child Psychology and Psychiatry, 25 (4), 1002–1014. https://doi.org/10.1177/1359104520938427
Money, J., & Primrose, C. (1968). Sexual dimorphism and dissociation in the psychology of male transsexuals. The Journal of Nervous and Mental Disease, 147 (5), 472–486. https://doi.org/10.1097/00005053-196811000-00004
Morgan, S. W., & Stevens, P. E. (2008). Transgender identity development as represented by a group of female-to-male transgendered adults. Issues in Mental Health Nursing, 29 (6), 585–599. https://doi.org/10.1080/01612840802048782
Mullen, G., & Moane, G. (2013). A qualitative exploration of transgender identity affirmation at the personal, interpersonal, and sociocultural levels. International Journal of Transgenderism, 14 (3), 140–154. https://doi.org/10.1080/15532739.2013.824847
Noblit, G. W., & Hare, R. D. (1988). Meta-ethnography: Synthesizing qualitative studies . Sage.
Book Google Scholar
Oakley, A. (2016). Disturbing hegemonic discourse: Nonbinary gender and sexual orientation labeling on Tumblr. Social Media and Society, 2 (3). https://doi.org/10.1177/2056305116664217
Opromalla, J. A. (2019). Transgender young adults’ negotiation of gender consciousness in relation to others’ behaviors and attitudes [Doctoral dissertation, Fordham University]. https://www.proquest.com/docview/2239312970
Ouzzani, M., Hammady, H., Fedorowicz, Z., & Elmagarmid, A. (2016). Rayyan—a web and mobile app for systematic reviews. Systematic Reviews, 5 (1), 210. https://doi.org/10.1186/s13643-016-0384-4
Patel, E. (2019). Understanding gender identity development in gender variant birth-assigned female adolescents with autism spectrum conditions [Doctoral dissertation, University College London]. https://discovery.ucl.ac.uk/id/eprint/10083597/
Penklis, H. S. (2020). “Celebrated, not tolerated”: How transgender and nonbinary individuals navigate the social world [Master’s thesis, The University of Texas at El Paso]. https://www.proquest.com/docview/2424094395
Pollock, L., & Eyre, S. L. (2012). Growth into manhood: Identity development among female-to-male transgender youth. Culture, Health & Sexuality, 14 (2), 209–222. https://doi.org/10.1080/13691058.2011.636072
Pullen Sansfaçon, A., Medico, D., Suerich-Gulick, F., & Temple Newhook, J. (2020). “I knew that I wasn’t cis, I knew that, but I didn’t know exactly”: Gender identity development, expression and affirmation in youth who access gender affirming medical care. International Journal of Transgender Health, 21 (3), 307–320. https://doi.org/10.1080/26895269.2020.1756551
QSR International Pty Ltd. (2020). NVivo (March 2020). https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home
Rankin, S., & Beemyn, G. (2012). Beyond a binary: The lives of gender-nonconforming youth. About Campus: Enriching the Student Learning Experience, 17 (4), 2–10. https://doi.org/10.1002/abc.21086
Rood, B. A., Reisner, S. L., Puckett, J. A., Surace, F. I., Berman, A. K., & Pantalone, D. W. (2017). Internalized transphobia: Exploring perceptions of social messages in transgender and gender-nonconforming adults. International Journal of Transgenderism, 18 (4), 411–426. https://doi.org/10.1080/15532739.2017.1329048
Sakai, C. (2003). Identity development in female-to-male transsexuals: A qualitative study [Doctoral dissertation, Alliant International University]. https://www.proquest.com/docview/305213596
Schimmel-Bristow, A., Haley, S. G., Crouch, J. M., Evans, Y. N., Ahrens, K. R., McCarty, C. A., & Inwards-Breland, D. J. (2018). Youth and caregiver experiences of gender identity transition: A qualitative study. Psychology of Sexual Orientation and Gender Diversity, 5 (2), 273–281. https://doi.org/10.1037/sgd0000269
Schneider, J., Page, J., & van Nes, F. (2019). “Now I feel much better than in my previous life”: Narratives of occupational transitions in young transgender adults. Journal of Occupational Science, 26 (2), 219–232. https://doi.org/10.1080/14427591.2018.1550726
Schulz, S. L. (2012). Gender identity: Pending? Identity development and health care experiences of transmasculine/genderqueer identified individuals [Doctoral dissertation, University of California]. https://www.proquest.com/docview/1322090378
Stryker, S. (2017). Transgender history: The roots of today’s revolution (Revised) . Seal Press.
Tan, S. (2019). Lived experience of Asian transgender youth in Canada: An intersectional framework [Doctoral dissertation, Adler University]. https://www.proquest.com/docview/2312892674
Valle, J. (2020). A qualitative study of the trans fem community: Exploring trans identity formation, familial support, and relationships with food [Doctoral dissertation, Alliant International University]. https://www.proquest.com/docview/2476835074
Ward, K. (2019). Building an identity despite discrimination: A linguistic analysis of the lived experiences of gender variant people in North East England [Doctoral dissertation, University of Sunderland]. https://sure.sunderland.ac.uk/id/eprint/10874/%0A
Weisgram, E. S. (2016). The cognitive construction of gender stereotypes: Evidence for the dual pathways model of gender differentiation. Sex Roles, 75 (7–8), 301–313. https://doi.org/10.1007/s11199-016-0624-z
Wright, K. A. (2011). Transgender identity formation [Doctoral dissertation, The Chicago School of Professional Psychology]. https://www.proquest.com/docview/1411944798
Download references
Acknowledgements
This work was supported by the Society for the Psychological Study of Social Issues as part of the 2021 Spring Grand-in-Aid program; and an Australian Government Research Training Program (RTP) Scholarship, granted to the first author.
Author information
Authors and affiliations.
School of Applied Psychology, Griffith University, Brisbane, Australia
Molly Speechley
United Nations University, Macao, China
Jaimee Stuart
Centre for Mental Health, Griffith University, Brisbane, Australia
Kathryn L. Modecki
You can also search for this author in PubMed Google Scholar
Contributions
Conceptualization: Molly Speechley, Jaimee Stuart, Kathryn Modecki; Methodology: Molly Speechley, Jaimee Stuart; Formal analysis and investigation: Molly Speechley; Writing—original draft preparation: Molly Speechley; Writing—review and editing: Molly Speechley, Jaimee Stuart, Kathryn Modecki; Funding acquisition: Molly Speechley, Kathryn Modecki; Supervision: Jaimee Stuart, Kathryn Modecki.
Corresponding author
Correspondence to Molly Speechley .
Ethics declarations
Ethical approval and consent to participate.
Not applicable.
Human and Animal Ethics
Consent for publication.
All authors consent to publication of the manuscript.
Availability of supporting data
All data analysed during this study are included in its supplementary information files.
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (DOCX 116 KB)
Rights and permissions.
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Speechley, M., Stuart, J. & Modecki, K.L. Diverse Gender Identity Development: A Qualitative Synthesis and Development of a New Contemporary Framework. Sex Roles 90 , 1–18 (2024). https://doi.org/10.1007/s11199-023-01438-x
Download citation
Accepted : 26 October 2023
Published : 11 December 2023
Issue Date : January 2024
DOI : https://doi.org/10.1007/s11199-023-01438-x
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Gender diversity
- Developmental experiences
- Identity development
- Non-binary identity
- Qualitative review
- Transgender
- Find a journal
- Publish with us
- Track your research
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Open access
- Published: 01 September 2020
Fluidity of gender identity induced by illusory body-sex change
- Pawel Tacikowski 1 , 2 ,
- Jens Fust ORCID: orcid.org/0000-0002-4706-092X 1 , 3 &
- H. Henrik Ehrsson ORCID: orcid.org/0000-0003-2333-345X 1
Scientific Reports volume 10 , Article number: 14385 ( 2020 ) Cite this article
34k Accesses
31 Citations
144 Altmetric
Metrics details
- Cognitive neuroscience
- Human behaviour
Gender identity is a collection of thoughts and feelings about one’s own gender, which may or may not correspond to the sex assigned at birth. How this sense is linked to the perception of one’s own masculine or feminine body remains unclear. Here, in a series of three behavioral experiments conducted on a large group of control volunteers (N = 140), we show that a perceptual illusion of having the opposite-sex body is associated with a shift toward a more balanced identification with both genders and less gender-stereotypical beliefs about own personality characteristics, as indicated by subjective reports and implicit behavioral measures. These findings demonstrate that the ongoing perception of one’s own body affects the sense of one’s own gender in a dynamic, robust, and automatic manner.
Similar content being viewed by others

Daily gender expression is associated with psychological adjustment for some people, but mainly men

Male recognition bias in sex assignment based on visual stimuli

Male sexual orientation, gender nonconformity, and neural activity during mental rotations: an fMRI study
Introduction.
Gender identity is a collection of thoughts and feelings about one’s own gender, which may or may not correspond to the sex assigned at birth 1 , 2 , 3 , 4 , 5 . This multifaceted, subjective sense of being male, female, both, or neither occurs in our conscious self-awareness, but the associated perceptions and beliefs can also be largely implicit 3 , 4 , 5 . In the past, gender identity was conceptualized as a male–female dichotomy; however, current theories consistently postulate that gender identity is a spectrum of associations with both genders 1 , 3 , 4 , 5 , 6 . There is also a general consensus in the field that gender identity is determined by multiple factors, such as person’s genes, hormones, patterns of behaviors, or social interactions 4 , 5 , 6 , 7 , 8 ; and that the sense of own gender (e.g., “I’m male”) is closely linked to one’s beliefs about males and females in general (e.g., “males are competitive”), as well as to the associated beliefs about own personality (“I am competitive”) 1 , 3 , 6 . The specific content of such beliefs and their strength contribute to what it means for a given person to be male or female in a given sociocultural context, which in some cases hinders the realization of one’s full personal or professional potential. Although gender identity has a profound impact on our lives, little is known about how this sense is formed or maintained. A better understanding of the neurocognitive mechanisms of gender identity is also important in the context of gender dysphoria (DSM-5 9 ; gender incongruence ICD-11 10 ), which is characterized by the prolonged and clinically relevant distress that some transgender individuals experience due to inconsistency between their sex assigned at birth and their subjective sense of gender.
Various observations suggest that gender identity and the perception of one’s own body are tightly connected. For example, people with gender dysphoria (see above) often avoid looking in the mirror, hide their bodies under loose-fitting clothes, and seek hormonal and/or surgical procedures to adjust their physical appearance to meet their subjective sense of own gender 6 , 11 , 12 . Moreover, among individuals whose gender identity matches their sex assigned at birth, mastectomy and androgen deprivation cancer therapies, which both involve changes to one’s feminine or masculine bodily characteristics, are often related to a gender identity crisis 13 , 14 . There are also data suggesting that the mental representation of one’s own body is altered in transgender individuals 15 and that the brain regions involved in this representation are anatomically and functionally different in this group compared to controls 16 , 17 , 18 , 19 , 20 , 21 , 22 , 23 . However, the link between own body perception and gender identity remains poorly understood from a behavioral experimental perspective, and we do not know whether, and if so how, the perceived sex of own body influences the sense of own gender in nontransgender individuals.
The full-body ownership illusion 24 is a powerful experimental tool for manipulating the perception of one’s own body 25 , 26 , 27 , 28 , 29 , 30 . During this illusion, the participants wear head-mounted displays (HMDs) and observe a stranger’s body from a first-person perspective. The stranger’s body is continuously stroked with a stick or a brush, and the experimenter applies synchronous touches on the corresponding parts of the participant’s body, which is out of view. Synchronous visuotactile stimulation induces a feeling that the stranger’s body is one’s own, whereas asynchronous stimulation breaks the illusion and serves as a well-matched control condition 24 , 31 , 32 , 33 . The full-body ownership illusion, similar to the rubber hand illusion involving a single limb 34 , 35 , 36 , 37 , occurs when visual, tactile, proprioceptive, and other sensory signals from the body are combined at the central level into a coherent multisensory representation of one’s own body 24 , 25 , 26 , 30 . Body ownership illusions involving limbs 37 and full bodies 31 , 33 , 38 are related to increased neural activity in regions of the frontal and parietal association cortices that are related to multisensory integration, such as the premotor and intraparietal cortices. Because these brain regions contain trimodal neurons that integrate visual, tactile, and proprioceptive signals and because body illusions closely follow the temporal and spatial constraints of multisensory integration, it has been proposed that combining bodily signals from different modalities is a key mechanism for attributing ownership to our bodies 25 , 26 , 27 , 28 , 29 , 30 . The full-body illusion has been replicated in numerous studies 24 , 31 , 32 , 33 , 39 , 40 , 41 , 42 , 43 , 44 , 45 , even with bodies of a sex opposite to that of the participants 24 , 43 , but the cognitive consequences of this transient physical sex change on gender identity have not been assessed.
Here, we conducted three within-subject behavioral experiments on a total of one hundred forty naïve control volunteers to investigate a possible dynamic relationship between the perception of own body and the sense of own gender. In all three experiments, we induced the “body-sex-change illusion”, which is analogous to the standard full-body illusion (see earlier), but in the HMDs, the participants observe the opposite-sex stranger’s body (Movies S1 and S2). Thus, we aimed to experimentally manipulate how the participants perceived the secondary sex characteristics of their own bodies to measure what outcome this manipulation has on different aspects of gender identity. Specifically, in Experiment I, we asked the participants to rate how masculine or feminine they felt after the body-sex-change illusion to assess the subjective and conscious facets of gender identity. Explicit methods such as the one above provide information about participants’ phenomenological experience, but ideally, they should be combined with objective tests to provide more conclusive results. Therefore, in Experiment II, we used a well-controlled behavioral method—the Implicit Association Test (IAT)—to measure the cognitive and implicit aspects of gender identity; this test is largely immune to conscious strategies 46 and has been validated for gender identity research in control 47 , 48 as well as in transgender individuals 48 . Finally, in Experiment III, we tested whether the perception of own body affects gender-related beliefs about own personality (see earlier) by asking the participants to rate after the illusion how much different traits, stereotypically related to males and females, pertain to their own personality. Applying such different measurements aimed to capture the multifaceted character of the sense of own gender (see earlier), while using continuous scales in all experiments addressed gender identity as a spectrum (see earlier). We hypothesized that if own body perception dynamically shapes gender identity, then even a brief transformation of one’s own perceived physical sex during the body-sex-change illusion should shift different aspects of gender identity toward the opposite gender.
Experiment I tested whether the perception of one’s own body dynamically shapes one’s subjective feeling of masculinity/femininity. The experiment comprised a two-by-two factorial design with four conditions (Fig. 1 a): “synchronous opposite sex” (syncO), “synchronous same sex” (syncS), “asynchronous opposite sex” (asyncO), and “asynchronous same sex” (asyncS). This design allowed us to manipulate the sex-related characteristics of the perceived bodily self in the body-sex-change illusion condition (syncO) while controlling for potential confounding factors related to experiencing a full-body ownership illusion itself (syncS) or cognitive biases due to simply looking at a male or female body (asyncS, asyncO). We measured the illusion psychometrically by asking the participants to rate their subjective experience of owning the stranger’s body (Fig. 1 b) and objectively by recording the participants’ physiological fear reactions (skin conductance responses) when the stranger’s body was physically threatened with a knife (Fig. 1 c). Both of these illusion measures should be higher during the synchronous than during the asynchronous conditions 24 , 32 , 38 , 39 , 42 . Importantly, before experiencing any body perception manipulation (baseline) and after every full-body illusion condition, the participants rated how masculine or feminine they felt (Fig. 1 d,e).

Perceptual illusion of having the opposite-sex body modulated the subjective experience of feeling masculine or feminine (Experiment I). ( a ) The participants (N = 32; 15 females) lay on a bed and wore a head-mounted display in which a body of an unknown male or female was shown from a first-person perspective (the participant’s real body was out of view). Video frames illustrate all four conditions for a male participant (top picture). For a female participant, the videos from the lower and upper rows would be swapped. In the synchronous conditions, touches applied to the participant and touches applied to the stranger’s body were matched (see the red triangle), whereas in the asynchronous conditions, touches applied to the participants were delayed by 1 s. We expected to induce the body-sex-change illusion specifically in the syncO condition, and the other conditions served as controls. ( b ) After each condition, the participants rated illusion (I1:I3) and control (C1:C4) statements on a 7-point scale (− 3—“strongly disagree”; + 3— “strongly agree”). The illusion statements assessed the feeling that the stranger’s body is one’s own, whereas the control statements controlled for any potential effects of suggestibility or task compliance. ( c ) Genuine ownership of the stranger’s body should be associated with increased physiological stress responses of the participant when the stranger’s body is physically threatened. Thus, we measured the participants’ skin conductance responses elicited by brief “knife threat” events that occurred in the videos. ( d ) Before the experiment (baseline) and after each condition, the participants rated how feminine or masculine they felt. The upper row shows scale assignment for female participants and the lower row for males. ( e ) The order of conditions was counterbalanced across the participants, and the whole experiment lasted ~ 30 min. ( f ) The illusion ratings and the magnitude of skin conductance responses were significantly higher in the synchronous than in the asynchronous conditions, which shows that the full-body ownership illusion was elicited as expected. ( g ) During syncO, the female participants indicated feeling less feminine, and the male participants indicated feeling less masculine than during other conditions. ( h ) Strong illusory ownership of the opposite-sex body was related to a significant shift toward the opposite gender, specifically in syncO. For clarity of display, only ratings from syncO and asyncO are shown; syncS, asyncS, and baseline are colored in gray for comparison. ( i ) The participants who experienced a strong body-sex-change illusion (above-median I1 ownership ratings: syncO–asyncO; N = 12) indicated feeling more masculine (females) or more feminine (males) during syncO than during other conditions. Plots show means ± SE.
The full-body ownership illusion was induced as expected, that is, “illusion scores” [illusion questionnaire ratings: (I1 + I2 + I3)/3 + (C1 + C2 + C3 + C4)/4] were higher in the synchronous than in the asynchronous conditions, and knife threats during the synchronous conditions triggered stronger skin conductance responses than knife threats during the asynchronous conditions (Fig. 1 f; Table S2 ; main effect of synchrony; illusion scores: F 1,32 = 64.48; P < 0.005; skin conductance: F 1,27 = 10.98; P < 0.005; two-sided; N = 32). With regard to our main hypothesis, we found that during syncO, female participants indicated feeling significantly less feminine and male participants significantly less masculine than during the baseline, syncS, and asyncS control conditions; the difference between syncO and asyncO showed a significant trend in the hypothesized direction (Fig. 1 g; Tables S2 and S3 ). Importantly, the shift toward the opposite gender, specifically in the syncO condition, was enhanced by the illusory ownership of the opposite-sex body (Fig. 1 h; Tables S2 and S3 ; synchrony × body × ownership: F 1,32 = 8.05; P = 0.008; main effect of ownership in syncO: b = − 0.6; SE = 0.2; t 30 = − 2.29; P = 0.022; two-sided; N = 32). Please note that “ownership” in the analysis above corresponds to I1 questionnaire ratings: syncO—asyncO (one value per participant). Moreover, we found that the participants who experienced a strong body-sex-change illusion (N = 12; median-split; see “ Materials and methods ”) indicated feeling more like the opposite gender in syncO compared to the other conditions (Fig. 1 i; Tables S2 and S3 ). Overall, Experiment I shows that the ongoing perception of one’s own body dynamically updates one’s subjective feelings of masculinity or femininity.
Experiment II tested whether the perceived sex of one’s own body also modulates implicit associations between oneself and gender categories. This experiment had the same two-by-two factorial design as Experiment I (Fig. 1 a), but this time, gender identity was measured with the IAT 47 , 48 . During this test, the participants heard words belonging to four semantic categories ( male , female , self , or other ) and sorted these words into just two response categories. In one block, the participants responded with the same key to words from the self and female categories, which made this block congruent for females and incongruent for males. In the other block, the participants responded with the same key to words from the self and male categories, which made this block incongruent for females and congruent for males (Fig. 2 b). Faster responses in the congruent block than in the incongruent block (i.e., congruent block being cognitively less demanding) indicate that a given person associates with the gender that is consistent with his/her sex. In turn, longer reaction times in the congruent block suggest an inclination toward the opposite gender, whereas similar responses in both blocks suggest a balanced gender identity. Thus, the IAT provides a fine-grained behavioral proxy of where a person is located on a gender identity spectrum (see “ Introduction ”). The participants performed the IAT four times, once during each condition, which allowed us to track changes in implicit gender identification across different embodiment contexts (Fig. 2 c).

The body-sex-change illusion balanced implicit associations between the self and both genders (Experiment II). ( a ) This experiment (N = 64; 32 females) comprised the same four conditions as Experiment I (Fig. 1 a), but we used recordings of a different male and female body to enhance the generalizability of our findings. ( b ) The left panel is a schematic representation of the congruent IAT block for the female participants (incongruent for males), as words from the self and female categories are assigned to the same response category (left arrow). The right panel shows the IAT block that is incongruent for the female participants and congruent for males. Please note that exactly the same words are used in both blocks, only the instructions (key assignment) are different. ( c ) During each condition, the participants completed one full IAT (two blocks). The condition order and block order were counterbalanced across participants. The whole experiment lasted ~ 60 min. ( d ) The body-sex-change illusion was successfully induced, as shown by questionnaire data and the magnitude of threat-evoked skin conductance responses. ( e ) In all conditions, reaction times were significantly shorter in the congruent than in the incongruent IAT blocks, which shows that it was generally easier for the participants to associate themselves with the gender consistent with their sex. ( f ) Strong illusory ownership of the opposite-sex body was related to the balancing of implicit associations between the self and both genders, specifically in syncO. For clarity of display, individual data points are not shown (n = 7,290). ( g ) The participants who experienced a strong body-sex-change illusion (above-median I1 ownership ratings: syncO–asyncO; N = 24) responded similarly quickly in the incongruent and congruent IAT blocks during syncO. Bar plots show means ± SE.
The body-sex-change illusion was also successfully induced in Experiment II, as demonstrated by the questionnaire and skin conductance data (Fig. 2 d; Table S4 ; main effect of synchrony; illusion scores: F 1,64 = 125.65; P < 0.005; skin conductance: F 1,60 = 4.97; P = 0.03; two-sided; N = 64). In all conditions, it was easier for the participants to associate themselves with the gender consistent with their sex, as indicated by shorter reaction times in the congruent than in the incongruent blocks (Fig. 2 e; Tables S4 and S5 ). More importantly, however, strong illusory ownership of the opposite-sex body was related to a reduced difference between the incongruent and congruent blocks specifically in syncO, which shows that the illusion balanced the strength of implicit associations between the self and both genders (Fig. 2 f; Table S4 ; synchrony × body × congruence × ownership: F 1,28878 = 17.03; P < 0.005; congruence × ownership in syncO: F 1,7207 = 9.37; P < 0.005; two-sided; N = 64). Furthermore, the participants who experienced strong illusory ownership of the opposite-sex body (N = 24; median-split; see “ Materials and methods ”) had similar reaction times in the congruent and incongruent IAT blocks during syncO (Fig. 2 g; Tables S4 and S5 ). Thus, the main finding of Experiment II is that the moment-to-moment perception of one’s own body balances the strength of implicit associations between the self and both genders.
Experiment III investigated whether the illusion-induced fluidity of gender identity is generalized to gender-related beliefs about one’s own personality (see “ Introduction ”). This experiment consisted of two conditions (syncO and asyncO); thus, in the HMDs, female participants always observed a male body, and male participants always observed a female body (Fig. 3 a,b). After each condition, the participants filled out a short version of the Bem Sex-Role Inventory (BSRI) 49 , 50 that contained personality characteristics stereotypically associated with males and females (Fig. 3 b,c). The participants’ task was to rate how much they thought each trait refers to their own personality. We found that the body-sex-change illusion was efficiently induced in Experiment III as well (Fig. 3 d; Table S6 ; main effect of synchrony; illusion scores: F 1,44 = 35.88; P < 0.005; two-sided; N = 44). Ratings of stereotype-congruent traits were generally higher than ratings of stereotype-incongruent traits (Fig. 3 e; Tables S6 and S7 ). Crucially, however, this stereotypical tendency was significantly reduced in the syncO condition by the illusory ownership of the opposite-sex body (Fig. 3 f; Tables S6 and S7 ; synchrony × congruence × ownership: F 1,759 = 5.6; P = 0.018; congruence × ownership in syncO: F 1,374 = 13.46; P < 0.005; two-sided; N = 44). The participants who experienced a strong body-sex-change illusion (N = 20; median-split; see “ Materials and methods ”) rated stereotype-congruent and stereotype-incongruent traits during syncO similarly high (Fig. 3 g; Table S7 ). These findings show that the perception of one’s own masculine or feminine physical characteristics flexibly updates gender-stereotypical beliefs about one’s own personality.

Illusory ownership of the opposite-sex body was associated with less gender-stereotypical beliefs about one’s own personality traits (Experiment III). ( a ) Frames from the videos used in this experiment (N = 44; 22 females). ( b ) The experiment consisted of two conditions (syncO and asyncO); thus, in the head-mounted display, the female participants always observed a male body and the male participants a female body that was stroked either synchronously or asynchronously with regard to touches delivered to the participants. The condition order was counterbalanced across the participants, and the whole experiment took ~ 45 min. ( c ) After each condition, the participants rated how well each personality characteristic describes the self (1—“not at all”; 7—“very much”). Each BSRI sublist contained five traits stereotypically related to males (gray) and five traits stereotypically related to females (black). ( d ) The illusion ratings were significantly higher in the syncO condition than in the asyncO condition, which demonstrates that the body-sex-change illusion was efficiently induced. ( e ) Stereotype-congruent personality traits were generally rated higher than stereotype-incongruent traits. ( f ) Strong illusory ownership of the opposite-sex body was associated with less gender-stereotypical beliefs about own personality traits, specifically in the syncO condition. For clarity of display, individual data points are not shown (n = 434). ( g ) The participants who experienced a strong body-sex-change illusion (above-median I1 ownership ratings: syncO–asyncO; N = 20) rated stereotype-congruent and stereotype-incongruent traits similarly high, specifically in the syncO condition. Bar plots show means ± SE.
Finally, to assess the overall robustness of the relationship between own body perception and gender identity, we performed a post hoc meta-analysis of the data from all three experiments combined. We found that strong illusory ownership of the opposite-sex body in syncO was related to increased updating of the sense of own gender (Fig. S1 ; ρ 138 = 0.24; P < 0.005; Spearman correlation; two-tailed). Control analyses showed that the male and female participants experienced the body-sex-change illusion equally strongly and that there was no consistent significant relationship between the illusion strength and the participants’ age or baseline masculinity/femininity ratings (Fig. S2 ; for analogous evidence regarding syncS, see Fig. S3 ). Moreover, the degree of gender identity updating did not significantly differ between males and females and was not significantly related to the participants’ age or baseline masculinity/femininity ratings (Fig. S4 ). These results are in line with the notion that the full-body illusion is a robust perceptual phenomenon that generally is not affected by high-level cognitive or emotional processes 25 , 30 , which validates the current illusion-based approach to dynamically changing the perceptual basis of the bodily self in a mixed group of male and female subjects.
The present study used the body-sex-change illusion to experimentally investigate the link between own body perception and gender identity. We found that even a brief transformation of one’s own perceived bodily sex dynamically updated the subjective, implicit, and personality-related aspects of the sense of own gender and made these aspects more balanced across male and female categories. This main finding was consistent across three separate experiments conducted on a large group of control volunteers, with the use of subjective and objective behavioral measures. The fluidity of gender identity that we report here extends previous knowledge by demonstrating that the link between own body perception and the sense of own gender is dynamic, robust, and direct. It is dynamic because the effects that we detected occurred after several minutes of the body-sex-change illusion, it is robust because these effects were present at explicit and implicit levels, and it is direct because the changes in gender identity precisely followed our experimental manipulation of perceived own body sex.
By highlighting the role of own body perception in the shaping of the sense of own gender, this study adds a new perspective to existing theories of gender identity development. Specifically, it has been previously proposed that during their first year of life, infants construct presymbolic, perceptual, and unconscious representations of gender, based on patterns of maternal and paternal interactive styles; their touch, activity levels, timbre of voice, affective reactions, etc. 4 , 5 . Around the same age, babies can also detect synchronous visuotactile and synchronous visuomotor information related to their body 51 , 52 , 53 , 54 , which suggests that they have already developed a basic multisensory representation of their own body that continues to mature throughout childhood 55 . Thus, it is possible that during direct interactions with their caregivers, infants experience various degrees of sensory alignment between their own body representation and the perceptual representations of gender; this alignment might be a foundation for what older children and adolescents refine into a conscious sense of own gender 4 , 5 . The present findings fit well with the above idea and offer important new insights by showing that the moment-to-moment perception of one’s own body continues to affect gender identity even in adult participants.
The fluidity of gender identity that we demonstrate here does not deny that most people experience a stable sense of own gender. Instead, our findings indicate that a change is possible if a sufficient modification of own body representation occurs. Thus, the present study is in line with the general notion that gender identity is a “softly assembled, self-organizing system” that involves dynamic coupling between relevant biological, psychological, and sociocultural factors, such as a person’s hormonal and anatomical status, thoughts and feelings about his or her own gender, or perceived societal norms; when all these factors cohere tightly, gender identity remains stable, but when coherence is poor, gender identity is updated accordingly 4 , 5 , 8 . What current results add to this perspective is experimental support that the perception of own secondary sex characteristics is an integral part of the gender identity construction process that can considerably perturb the sense of own gender in nontransgender adults.
A thorough reader might ask how, if the perception of one’s own body is so critical for gender identity, these two aspects can remain in conflict for a prolonged period of time in transgender individuals. First, our results should not be treated as evidence that perceived bodily sex is the only factor that shapes the sense of own gender; this sense is a complex phenomenon that is constructed from multiple factors (see “ Introduction ”). Second, some characteristics of gender dysphoria, such as avoiding looking in the mirror or hiding one’s body under loose-fitting clothes 11 , 12 , suggest that these individuals might actively suppress the link between their own body perception and their subjective sense of gender. Our results contribute to the discussion about the mechanisms of gender identity by suggesting that there is a continuous bottom-up influence from the perceptual body representation on the cognitive, conceptual, and possibly affective representations of gender identity in terms of the body’s secondary sexual characteristics. Future studies should address the important question of how transgender people, with and without gender dysphoria, update their sense of own gender during the body-sex-change illusion and whether the illusion could partly alleviate distress by reducing the incongruence between the body and subjective gender.
Another key finding of the present study is that the body-sex-change illusion reduced gender-stereotypical beliefs about own personality. This result supports the claim that gender identification (e.g., “I’m a male”), gender stereotypes (e.g., “Males are competitive”), and gender-stereotypical beliefs about one’s own personality (e.g., “I’m competitive”) are connected with each other 1 , 3 , 6 , so that a change in one aspect (gender identification), due to the body-sex-change illusion, affects the other aspects (stereotypical self-beliefs). It is worth mentioning that existing programs against gender discrimination, such as media campaigns or educational workshops, mainly target explicit manifestations of gender stereotypes 56 . However, people are often unaware that their way of thinking is biased, and thus, they cannot deliberately change it. Body-oriented techniques, similar to the one used here, could possibly overcome this limitation and target more covert aspects of gender discrimination. Future research is needed to validate this approach.
Previous studies have shown that different versions of the full-body ownership illusion have various cognitive, emotional, and behavioral consequences. For example, attitudes toward other people change after illusory ownership of their bodies 29 , emotional feelings of social fear 42 and body dissatisfaction 32 , 33 can be modulated by the full-body ownership illusion, and the encoding of episodic memories depends on the embodied first-person perspective 57 . Even beliefs about own personality characteristics 58 , the recognition of one’s own face 59 , 60 , 61 , the style of one’s own behavior 62 , and implicit associations with the past-self 45 are flexibly adjusted based on the ongoing perception of one’s own body. With regard to gender, it has been shown that it is possible to induce the body-sex-change illusion 24 , 43 and that female participants who looked at male avatars from a first-person perspective improved their working memory performance during a stereotype-threatening situation 63 ; however, the latter finding needs to be interpreted with caution, as there was no conclusive evidence that the participants felt ownership of the avatar’s body. Our study extends the above literature in three ways: first, by showing that even the supposedly most stable aspects of the psychological sense of self, that is, gender identity, are dynamically updated based on the ongoing perception of one’s own body; second, by demonstrating that this updating affects both implicit and explicit beliefs about the self; and third, by clarifying that the illusory ownership of another person’s body not only modifies attitudes toward that person or toward a social group that he or she is a member of but also modifies beliefs about the self.
With regard to the cognitive mechanisms behind the body-related flexibility of self-concept, there are several possible explanations. Embodied cognition theories propose that all concepts are grounded in sensorimotor and situated representations 64 ; thus, a change in own body representation, for example, during a full-body ownership illusion, affects conceptual knowledge about the self. In turn, predictive processing theories suggest that if the low-level perceptual representation of one’s own body creates a conflict further up in the processing hierarchy, then this conflict is resolved by updating higher-order beliefs about oneself 28 , 65 . Other authors proposed that illusory ownership of someone else’s body (1) involves making inferences about own attitudes, e.g., “I am polite, because the person whose body I have is polite” 62 ; (2) that the illusion allows new associations to be formed within the “self-image network” 66 ; (3) that “owning” another person’s body makes knowledge about that person, or about a social group that this person belongs to, more accessible (i.e., primed) in the conceptual knowledge system 67 ; or (4) that body experiences of this kind increase the perceived physical similarity between the self and the other, which consequently increases the perceived conceptual similarity between the two 29 . What the present study adds to this complex discussion is the demonstration that gender identity updating is not a result of deliberate inference, as the effect occurred for implicit associations measured by the IAT; and this updating could not simply be explained by conceptual priming, because the semantic category of the opposite gender was likely “activated” even by looking at the opposite sex body during asyncO. Moreover, our results suggest that creating new associations within the self-image network is not the only mechanism involved in the updating of self-concept because, at the implicit level, the body-sex-change illusion mainly weakened associations between the self and the preferred gender category (i.e., lengthening reaction times in the congruent IAT block; Fig. 2 f; Table S5 ). Thus, the perceived bodily-sex-change possibly increased a cognitive conflict within the existing beliefs about oneself at the implicit level, which in turn was compensated by revising self-beliefs with new information at the explicit level (i.e., increasing ratings of stereotype-incongruent traits; Fig. 3 f; Table S7 ). Future studies should determine whether the body-related flexibility of self-concept involves different cognitive mechanisms depending on the degree of conscious awareness.
We speculate that at the neural level, the fundamental interplay between the perception of one’s own body and gender identity is implemented by functional interactions between the multisensory frontoparietal areas that represent the bodily self 30 , 31 , 37 , on the one hand, and the medial prefrontal regions that are involved in the self-concept representation 68 , 69 , affective body representations in the insula and anterior cingulate cortex 33 , and higher-order visual representation of the body in the lateral occipital cortex 70 , 71 , on the other. Multisensory representations in the posterior parietal cortex may be particularly important in this respect, as this region is sensitive to the perceived size and shape of one’s own body 33 , 72 , including waist size 72 , which is likely to be important for the identification of the body’s sex based on secondary sex characteristics. Notably, the pattern of resting-state connectivity in the posterior parietal cortex is different in transgender individuals compared to age-matched controls 21 , and a recent study reported that individuals with gender dysphoria display greater cortical thickness of the anterior cingulate cortex and lateral occipital cortex than controls 23 . Interestingly, the lateral occipital cortex, which includes the extrastriate body area—a higher-order visual area that is involved in the processing of images of human body parts 73 —shows increased activation during body ownership illusions 33 , 38 , 70 , 71 . Future neuroimaging studies could use the present body-sex-change illusion to perturb the sense of gender identity experimentally and investigate how the patterns of activity and functional connectivity within the above fronto-parieto-occipital networks change accordingly.
It is noteworthy that our findings are mainly related to balancing the identification with both genders rather than to a “full switch” to the opposite gender. This could be because the perception of one’s own body is not potent enough to completely override the existing sense of own gender or because the body-sex-change illusion in the present study was not induced for long enough. Future studies are needed to reveal the extent to which gender identity could change as a result of modified body representation and the persistence of such changes over time. Another methodological aspect that is noteworthy is that the body-induced fluidity of gender identity showed relatively large interindividual differences. This variability was related mainly to how vividly the participants experienced the body-sex-change illusion, which of course makes sense because if there was no change in the representation of own body, then there was no reason to update one’s gender identity. Individual differences in the strength of body ownership illusions are most likely related to how brains integrate visual, tactile, and proprioceptive signals 30 , 74 and depend on the relative weights assigned to different sensory channels, as well as prior knowledge that varies across subjects 34 , 75 . For example, if more weight is given to vision than to proprioception, the illusion should be stronger, and vice versa. Based on our data, we can conclude that variability in the illusion strength was not significantly related to the participants’ sex, age, or baseline feelings of masculinity/femininity (Figs. S2 and S3 ). Finally, it is worth mentioning that our within-subject experimental design allowed us to demonstrate a particularly strong case of gender identity flexibility that occurred for the same participants across different body perception contexts.
In sum, the present study shows that there exists a dynamic and automatic link between the perception of own body and different aspects of the sense of own gender. This main finding has important bearings on neurocognitive models of gender identity, as well as on clinical psychology and psychiatry. Moreover, the body-sex-change illusion that we report here allows for a manipulation of gender identification in nontransgender participants, which offers an unprecedented opportunity to investigate the sense of own gender in a controlled experimental setting. Importantly, people with gender dysphoria who consider surgical and hormonal procedures to adjust their physical appearance to match their gender identity could perhaps benefit from future iterations of the body-sex-change illusion, which combined with virtual reality and 3D body scanners might alleviate distress and allow these individuals to somewhat experience their own “new body” before undergoing more permanent procedures.
Materials and methods
All participants provided written informed consent before the start of each experiment. The Regional Ethics Review Board of Stockholm approved the studies. All methods were performed in accordance with the approved guidelines. The inclusion criteria were as follows: (1) age between 18 and 65 years old; (2) no history of severe psychiatric illness or neurological disorder; (3) normal or corrected-to-normal vision and hearing; (4) not wearing glasses during the experiment; and (5) understanding English (see below). These criteria were assessed during an initial interview. Sample sizes were based on similar previous studies (see “ Introduction ”) and our counterbalancing schemes. Data collection was finalized when the planned number of participants was reached. At the end of each experiment, the participants were debriefed and received compensation. All measures that were used are reported in the manuscript. Because the participants were of different nationalities, all experiments were conducted in English; the participants followed instructions without problems. The stroking procedure in Experiment I was performed by P.T., and in Experiments II and III, it was performed by J.F.
Experiment I
Participants.
Thirty-three naïve adults participated (age: 25 ± 4; 4 left-handed; 15 females). Data from one participant were excluded due to a procedural error (same condition repeated twice).
The participants first rated how masculine or feminine they felt before experiencing any body perception manipulation (baseline; Fig. 1 d). The main experiment consisted of four conditions: “synchronous opposite sex” (syncO), “synchronous same sex,” (syncS), “asynchronous opposite sex,” (asyncO), and “asynchronous same sex” (asyncS). Each condition lasted 3.5 min. During each condition, the participants lay on a bed with their heads tilted forward (~ 45°) and wore a head-mounted display (HMD; Oculus Rift Development Kit 2, Oculus VR, Menlo Park, CA, USA) so that they could not see their actual body. In the HMD, the participants watched prerecorded 3D videos of a stranger’s body, male or female, that was shown from a first-person perspective. The stranger’s body was continuously stroked on the thighs and abdomen, and the experimenter delivered synchronous (syncO, syncS) or asynchronous (1 s delayed; asyncO, asyncS) touches on the corresponding parts of the participant’s body (Fig. 1 a). During each condition, there were three “knife threats” that occurred 1, 2, and 3 min after the beginning of each video (Fig. 1 c,e). After each condition, the participants took off the HMD, filled out the illusion questionnaire (Fig. 1 b) and rated how masculine or feminine they felt during the preceding session (Fig. 1 d). The order of conditions was counterbalanced across the participants, and the whole experiment lasted ~ 30 min (Fig. 1 e).
Prerecorded videos
During filming, a male and a female lay still on a bed. The experimenter used a 90-cm-long stick with a white plastic ball (diameter 10 cm) attached to its end to deliver strokes to each model’s abdomen, left thigh, or right thigh. The duration of each stroke was 1 s, and each stroke covered ~ 20 cm of the model’s body. The time between the end of one touch and the onset of the next touch ranged between 3 and 5 s. The frequency of strokes was 12 times per minute. The order of strokes was pseudorandom (i.e., no more than two successive strokes of the same body part). Altogether, 36 strokes (12 to each body part) were delivered during each video. The videos were recorded with two identical cameras (GoPro HERO4 Silver, GoPro, Inc., San Mateo, CA, USA) placed parallel to each other (8 cm apart) just above the models’ heads. The recordings from both cameras were combined into a single frame using Final Cut Pro software (version 7, Apple Inc., Cupertino, CA, USA). Two versions of high-quality 3D videos were created: one for the male and one for the female body. Audio cues were then added to each video. These cues were either congruent with touches applied in the videos (same body parts, same onset, same duration) or delayed by 1 s. The experimenter listened to these cues during the experiment and applied touches accordingly. All other aspects were identical in the synchronous and asynchronous videos.
Knife threats
For each of the two videos, we recorded knife-threat events. During these events, a hand holding a knife entered the field of view from above and performed a stabbing movement toward the model’s body (Fig. 1 c). The knife stopped just before hitting the body, changed direction (− 180°), and exited the field of view in the same way that it had entered. The whole event lasted 2 s. Great care was taken to ensure that the knife threats in the male and female versions of the videos looked as similar as possible. Knife threats in the synchronous and asynchronous versions of the same video (male or female) were identical. Subsequent knife threats within a given condition were also identical. After each knife threat, there was a 10 s pause when no strokes were delivered. In line with good ethical practice, before the experiment, we informed the participants about the knife threats in the videos to prevent overly high emotional stress.
Visuotactile stimulation during the experiment
The experimenter listened to audio cues from the videos (see earlier) and accordingly applied touches to the participant’s body. These cues were played via headphones, so the participants could not hear them. The number, order, type, length, velocity, and frequency of strokes during the experiment precisely followed the prerecorded videos (see earlier). To deliver touches, the experimenter used the same white ball attached to a stick that had been used in the video recordings.
Illusion questionnaires
Subjective experience of the full-body ownership illusion was quantified with a questionnaire that began with an open-ended sentence (“During the last session, there were times when…”). This sentence was followed by three illusion statements that quantified the explicit feeling of body ownership (I1; Fig. 1 b) and the sensation of touch directly on the stranger’s body (I2 and I3; Fig. 1 b). Ownership and referral of touch are considered to be the two core elements of the multisensory full-body illusion 25 , 26 . Apart from the illusion statements, the questionnaire included four control statements (C1–C4; Fig. 1 b) that were added to control for potential task compliance or suggestibility effects. The questionnaire administered to the participants had items listed in the following pseudorandom order: C1, I1, C2, I2, C3, C4, I3. The participants marked their responses on a scale from − 3 (“strongly disagree”) to + 3 (“strongly agree”).
Skin conductance responses
The skin conductance response reflects increased sweating attributable to the activation of the autonomic nervous system 76 . When one’s own body is physically threatened, the threat triggers emotional feelings of fear and anticipation of pain that are associated with autonomic arousal. This arousal can be registered as a brief increase in skin conductance a few seconds after the threat event. Increased threat-evoked skin conductance responses, compared to a well-matched control condition, are often used as an index of body ownership in body illusion paradigms 24 , 30 , 38 . In the current experiment, data were recorded continuously with the Biopac system MP150 (Biopac Systems Inc., Goleta, CA, USA) and AcqKnowledge software (version 3.9). The following parameters were used: sampling rate = 100 Hz, low-pass filter = 1 Hz, high-pass filter = DC, gain = 5 μS/V, and CAL2 scale value = 5. Two Ag–AgCl electrodes (model TSD203, Biopac Systems Inc., Goleta, CA, USA) were placed on the volar surfaces of the distal phalanges of the participants’ left index and middle fingers. Isotonic paste (GEL101; Biopac Systems Inc., Goleta, CA, USA) was used to improve the skin contact and recording quality. At the beginning of the experiment, we asked the participants to take the deepest breath possible and hold it for a couple of seconds. In this way, we tested our equipment and established a near maximum response for each participant. The timing of threat events was marked in the recording file by the experimenter by pressing a laptop key immediately after the threat occurred.
Masculinity/femininity ratings
The participants marked their responses on a visual analog scale (Fig. 1 d). Scale assignment was different for the male and female participants (Fig. 1 d). Baseline ratings were generally greater than zero, as expected for a nontransgender group, but showed some degree of variability (mean = 2.22; SD = 0.97; min = − 1; max = 4).
Experiment II
Sixty-four naïve adults participated (age: 27 ± 5; all right-handed; 32 females).
The participants first completed a practice IAT (20 trials). The main study consisted of the same four conditions as those in Experiment I, that is, syncO, asyncO, syncS, and asyncS (Figs. 1 a, 2 a). After the initial phase of just watching the videos and feeling touches (30 s), the participants started the first IAT block (Fig. 2 b,c). IAT stimuli were presented via headphones (Spectrum, Maxell Europe Ltd., Berkshire, UK). The participants used a wireless computer mouse held in the right hand to indicate responses. During each condition, the participants observed two “knife threats” (see further), one in the middle and one at the end of each condition (Fig. 2 c). After each condition, the participants completed the same illusion questionnaire as in Experiment I (Fig. 1 b). The order of the conditions was counterbalanced. The whole study lasted ~ 1 h (Fig. 2 c).
The videos were prepared analogously to those in Experiment I, but a different male and female were filmed to assure that our results were not driven by a certain body type or clothing style of the models (Fig. 2 a). Strokes were applied to three body parts: abdomen, left thigh, and right thigh. The abdomen strokes were either single or double (1 s apart). The duration of each stroke was 1 s, and each stroke covered ~ 20 cm of the model’s body. The time between the offset of one touch and the onset of the next touch ranged from 3 to 6 s. The frequency of strokes was 12 times per minute. The touches were delivered in a pseudorandom sequence, with no more than three successive strokes on the same body part. Altogether, 88 touches (22 on each body part) were applied in each video. The videos were recorded with Infinity cameras (1080p Full HD, CamOneTec, Delbrück, Germany) and prepared in the same way as in Experiment I. In the synchronous videos, audio cues were matched with the touches applied in the videos, whereas in the asynchronous videos, the cues were delayed by 1 s and pertained to different body parts. Altogether, we created four versions (syncO, syncS, asyncO, asyncS) of the high-quality 3D videos, each lasting 7 min 5 s.
We used the auditory version of the brief gender identity IAT 47 , 77 . The instruction for one block was as follows: “The test will start in a few seconds. Please listen to the instructions. Try to go as fast as possible while making as few mistakes as possible. If the word belongs to the categories female or self , press left. If the word does not belong to these categories, press right. The test will begin now.” The instruction for the other block differed only with regard to category assignment: “If the word belongs to the categories male or self , press left. If the word does not belong to these categories, press right.” The key assignment remained the same for a given participant across all conditions but was counterbalanced between the participants. The order of IAT blocks was counterbalanced in the same way. The stimulus set consisted of twenty words (Fig. 2 b) that were read by an English native speaker. The volume of each word sound was adjusted using Audacity software (the “normalize” effect; version 2.1.2, https://www.audacityteam.org ). Each word was edited to have a duration similar to that of other words. Please note that the physical differences between stimuli cannot explain the main IAT results because the congruent and incongruent blocks used exactly the same stimuli. The participants had a maximum of 3 s to provide a response (time from the stimulus onset to the end of each trial). If no key was pressed within this time or the wrong key was pressed, the participants heard a “wrong” feedback beep. Each IAT block consisted of 60 trials (three repetitions of all 20 words) presented in random order. The procedure was self-paced, that is, the next trial started as soon as the participant responded in the previous trial (maximum duration of one block ~ 3 min). Presentation software (Neurobehavioral Systems Inc., Albany, CA, USA) was used to present the stimuli and record responses.
These events were recorded in the same way as in Experiment I (i.e., stabbing movement toward the abdomen; 2 s duration). We used triggers from the Presentation software to automatically flag the onset of the knife threats in the skin conductance recording files.
Experiment III
Forty-five naïve adults participated (age: 26 ± 5; all right-handed; 22 females). One participant was excluded because he did not complete one of the questionnaires.
The study lasted ~ 35 min and comprised two conditions: syncO and asyncO (Fig. 3 a,b). Each condition lasted 14 min 10 s. After each condition, the participants filled out the illusion questionnaire (the same as in Experiments I and II) and the Bem Sex-Role Inventory; BSRI 49 , 50 (see further). The order of conditions was counterbalanced across participants (Fig. 3 b).
The videos were prepared analogously to those in Experiments I and II. Four types of strokes (single abdomen, double abdomen, left thigh, and right thigh) were applied. The duration of each stroke was 1 s, and each stroke covered ~ 20 cm of the model’s body. The time between the offset of one touch and the onset of the next touch ranged from 2 to 10 s. The frequency of strokes was 12 times per minute. Different touches were delivered in a pseudorandom sequence, with no more than three successive strokes on the same body part. Altogether, 160 touches (40 on each body part) were applied in each video. Infinity cameras (1080p Full HD, CamOneTec, Delbrück, Germany) were used to record the videos. Audio cues were matched to touches in the synchronous videos and delayed by 1 s in the asynchronous videos.
After each condition, the participants filled out a version of the BSRI 49 , 50 . The questionnaire contained 5 stereotypically masculine and 5 stereotypically feminine personality traits (Fig. 3 c). Using a 7-point Likert scale (1—“not at all”; 7—“very much”), the participants rated how well each trait described them. Ten traits were rated after the first condition and the other ten after the second condition. The order of BSRI versions was counterbalanced.
Analysis of illusion questionnaires
For each participant and condition, we calculated “illusion scores” as the differences between the average illusion (I1–I3) and the control (C1–C4) ratings. To confirm successful induction of the illusion, we compared these illusion scores between the synchronous and asynchronous conditions. The results for individual questionnaire items are shown in Figs. S5 and S6 . The effect of “ownership” used in the correlation analyses (Figs. 1 h, 2 f, 3 f) was the difference between I1 ownership ratings in syncO–asyncO (one value per participant). The participants who experienced a strong body-sex-change illusion were selected using the median-split method applied to ownership scores (see above). The median-split analyses (Figs. 1 i, 2 g, and 3 g) were performed mainly for display purposes and to complement the main analyses using continuous scores.
Analysis of skin conductance responses
Each response was measured as the difference between the maximum and minimum values during the 0–6 s period after each knife threat. Responses below 0.02 μS were treated as zeroes but were included in the analysis of the magnitude of skin conductance responses 76 . Statistical outliers were identified with the ± 1.5 interquartile criterion and removed from the dataset (16% and 6% of the values in Experiments I and II, respectively). Keeping the outliers did not change the main findings (main effect of synchrony in Experiment I: F 1,31 = 5.76; P = 0.023; N = 32; Experiment II: F 1,63 = 6.43; P = 0.014; N = 64; two-sided). We applied a square-root transformation to the skin conductance data 76 . Statistical models included the effect of “repetition”, which indicated how many knife threats had already occurred in the study (max. 12 in Experiment I and max. 8 in Experiment II). The magnitude of the skin conductance responses decreased exponentially with subsequent knife threats (Fig. S7 ). To “linearize” this relationship, we transformed the repetition number (1/repetition), which substantially improved the fit of the linear models to the data (Fig. S7 ; Experiment I: χ 2 = 4.36; P < 0.005; Experiment II: χ 2 = 37.26; P < 0.005; two-sided; N = 32 and N = 64, respectively). The effect of repetition (habituation) was highly significant (Tables S2 and S4), which was expected 76 . For the control analyses presented in Figs. S2 and S3 , we (1) calculated residuals from the following model: SCR ~ repetition; (2) averaged them for a given participant and condition; and (3) calculated the difference: syncO–asyncO (Fig. S2 ) or syncS–asyncS (Fig. S3 ). Using the residuals accounted for the habituation effect (see earlier).
Analysis of masculinity/femininity ratings, IAT, and BSRI
Raw masculinity/femininity ratings were analyzed (n = 160; one value per condition). IAT data included only correct trials, in which reaction times were longer than 200 ms and shorter than 1,500 ms (95.5% of all trials; n = 29,147). Reaction times were log-transformed. The BSRI analysis was performed on raw ratings (n = 862; 18 ratings missing). Analyses of IAT and BSRI included random intercepts of “1|Item”, which accounted for possible variability between different words (Tables S4 – S7 ).
Meta-analysis
For each participant in each experiment, we calculated the degree of gender identity updating. In Experiment I, this updating score was calculated as the following difference between the masculinity/femininity ratings: [(syncS + asyncS + asyncO)/3]–syncO. In Experiment II, this score was calculated as the difference between the average reaction times in each IAT block: [(syncS i-c + asyncS i-c + asyncO i-c )/3] – syncO i-c , where “i” and “c” denote “incongruent” and “congruent”, respectively. Finally, in Experiment III, the updating was calculated as the difference between average personality ratings from each condition: asyncO c-i –syncO c-i , where “c” and “i” correspond to stereotype-congruent and stereotype-incongruent traits, respectively. Because these scores were on different scales, we standardized them (i.e., from each participant’s score, we subtracted the group mean from the respective experiment and divided the result by the group standard deviation).
General statistical information
All statistical analyses were performed in RStudio and R software (version 3.3.3, The R Foundation for Statistical Computing, https://www.r-project.org ). Linear mixed models were estimated using the “lme4” package. Information regarding model selection is provided in Table S1 . All results are reported in Tables S2 – S7 . The distribution of residuals from each main model are shown in Fig. S8 . P -values for the F-tests were based on Satterthwaite’s approximation to degrees of freedom, as implemented by the “lmerTest” package (Tables S2 , S4 , and S6 ). P -values for effect size coefficients (Tables S3 , S5 , and S6 ) and their 95% confidence intervals were obtained with the bootstrapping method by comparing a given coefficient value to its null distribution derived from resampling the original dataset (“boot” package; 1,000 simulations).
Data availability
We do not have ethics approval to make the raw data from individual subjects publicly available.
Egan, S. K. & Perry, D. G. Gender identity: a multidimensional analysis with implications for psychosocial adjustment. Dev. Psychol. 37 , 451–463 (2001).
PubMed CAS Google Scholar
Tate, C. C., Youssef, C. P. & Bettergarcia, J. N. Integrating the study of transgender spectrum and cisgender experiences of self-categorization from a personality perspective. Rev. Gen. Psychol. 18 , 302–312 (2014).
Google Scholar
Tobin, D. D. et al. The intrapsychics of gender: a model of self-socialization. Psychol. Rev. 117 , 601–622 (2010).
PubMed Google Scholar
Fausto-Sterling, A. The dynamic development of gender variability. J. Homosex. 59 , 398–421 (2012).
Fausto-Sterling, A. Gender/sex, sexual orientation, and identity are in the body: how did they get there?. J. Sex Res. 56 , 529–555 (2019).
Money, J. The concept of gender identity disorder in childhood and adolescence after 39 years. J. Sex Marital Ther. 20 , 163–177 (1994).
Frable, D. E. S. Gender, racial, ethnic, sexual, and class identities. Annu. Rev. Psychol. 48 , 139–162 (1997).
Martin, C. L. & Ruble, D. N. Patterns of gender development. Annu. Rev. Psychol. 61 , 353–381 (2009).
American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed.) . (2013).
World Health Organization. International statistical classification of diseases and related health problems (11th ed.) . (2019).
Becker, I. et al. Body image in young gender dysphoric adults: a European multi-center study. Arch. Sex. Behav. 45 , 559–574 (2016).
van de Grift, T. C. et al. Body satisfaction and physical appearance in gender dysphoria. Arch. Sex. Behav. 45 , 575–585 (2016).
Piot-Ziegler, C., Sassi, M.-L., Raffoul, W. & Delaloye, J.-F. Mastectomy, body deconstruction, and impact on identity: a qualitative study. Br. J. Health Psychol. 15 , 479–510 (2010).
Wassersug, R. J., Mckenna, E. & Lieberman, T. Eunuch as a gender identity after castration. J. Gend. Stud. 21 , 253–270 (2012).
Feusner, J. D. et al. Female-to-male transsexual individuals demonstrate different own body identification. Arch. Sex. Behav. 45 , 525–536 (2016).
Majid, D. S. A. et al. Neural systems for own-body processing align with gender identity rather than birth-assigned sex. Cereb. Cortex 30 , 2897–2909 (2020).
Manzouri, A., Kosidou, K. & Savic, I. Anatomical and functional findings in female-to-male transsexuals: testing a new hypothesis. Cereb. Cortex 27 , 998–1010 (2017).
Burke, S. M., Manzouri, A. H. & Savic, I. Structural connections in the brain in relation to gender identity and sexual orientation. Sci. Rep. 7 , 17954 (2017).
ADS PubMed PubMed Central Google Scholar
Burke, S. M. et al. Testosterone effects on the brain in transgender men. Cereb. Cortex 28 , 1582–1596 (2018).
Kilpatrick, L. A., Holmberg, M., Manzouri, A. & Savic, I. Cross sex hormone treatment is linked with a reversal of cerebral patterns associated with gender dysphoria to the baseline of cisgender controls. Eur. J. Neurosci. 50 , 3269–3281 (2019).
Lin, C.-S. et al. Neural network of body representation differs between transsexuals and cissexuals. PLoS ONE 9 , e85914 (2014).
Case, L. K., Brang, D., Landazuri, R., Viswanathan, P. & Ramachandran, V. S. Altered white matter and sensory response to bodily sensation in female-to-male transgender individuals. Arch. Sex. Behav. 46 , 1223–1237 (2017).
Manzouri, A. & Savic, I. Possible neurobiological underpinnings of homosexuality and gender dysphoria. Cereb. Cortex 29 , 2084–2101 (2019).
Petkova, V. I. & Ehrsson, H. H. If I were you: perceptual illusion of body swapping. PLoS ONE 3 , e3832 (2008).
Ehrsson, H. H. The concept of body ownership and its relation to multisensory integration. in The new handbook of multisensory processes (ed. Stein, B. E.) 775–792 (MIT Press, 2012).
Kilteni, K., Maselli, A., Kording, K. P. & Slater, M. Over my fake body: body ownership illusions for studying the multisensory basis of own-body perception. Front. Hum. Neurosci. 9 , 141 (2015).
PubMed PubMed Central Google Scholar
Blanke, O. Multisensory brain mechanisms of bodily self-consciousness. Nat. Rev. Neurosci. 13 , 556–571 (2012).
Tsakiris, M. The multisensory basis of the self: from body to identity to others. Q. J. Exp. Psychol. 70 , 597–609 (2017).
Maister, L., Slater, M., Sanchez-Vives, M. V. & Tsakiris, M. Changing bodies changes minds: owning another body affects social cognition. Trends Cogn. Sci. 19 , 6–12 (2014).
Ehrsson, H. H. Multisensory processes in body ownership. In Multisensory Perception: From Laboratory to Clinic (eds. Sathian, K. & Ramachandran, V.) 179–200 (Academic Press, 2020).
Petkova, V. I. et al. From part- to whole-body ownership in the multisensory brain. Curr. Biol. 21 , 1118–1122 (2011).
Preston, C. & Ehrsson, H. H. Illusory changes in body size modulate body satisfaction in a way that is related to non-clinical eating disorder psychopathology. PLoS ONE 9 , e85773 (2014).
Preston, C. & Ehrsson, H. H. Illusory obesity triggers body dissatisfaction responses in the insula and anterior cingulate cortex. Cereb. Cortex 26 , 4450–4460 (2016).
Ehrsson, H. H. & Chancel, M. Premotor cortex implements causal inference in multisensory own-body perception. Proc. Natl. Acad. Sci. USA 116 , 19771–19773 (2019).
Botvinick, M. & Cohen, J. Rubber hands ‘feel’ touch that eyes see. Nature 391 , 756 (1998).
ADS PubMed CAS Google Scholar
Guterstam, A., Larsson, D. E. O., Zeberg, H. & Ehrsson, H. H. Multisensory correlations—not tactile expectations—determine the sense of body ownership. PLoS ONE 14 , e0213265 (2019).
PubMed PubMed Central CAS Google Scholar
Ehrsson, H. H., Spence, C. & Passingham, R. E. That’s my hand! Activity in premotor cortex reflects feeling of ownership of a limb. Science 305 , 875–877 (2004).
Guterstam, A., Björnsdotter, M., Gentile, G. & Ehrsson, H. Posterior cingulate cortex integrates the senses of self-location and body ownership. Curr. Biol. 25 , 1416–1425 (2015).
van der Hoort, B., Guterstam, A. & Ehrsson, H. H. Being Barbie: the size of one’s own body determines the perceived size of the world. PLoS ONE 6 , e20195 (2011).
Peck, T. C., Seinfeld, S., Aglioti, S. M. & Slater, M. Putting yourself in the skin of a black avatar reduces implicit racial bias. Conscious. Cogn. 22 , 779–787 (2013).
Maister, L., Sebanz, N., Knoblich, G. & Tsakiris, M. Experiencing ownership over a dark-skinned body reduces implicit racial bias. Cognition 128 , 170–178 (2013).
Guterstam, A., Abdulkarim, Z. & Ehrsson, H. H. Illusory ownership of an invisible body reduces autonomic and subjective social anxiety responses. Sci. Rep. 5 , 9831 (2015).
ADS PubMed PubMed Central CAS Google Scholar
Slater, M., Spanlang, B., Sanchez-Vives, M. V. & Blanke, O. First person experience of body transfer in virtual reality. PLoS ONE 5 , e10564 (2010).
Banakou, D., H, P. D. & Slater, M. Virtual embodiment of white people in a black virtual body leads to a sustained reduction in their implicit racial bias. Front. Hum. Neurosci. 10 , 601 (2016).
Banakou, D., Groten, R. & Slater, M. Illusory ownership of a virtual child body causes overestimation of object sizes and implicit attitude changes. Proc. Natl. Acad. Sci. 110 , 12846–12851 (2013).
Egloff, B. & Schmukle, S. C. Predictive validity of an implicit association test for assessing anxiety. J. Pers. Soc. Psychol. 83 , 1441–1455 (2002).
Sriram, N. & Greenwald, A. G. The brief implicit association test. Exp. Psychol. 56 , 283–294 (2009).
Olson, K. R., Key, A. C. & Eaton, N. R. Gender cognition in transgender children. Psychol. Sci. 26 , 467–474 (2015).
Stern, B. B., Barak, B. & Gould, S. J. Sexual identity scale: a new self-assessment measure. Sex Roles 17 , 503–519 (1987).
Bem, S. L. The measurement of psychological androgyny. J. Consult. Clin. Psychol. 42 , 155–162 (1974).
Bahrick, L. E. & Watson, J. S. Detection of intermodal proprioceptive-visual contingency as a potential basis of self-perception in infancy. Dev. Psychol. 21 , 963–973 (1985).
Filippetti, M. L., Johnson, M. H., Lloyd-Fox, S., Dragovic, D. & Farroni, T. Body perception in newborns. Curr. Biol. 23 , 2413–2416 (2013).
Filippetti, M. L., Lloyd-Fox, S., Longo, M. R., Farroni, T. & Johnson, M. H. Neural mechanisms of body awareness in infants. Cereb. Cortex 25 , 3779–3787 (2015).
Bremner, A. J. Developing body representations in early life: combining somatosensation and vision to perceive the interface between the body and the world. Dev. Med. Child Neurol. 58 , 12–16 (2016).
Cowie, D., McKenna, A., Bremner, A. J. & Aspell, J. E. The development of bodily self-consciousness: changing responses to the full body illusion in childhood. Dev. Sci. e12557 (2017).
Lai, C. K. et al. Reducing implicit racial preferences: I. A comparative investigation of 17 interventions. J. Exp. Psychol. Gen. 143 , 1765–85 (2014).
Bergouignan, L., Nyberg, L. & Ehrsson, H. H. Out-of-body-induced hippocampal amnesia. Proc. Natl. Acad. Sci. 111 , 4421–4426 (2014).
Tacikowski, P., Weijs, M. L. & Ehrsson, H. H. Perception of our own body influences self-concept and self-incoherence impairs episodic memory. iScience (2020). https://doi.org/10.1016/j.isci.2020.101429 .
Tsakiris, M. Looking for myself: current multisensory input alters self-face recognition. PLoS ONE 3 , e4040 (2008).
Tajadura-Jimenez, A., Grehl, S. & Tsakiris, M. The other in me: interpersonal multisensory stimulation changes the mental representation of the self. PLoS ONE 7 , e40682 (2012).
Sforza, A., Bufalari, I., Haggard, P. & Aglioti, S. M. My face in yours: visuo-tactile facial stimulation influences sense of identity. Soc. Neurosci. 5 , 148–162 (2010).
Yee, N., Bailenson, J. N. & Ducheneaut, N. The Proteus effect implications of transformed digital self-representation on online and offline behavior. Communic. Res. 36 , 285–312 (2009).
Peck, T. C., Doan, M., Bourne, K. A. & Good, J. J. The effect of gender body-swap illusions on working memory and stereotype threat. IEEE Trans. Vis. Comput. Graph. 24 , 1604–1612 (2018).
Barsalou, L. W. Grounded cognition. Annu. Rev. Psychol. 59 , 617–645 (2008).
Apps, M. A. J. & Tsakiris, M. The free-energy self: a predictive coding account of self-recognition. Neurosci. Biobehav. Rev. 41 , 85–97 (2014).
Bedder, R. L. et al. A mechanistic account of bodily resonance and implicit bias. Cognition 184 , 1–10 (2019).
Peña, J., Hancock, J. T. & Merola, N. A. The priming effects of avatars in virtual settings. Communic. Res. 36 , 838–856 (2009).
Tacikowski, P., Berger, C. C. & Ehrsson, H. H. Dissociating the neural basis of conceptual self-awareness from perceptual awareness and unaware self-processing. Cereb. Cortex 27 , 3768–3781 (2017).
Macrae, C. N., Moran, J. M., Heatherton, T. F., Banfield, J. F. & Kelley, W. M. Medial prefrontal activity predicts memory for self. Cereb. Cortex 14 , 647–654 (2004).
Gentile, G., Guterstam, A., Brozzoli, C. & Ehrsson, H. H. Disintegration of multisensory signals from the real hand reduces default limb self-attribution: an fMRI study. J. Neurosci. 33 , 13350–13366 (2013).
Limanowski, J. & Blankenburg, F. Integration of visual and proprioceptive limb position information in human posterior parietal, premotor, and extrastriate cortex. J. Neurosci. 36 , 2582–2589 (2016).
Ehrsson, H. H., Kito, T., Sadato, N., Passingham, R. E. & Naito, E. Neural substrate of body size: illusory feeling of shrinking of the waist. PLoS Biol. 3 , e412 (2005).
Downing, P. E., Jiang, Y., Shuman, M. & Kanwisher, N. A cortical area selective for visual processing of the human body. Science 293 , 2470–2473 (2001).
Costantini, M. et al. Temporal limits on rubber hand illusion reflect individuals’ temporal resolution in multisensory perception. Cognition 157 , 39–48 (2016).
Samad, M., Chung, A. J. & Shams, L. Perception of body ownership is driven by Bayesian sensory inference. PLoS ONE 10 , e0117178 (2015).
Dawson, M., Schell, A. & Filion, D. The electrodermal system. in The handbook of psychophysiology (eds. Cacioppo, J., Tassinary, L. & Berntson, G.) 152–191 (Cambridge University Press, 2007).
Nosek, B. A., Bar-Anan, Y., Sriram, N., Axt, J. & Greenwald, A. G. Understanding and using the brief implicit association test: Recommended scoring procedures. PLoS ONE 9 , 1–31 (2014).
Download references
Acknowledgements
This study was funded by the Swedish Research Council, Torsten Söderbergs Stiftelse, Göran Gustafsons Stiftelse, StratNeuro, and the European Commission (MSCA fellowship awarded to P.T.; 750955). We want to thank all the participants and Martti Mercurio for important technical support.
Open Access funding provided by Karolinska Institute.
Author information
Authors and affiliations.
Department of Neuroscience, Karolinska Institute, Stockholm, Sweden
Pawel Tacikowski, Jens Fust & H. Henrik Ehrsson
Department of Neurosurgery, Univeristy of California Los Angeles, Los Angeles, USA
Pawel Tacikowski
Department of Clinical Neuroscience, Karolinska Institute, Stockholm, Sweden
You can also search for this author in PubMed Google Scholar
Contributions
P.T. and H.H.E. designed the study and wrote the manuscript. P.T. and J.F. collected and analyzed the data. All authors provided revisions and approved the final version of the manuscript for submission.
Corresponding author
Correspondence to Pawel Tacikowski .
Ethics declarations
Competing interests.
The authors declare no competing interests.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary movie s1, supplementary movie s2, rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Cite this article.
Tacikowski, P., Fust, J. & Ehrsson, H.H. Fluidity of gender identity induced by illusory body-sex change. Sci Rep 10 , 14385 (2020). https://doi.org/10.1038/s41598-020-71467-z
Download citation
Received : 02 September 2019
Accepted : 11 August 2020
Published : 01 September 2020
DOI : https://doi.org/10.1038/s41598-020-71467-z
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
This article is cited by
Developmental changes of bodily self-consciousness in adolescent girls.
- Cédric Goulon
- Marie-Hélène Grosbras
Scientific Reports (2024)
Synchronous motor imagery and visual feedback of finger movement elicit the moving rubber hand illusion, at least in illusion-susceptible individuals
- Christopher C. Berger
- H. Henrik Ehrsson
Experimental Brain Research (2023)
Navigating the Cultural Landscape Through Publishing Brands: A Theoretical, Gendered Perspective
- Miriam J. Johnson
Publishing Research Quarterly (2023)
Effects of a virtual gender swap on social and temporal decision-making
- Jasmine T. Ho
- Bigna Lenggenhager
Scientific Reports (2021)
Bodily ownership and agency sensations in a natural state
- Souta Hidaka
- Kyoshiro Sasaki
- Wataru Teramoto
By submitting a comment you agree to abide by our Terms and Community Guidelines . If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.

Click through the PLOS taxonomy to find articles in your field.
For more information about PLOS Subject Areas, click here .
Loading metrics
Open Access
Peer-reviewed
Research Article
Sexual orientation and gender identity and expression conversion exposure and their correlates among LGBTQI2+ persons in Québec, Canada
Roles Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Supervision, Writing – original draft
* E-mail: [email protected]
Affiliations Research Chair in Sexual Diversity and Gender Plurality, Université du Québec à Montréal, Montréal, Québec, Canada, Département de sexologie, Université du Québec à Montréal, Montréal, Québec, Canada
Roles Writing – original draft
Affiliation Research Chair in Sexual Diversity and Gender Plurality, Université du Québec à Montréal, Montréal, Québec, Canada
Roles Writing – review & editing
Affiliation Faculty of Law and Joint Centre for Bioethics, University of Toronto, Toronto, Ontario, Canada
Roles Formal analysis, Methodology
Roles Conceptualization, Funding acquisition, Writing – review & editing
Affiliation Département de travail social, Université du Québec en Outaouais, Gatineau, Québec, Canada
- Martin Blais,
- Fabio Cannas Aghedu,
- Florence Ashley,
- Mariia Samoilenko,
- Line Chamberland,
- Isabel Côté
- Published: April 6, 2022
- https://doi.org/10.1371/journal.pone.0265580
- Reader Comments
Despite greater acceptance of sexual and gender diversity and the scientific consensus that same-gender attraction, creative gender expression, and transness are not mental illnesses, LGBTQI2+ persons are still commonly told that they can or should change their sexual orientation, gender identity, or gender expression (SOGIE). The aim of this study was to describe the prevalence of SOGIE conversion efforts, including their sociodemographic correlates, among LGBTQI2+ persons.
Using community-based sampling, we assessed SOGIE conversion attempts and involvement in conversion services of 3,261 LGBTQI2+ persons aged 18 years and older in Quebec, Canada.
A quarter of respondents experienced SOGIE conversion attempts, and fewer than 5% were involved in conversion services. Over half of those who were involved in SOGIE conversion services consented to them, but the services’ goals were made clear and explicit to only 55% and 30% of those who engaged in SO and GIE conversion, respectively. The results also suggest that family plays a key role in SOGIE conversion attempts and services utilization, and that indigenous, intersex, transgender, non-binary, and asexual persons, people of colour, as well as individuals whose sexual orientation is not monosexual (i.e., bisexual, pansexual) were more likely to have been exposed to conversion attempts and involved in conversion services.
Conclusions
This study found that the prevalence of conversion efforts is substantial. Interventions to protect LGBTQI2+ people from such attempts should focus not only on legal bans, but also on supporting families who need to be counseled in accepting sexual and gender diversity. Health professionals need to be adequately trained in LGBTQI2+ affirmative approaches. Religious therapists should consult with colleagues and undergo supervision to ensure that their religious beliefs do not interfere with their practice.
Citation: Blais M, Cannas Aghedu F, Ashley F, Samoilenko M, Chamberland L, Côté I (2022) Sexual orientation and gender identity and expression conversion exposure and their correlates among LGBTQI2+ persons in Québec, Canada. PLoS ONE 17(4): e0265580. https://doi.org/10.1371/journal.pone.0265580
Editor: Stefano Federici, University of Perugia: Universita degli Studi di Perugia, ITALY
Received: September 24, 2021; Accepted: March 7, 2022; Published: April 6, 2022
Copyright: © 2022 Blais et al. This is an open access article distributed under the terms of the Creative Commons Attribution License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: Since the data contain potentially sensitive information about study participants, the Université du Québec à Montréal’ Human Research Ethics Board has only approved storage of the dataset on secure institutional servers. Any requests to access the data can be made to Université du Québec à Montréal’ Human Research Ethics Board ( [email protected] ; reference Ethics Protocol Number #2020-2218).
Funding: This research is supported by funding from the Social Sciences and Humanities Research Council of Canada. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests: The authors have declared that no competing interests exist.
Introduction
Despite greater acceptance of sexual and gender diversity and the scientific consensus that same-gender attraction, creative gender expression, and transness are not mental illnesses, lesbian, gay, bisexual, trans, queer, intersex, two-spirit (LGBTQI2+) persons are still commonly told that they can or should change their sexual orientation (SO), gender identity (GI), or gender expression (GE). A recent study revealed that two-thirds of youths aged 13–24 years in the US reported that someone had tried to convince them to change their SOGIE [ 1 ]. Such pressures stem from the belief that it is best to be heterosexual and cisgender (i.e., not transgender) and that people should be changed when they do not conform to cisheterosexist norms. The concept of SOGIE change efforts has been coined to describe any direction or advice that intentionally delays or impedes self-acceptance of one’s sexual orientation, gender identity, or gender expression [ 2 – 4 ]. The 2020 edition of the Canadian Sex Now Survey revealed that about 20% of sexual minority men (gay, bisexual, transgender, Two-Spirit and queer) have been exposed to such efforts [ 5 ]. The US Transgender Survey found that 14% of respondents reported lifetime exposure to gender identity conversion efforts [ 6 ].
Conversion therapy refers to more sustained, structured, specific interventions aiming at changing, discouraging, or repressing SOGIE [ 2 – 4 ]. It relies on various techniques, inspired by psychotherapeutic, medical, or faith-based principles (e.g., talk therapy, aversion therapy, hormonotherapy, spiritual guidance) and takes place in various contexts ranging from private or public settings to “gay conversion camps” or religious institutions. Not only are they inefficient, scientifically unsound, and unethical, but they are also known to have adverse effects on survivors [ 6 – 8 ]. It is thus unsurprising that most psychological, medical, and sexual health professional associations have opposed SO conversion efforts for decades, and most of them are now adopting similar responses to GIE conversion efforts [ 9 ]. In December 2020, a ban on SOGIE conversion therapies has been adopted in Québec. This new law targets practices intended to “induce persons to change their sexual orientation, gender identity or gender expression or to repress non-heterosexual sexual behaviour” and applies regardless of age [ 10 ]. Violations are subject to heavy fines, professional discipline, and/or victim compensation. Federally, a criminal ban has been adopted by the Senate [ 11 ]. According to this new law, anyone who advertises, materially benefits from, or causes a person to undergo SOGIE conversion therapy would be liable to imprisonment for up to five years depending on the offence.
Professional associations’ statements are insufficient, as conversion experiences continue to be reported. In the US, about 4% of youths aged 13–24 years have undergone SOGI conversion therapy [ 7 ]. In Canada, three large, non-probabilistic studies have documented SOGI conversion experiences: the Sex Now survey 2011–2012 (N = 8,388) revealed that about 3.5% of Canadian sexual minority men (i.e., gay, bisexual, transgender, Two-Spirit and queer) experienced SO conversion therapy (4.2% in Quebec; [ 4 ]), the Sex Now survey 2019–2020 (N = 9,214) found that 9.9% of participants were exposed to SOGI conversion therapy [ 3 ]; and the Trans Pulse Canada survey (N = 2033) found that 11% of transgender and non-binary people had experienced conversion therapy [ 12 ].
Survivor characteristics
In Canada, men who have sex with men (MSM) who have been exposed to SO or GI conversion efforts or practices were more likely to be gay (compared to bisexual), transgender and non-binary (compared to cisgender), “out” about their sexual orientation (relative to those who were not), younger, immigrants, and to earn an annual personal income of less than $30,000 (compared to those who earn $60,000 or more [ 3 , 4 ]. The TransPULSE study found increasing rates of conversion therapy experiences with age [ 12 ]. In a US cohort of middle-aged and older MSM, Meanley et al. [ 13 ] found lower exposure to conversion therapy among MSM with any college education, but higher exposure among participants who enrolled in the studies post-2001 (compared to those enrolled pre-1987). Among US youths, Green et al. [ 7 ] found a higher prevalence of conversion experiences among gay and lesbian youths (relative to youths identifying as bisexual or as “something else”) and those from low-income families.
Conversion effort exposure appears to be evenly distributed before and after the age of 18 years. Societal, legal, and cultural homo- or trans-negativity is often endorsed by parents of LGBTQI2+ youths [ 14 , 15 ], leading them to seek conversion efforts for their children. Furthermore, these beliefs may lead LGBTQI2+ child(ren) to believe that they would be more accepted if they were heterosexual and cisgender. Growing up with cultural and parental cisheteronormative values is thus likely to influence LGBTQI2+ persons to initiate, be exposed to, or participate in conversion efforts, whether voluntarily or not.
To explore such societal, legal, or cultural contexts, previous studies have relied on variables such as race/ethnicity, age cohort, religious affiliation, or family’s support of SOGIE. Salway et al. [ 4 ] found greater SO conversion therapy prevalence among Canadian Indigenous individuals and other racial minorities (relative to White men), but no differences were found between age groups. The study found that conversion efforts were far more common among trans respondents (12.1% versus 3.5%). Salway et al. [ 3 ] found that the prevalence of SOGI conversion therapy practices was higher among younger generations, immigrants, and racial/ethnic minorities. Meanley et al. [ 13 ] found a greater prevalence of these practices among US middle-aged and older Black MSM (both non-Hispanic and Hispanic) and those of other racial minority groups (compared to non-Hispanic White men), while Green et al. [ 7 ] found a higher prevalence among Hispanic/Latinx youths. In Ryan et al.’s [ 8 ] sample, respondents who were not born in the US were more likely than those born in the US to report having been taken to a therapist or religious leader by their parents to change their SO. Hypothesizing the role of more conservative values, Flores et al. [ 16 ] found lower support for banning conversion therapy among US racial and cultural minority groups. This conclusion supports the finding that ethnic minority parents report greater levels of homonegativity than ethnic majority parents [ 17 ]. Given the between-country variations in attitudes toward SOGIE, we can expect variations in exposure to conversion efforts depending on the country of birth.
Youth who underwent SO or SOGI conversion therapy are also more likely to come from religious families [ 8 ] or to have heard their parents (or caregivers) use religion to justify saying negative things about LGBTQ individuals [ 7 ]. Adamson et al. [ 18 ] found that, in their worldwide sample, about one-fourth of respondents who have been exposed to conversion efforts indicated that they had sought conversion therapy on their own, while the rest of the sample reported that this decision was beyond their control or made on their behalf by their family, religious leaders or community, school, or employer. They also found that most practitioners who led conversion therapy were mental health providers, followed by religious authorities or their associates.
While LGBTQI2+ people in Canada have been subjected to SOGIE conversion efforts, data are still scarce as most studies are limited to sexual minority men and specifically to SO conversion efforts. In Quebec, the only prevalence estimates available come from the Sex Now survey data, which found conversion therapy rates of 4.2% for SO [ 4 ] and 6.8% for SOGI [ 3 ] among Canadian sexual minority men. While little is known about conversion efforts among other sexual orientation groups (e.g., bisexual and pansexual individuals) and across genders and gender modalities (i.e., cisgender or transgender), rates of conversion efforts appear higher among transgender people [ 3 , 4 , 12 , 19 ]. Moreover, as asexuality has only been recently recognised as different from sexual desire disorders [ 20 ], it is likely that persons describing their sexual orientation as asexual are more likely to have experienced sexual orientation conversion efforts or to have sought services to help them change. Also, to our knowledge, data on intersex persons’ experiences with gender identity assignment or modification are also scarce, though such experiences are likely as intersex variations are treated as a medical condition falling under sex/gender (re)assignment. Relying on a large, province-wide community-based survey, the current study describes the prevalence of SOGIE conversion attempts and involvement in conversion services, as well as their sociodemographic correlates, among LGBTQI2+ persons in Quebec.
Participant recruitment
Data on SOGIE conversion experiences were collected as part of the Understanding the Inclusion and Exclusion of LGBTQ People (UNIE-LGBTQ) research project, which aimed to document events during which LGBTQI2+ people (aged 18 years and older) were demeaned, rejected and belittled, or deprived of the full extent of their rights in important life domains. Participants were recruited from September 2019 to August 2020 (before any legal ban on conversion therapy in Quebec or Canada) through the project’ and community partners’ communication channels (emails, listservs, the project website, Facebook pages and groups, Twitter, and LinkedIn), web and printed media, and word of mouth. The survey was administered online and was available in both French and English. Inclusion criteria were understanding French or English, being at least 18 years old, self-identify as LGBTQI2+, and live in the province of Quebec.
Over 6,000 persons accessed the online questionnaire, of which we retained only those who provided a valid Quebec postal code or whose IP address was located in the province (n = 6,095). Participants who did not provide sufficient data to confirm their eligibility or who did not meet the inclusion criteria were excluded (n = 1,115, of which 11 did not consent, 71 were younger than 18, and 85 were not LGBTQI2+). The final sample was composed of 4,980 participants. The present paper is based on the data of the 3,261 respondents who provided information on their exposure to SOGIE conversion attempts or their involvement in SOGIE conversion services. This study was approved by the Institutional Research Ethics Board of the Université du Québec à Montréal (Québec, Canada) (Protocol #2775).
We assessed lifetime involvement in conversion therapy services and lifetime exposure to conversion attempts. Both were measured separately for SO and GIE, as social attitudes and professional guidelines toward sexual diversity and gender diversity are different. The four items used to assess these constructs, and their response options, are presented in Table 1 . The research team created the survey questions based on the scientific literature and by consulting experts on conversion therapy and key informants from community-based organizations.
- PPT PowerPoint slide
- PNG larger image
- TIFF original image
https://doi.org/10.1371/journal.pone.0265580.t001
Questions on lifetime involvement in conversion services were introduced by explicitly stating the aim of such services. Participants were provided with the following instructions: “The next questions ask about the contacts you may have had with services for which your aim was, for instance, [see Table 1 for specific wording of the aim for SO and GIE] . These services may have been provided by health professionals, spiritual or religious guides, or other types of people. These services may go by various names, including therapy or treatment (conversion, reparative, or corrective), special consultations, spiritual processes, healing or deliverance sessions, or other names you may be familiar with. Answer the following questions in relation to all the services you have been in contact with taken together, whether this was on your own initiative or upon someone else’s request (parent, partner, spiritual advisor, etc.)”. Contrary to these organized efforts, conversion attempts refer to any direction or advice to change someone’s SOGIE, make them conform to cisheterosexist norms, or to prevent them from becoming gay, lesbian, bisexual, or transgender.
We asked those who were involved in conversion services to provide information on their most recent experience: their age at the time, and the type of service provider (response options were: a doctor or psychiatrist; a psychologist; a sexologist; another type of therapist or psychotherapist; a member of the clergy, of a religious group, or of a church; no recollection of the person; other). We also inquired about the goals of the services. For SO conversion, the goals were: “to prevent you from being or becoming gay, lesbian, or bisexual”; “to change your sexual orientation (e.g., toward heterosexuality)”; and “to change how you express yourself in your body (your mannerisms, your ways of speaking, moving, walking, dressing, doing your hair, etc.)”. For GIE conversion, the possible goals were: “to prevent you from being or becoming trans”; “to change your gender identity (e.g., to become cisgender)”; and “to change how you express your gender identity with your body (your mannerisms, your ways of speaking, moving, walking, dressing, doing your hair, etc.)”. The four response anchors were dichotomized: not at all (coded 0); a bit (coded 0); somewhat (coded as 1); and a lot (coded as 1). Respondents also indicated whether they themselves, their parents (or their representatives), or someone else consented to these services and whether their conversion purposes were explicit from the beginning (response options: yes; no).
We also explored six potential motivations to seeking conversion services: 1) “I thought it would be easier for me and for my future if I tried”, 2) “I wanted to become [heterosexual, or cisgender] or to avoid becoming [gay, lesbian, or bisexual, or trans]”, 3) I was afraid of negative consequences if I refused to try (e.g., family rejection, refusal of care, termination of treatment), 4) “I felt that my loved ones would be happy if I did it”, 5) “I could not say no to the person or people who suggested it to me”, and 6) “They convinced me it was a good idea to try”. The response options ranged from 0 (Totally false) to 3 (Totally true).
Additional data on year of birth, intersex variation, sexual orientation, gender modality and identity, race/ethnicity, education, place of birth, household income, parents’ religious attendance, and perceived parents’ attributed importance to religious upbringing were also collected.
Data analysis
Descriptive statistics were computed to summarize the sample’s characteristics. Continuous variables were presented as means and standard deviations, or as medians and intervals defined by the first and third quartiles. For dichotomous variables, their prevalence and 95% exact confidence intervals (CI) were calculated [ 21 ]. For categorical variables, we presented the proportion of each category and the corresponding 95% CI were calculated simultaneously for multinomial proportions [ 22 ]. Chi-square or Ficher exact tests were used to compare the distributions of the lifetime exposure to SOGIE conversion attempts and involvement in conversion services between cisgender LGBQ+ and trans participants. Crude Poisson regression with a robust error variance [ 23 ] was applied to assess the associations between lifetime exposure to SOGIE conversion attempts or service involvement and participant’s characteristics on the prevalence ratio (PR) scale. Analyses were performed using STATA 16.1 and SAS 9.4.
Missing data on the outcome variables followed a monotone pattern reflecting sections order in the online questionnaire, ranging from 34.5% (for conversion services involvement) to 39.7% (for conversion attempts). For both outcomes, weak associations [ 24 , 25 ] were found between the presence of missing data and education (Cramer’s V between 0.12 and 0.13), and between the missingness in SOGIE conversion services involvement and birth cohort (Cramer’s V = 0.12), suggesting that missing data on the outcome variables were not completely random. Participants with a university degree and older participants were more likely to have completed the questionnaire. The percentage of missing values in the analytic sample was below 9% for most variables included in the present paper but exceeded 10% for two variables (parental religious attendance and attitudes). Statistical guidelines suggest that bias is negligeable with less than 10% missingness [ 26 ]. Missing values were not replaced. The significance level was set at p < 0.05.
Participants
Table 2 presents the sample’s characteristics. While most participants were born after 1980, multiple birth cohorts were represented. Most participants described their sexual orientation as gay or lesbian (59%), bisexual (17%), or pansexual (10%). Over 80% of the sample was cisgender (43% women, 40% men), and 17% were transgender or non-binary (12% trans men and non-binary assigned female at birth, 5% trans women and non-binary persons assigned male at birth). Fourteen persons reported intersex variations. Most of the sample was white (89%) but included indigenous people (3%) and people of color (8%). Over half of participants reported a college or university degree (56%), most were born in Canada (87%), and were equally distributed across the four assessed household income brackets. About one-third of respondents reported that their parents never attended religious services and did not attribute any importance to religious upbringing.
https://doi.org/10.1371/journal.pone.0265580.t002
Lifetime prevalence of SOGIE conversion attempt exposure and involvement in conversion services
Overall, 26.4% (95% CI, 24.8% to 28.0%) of respondents have experienced lifetime SOGIE conversion attempts or have been involved in conversion services (see Table 3 ). Cisgender sexual minority participants were more likely to have experienced conversion efforts targeting their SO (20.0%, 95% CI, 18.4 to 21.5) than their GIE (6.2%, 95% CI, 5.3 to 7.2), while trans participants were more likely to have been targeted for their GIE (41.9, 37.5 to 46.4) rather than their SO (25.6%, 95% CI, 21.8 to 29.7). Overall, trans participants were more likely to have been exposed to SOGIE conversion attempts and involved in SOGIE conversion services.
https://doi.org/10.1371/journal.pone.0265580.t003
SOGIE conversion attempts
Over two-thirds of respondents identified family members as responsible for the SOGIE conversion attempts (see Table 4 ), followed by friends and acquaintances, members of the clergy, and relationship (ex-)partners. Ten percent or less of participants identified healthcare professionals as responsible for such efforts. Trans participants were more likely than their cisgender LGBQ+ counterparts to have experienced GIE conversion attempts by friends or acquaintances (28.4%, 95% CI: 22.2% to 35.1% vs 15.3%, 95% CI: 9.8% to 22.2%), relationship (ex-)partner(s) (22.9%, 95% CI: 17.3% to 29.3% vs 11.1%, 95% CI: 6.5% to 17.4%), and healthcare professionals (12.9%, 95% CI: 8.6% to 18.4% vs 2.1%, 95% CI: 0.4% to 6.0%).
https://doi.org/10.1371/journal.pone.0265580.t004
Table 5 reports sociodemographic correlates of SO and GIE conversion attempts. SO conversion attempts were more commonly experienced by respondents who were bisexual, pansexual, and asexual (compared to gay/lesbian), transgender (compared to cisgender), indigenous and racialized (compared to white), and those whose parents were more likely to attend religious services (compared to never ) and to at least somewhat value religious upbringing (compared to not at all ). SO conversion attempts were less common among participants who had a college or university education (compared to less than college), who were born in Canada (compared to those born abroad), and who reported an annual household income of over $30,000 CAD (compared to < $30,000 CAD).
https://doi.org/10.1371/journal.pone.0265580.t005
GIE conversion attempts were more commonly experienced by participants who were born in 1981–1990 and after 1990 (compared to those born before 1955), who reported an intersex variation (compared to endosex respondents), who were bisexual, pansexual, queer, and asexual (compared to gay/lesbian), transgender (compared to cisgender), transmasculine and transfeminine (compared to cisgender women), indigenous and racialized (compared to white), and by participants whose parents extremely valued religious upbringing (compared to not at all ). GIE conversion attempts were less commonly experienced by respondents with a college or university education (compared to less than college) and by those who reported an annual household income of over $60,000 CAD (compared to < $30,000 CAD).
Involvement in SOGIE conversion services
Regarding SOGIE conversion services’ involvement (see Table 6 ), respondents born after 1990 reported the lowest prevalence (2.5%, 95% CI 1.8% to 3.4%), with a gradual increase among older cohorts. Participants born before 1955 were the most likely to have been involved in these services (11.7%, 95% CI, 7.7% to 17.2%) compared to other age cohorts, as were transgender participants (PR = 1.59, 95% CI, 1.10 to 2.30), cisgender men (PR = 1.62, 1.12 to 2.36) and transfeminine participants (PR = 3.28, 1.94 to 5.55) compared to cisgender women, indigenous (PR = 2.10, 95% CI, 1.10 to 4.03) and racialized participants (PR = 2.08, 95% CI, 1.33–3.26) compared to white, and those whose parents attended religious services at least 3 times a year, compared to never , and to value religious upbringing at least somewhat , compared to not at all ).
https://doi.org/10.1371/journal.pone.0265580.t006
Regarding the most recent involvement in SOGIE conversion services ( Table 7 ) results show a wide range in terms of the age at which it took place, with as early as 2 years old and as late as almost 60 years old (median age = 18 years). Over half of occurrences occurred after 2000, with trans participants being more likely to have experienced such involvement after 2009 (57.1, 95% CI: 36.8 to 75.3) compared to cisgender ones (24.8, 95% CI: 16.0 to 36.3). Most commonly, the services were provided by healthcare professionals (doctors, psychiatrists, psychologists, or sexologists), a member of the clergy, another type of professional (e.g., counselors, therapists, teachers, etc.) or, less commonly, by a relative or a family friend. Multiple service providers were identified, which suggests that multiple persons provided conversion services, or that some of them occupied multiple functions (e.g., both a healthcare professional and a member of the clergy, both a sexologist and physician, etc.).
https://doi.org/10.1371/journal.pone.0265580.t007
Among cisgender participants, conversion services’ main goals were to make them heterosexual (69.0%) or to prevent them from being gay, lesbian, or bisexual (62.4%). Among trans participants, the most reported goals were to make them heterosexual (83%), change their gender identity (68.2%) or their gender expression (60.0%), or to prevent them from being or becoming transgender (65.2%).
Among respondents who were involved in SO conversion services, about 52% consented themselves, of whom only 55% were clearly aware of the services’ objectives (see Table 8 ). About 48% reported that their parents (or a family member) consented on their behalf, with over 60% of them indicating that the family member(s) did so with clear awareness of the services’ objectives. An additional one-fifth of participants who were involved in SO conversion services reported that someone other than family consented on their behalf, being cognizant of the services’ objectives in over 80% of cases. The most frequently endorsed reasons for using such services were that they thought it would be easier for them and for their future if they tried, and that they could not say no to the person or people who suggested it.
https://doi.org/10.1371/journal.pone.0265580.t008
Approximately 56% of respondents having been involved in GIE conversion services consented themselves, 30% of whom were cognizant of these services’ conversion goals. Forty percent reported that their family consented for them, with clear awareness of the services’ objectives in 40% of cases. One-fifth of the participants who were involved in GIE conversion services reported that someone other than family consented on their behalf (e.g., physician, member of the clergy, psychologist, friends, school staff, etc.), close to 63% of whom were clearly aware of the services’ objectives. The main reasons endorsed for using these services were to make their lives and futures easier, to please their loved ones, and because they feared negative consequences in case of refusal (e.g., family rejection, refusal of care, termination of treatment, etc.).
This study is the first to report data on lifetime exposure to various forms of SOGIE conversion efforts across all gender identities and modalities and sexual orientation groups in Canada. We used data from a large community-based survey to investigate SOGIE prevalence and correlates among LGBTQI2+ people in the province of Quebec. This study revealed that 4.4% of the sample used SOGIE conversion services, with higher prevalence rates among trans participants (PR = 1.59, 95% CI, 1.10 to 2.30). The overall rate of conversion service involvement was close to those reported for Quebecois MSM in the Canadian Sex Now survey (4.2%, [ 4 ]; 6.8%; [ 3 ]). In the current study, conversion services involvement among transgender participants (6.3%) was lower than that reported in the US Transgender Survey (i.e., 14%; [ 6 ]).
SOGIE modification attempts were far more prevalent than conversion services involvement in the current LGBTQI2+ sample (25%), particularly among trans participants who were about 7 times more likely to report so compared to cisgender participants. In comparison, Salway et al. [ 5 ] report a lower prevalence among sexual-minority men (15% in Quebec, 20% across Canada). Disparities in these estimates may reflect variations in the wording of the phenomenon, such as services involvement, sustained efforts [ 5 ], conversion therapy [ 1 , 7 , 13 ], reparative therapy [ 7 ], attempts or efforts [ 3 ], treatment or cure [ 8 ], or sexual repair/reorientation [ 4 ], as well as geographical variations in the conversion services offered and in the societal attitudes toward sexual and gender diversity across the US and Canada, and in Quebec more specifically.
Correlates of conversion services involvement
It should be noted that licensed healthcare providers were responsible for about half of the current sample’s most recent conversion experiences, and members of the clergy or of a religious group, for about one-third. Over half of participants reported having consented to SOGIE conversion services. These services’ objectives, however, were clear to only 55% of those who engaged in SO conversion and to 30% of those who engaged in GIE conversion, which suggests that the goal of conversion became known to these participants only once after being involved in the process. These numbers are higher than those of a previous study that included participants from over 100 countries and showed that only one-fourth of the sample have sought conversion services on their own, while the rest of respondents declared that the decision was largely outside of their control [ 18 ].
The results also show that other persons were also involved to varying degrees in these decisions (parents, extended family, religious congregation members, or school personnel, including private school personnel, which are assumed to be religious), and that these individuals were more likely than the participants to have been aware of the services’ conversion goals. Overall, conversion services involvement among Quebec LGBTQI2+ persons likely resulted from concerted efforts from their immediate environment. Given that the most frequently endorsed reasons to consent to or comply with these services were the wish for a better future and the fear of rejection, it is also likely that these individuals were swayed by ambient hostility toward sexual and gender diversity, leading them to believe that SOGIE conversion was their best option. The results further revealed that a high percentage of participants, parents, and family members were unaware of conversion services’ goals, suggesting that they may involve deception or manipulation, especially in relation to GIE conversion services. To increase power when exploring for correlates, we merged participants who reported having accessed any SO or GIE conversion services. This decision was supported by our finding that response patterns concerning both services were similar. Contrary to Salway et al. [ 3 ] who found a greater exposure to conversion therapy practices among younger generations of Canadian MSM, we observed a birth cohort effect regarding the accessing of conversion services, with older cohorts being more likely than younger ones to report having done so. This pattern may reflect changes in societal attitudes and professional regulations that oppose SO conversion practices, and only more recently, GIE conversion practices.
Accessing SOGIE conversion services was also more commonly reported by indigenous and racialized participants, as well as by those from more religious families. These findings support those of previous studies, and suggests that these groups may endorse more conservative values and stricter sexuality and gender norms (often imported from a colonial past; see Barker [ 27 ]), which contribute to create a hostile climate toward sexual and gender diversity and to increase the likelihood of seeking SOGIE conversion services [ 15 ]. While there were no variations between sexual orientation groups regarding SOGIE conversion services involvement, we found that transgender persons and those assigned male at birth (cisgender, transgender, or non-binary) presented increased risk. This points to a lower threshold for gender (non-)conformity tolerance toward persons assigned male at birth. Contrary to Salway et al. [ 4 ], low-income participants were not more likely to have been involved in SOGIE conversion services than those with higher incomes.
Correlates of conversion attempts
While our findings regarding SOGIE conversion attempts also confirm the role of sociocultural context, differences between SO and GIE conversion attempts are noteworthy. While SO conversion efforts occurred in similar proportions across birth cohorts, GIE attempts were mainly reported by younger generations. This could reflect socially and politically conservative reactions to increased consultations regarding GIE variations among younger generations [ 28 ]. Such conversion attempts could also be due to more recent cohorts of non-binary and transgender persons coming out earlier due to increasing trans visibility, and while still living in their parents’ homes, which can make them more vulnerable to family pressure and other cisnormative influences.
Both SO and GIE conversion attempts were more commonly reported by less educated and lower income participants, while SO conversion attempts more specifically were more common among those who were from more religious households and who were born outside Canada. These results confirm previous findings about the key role of geographical and socioeconomic factors in creating a social or family context that is hostile to sexual and gender diversity. As Salway et al. [ 4 ] suggested, it is possible that the association between ethnicity and racialized status and SO conversion efforts may be at least partially explained by the mediating effect of socioeconomic factors. Yet, as exposure to SOGIE conversion likely happened before the income and education level measured at the time of the study, it is more likely that exposure to SOGIE conversion efforts has negatively impacted the socioeconomic trajectory, a hypothesis that is also suggested by other authors [ 8 ].
That SOGIE conversion attempts were more commonly reported by individuals who identified as other than gay or lesbian can reflect the greater acceptance and recognition of gay and lesbian persons, while other sexual identities remain misunderstood (e.g., bisexuality and pansexuality) or conceptualized as sexual disorders (e.g., asexuality). Results revealed how cisnormativity can also affect intersex persons, who were more likely than their endosex counterparts to have been exposed to GIE, but not SO, conversion attempts. Moreover, our results showed that, compared to their cisgender counterparts, transgender persons were more exposed to both SO and GIE conversion attempts. Their higher exposure to SO conversion efforts might reflect how gender (non)conformity is often taken as a sign of non-heterosexuality. Unlike conversion services, there were no significant differences in the rates of conversion attempts between trans people assigned male and assigned female at birth.
Strengths and limitations
This study is the first to examine exposure to both SO and GIE conversion attempts and conversion services involvement across multiple sexual orientation groups and gender identities and modalities in a large sample. Yet, this work also has some limitations. First, its cross-sectional, retrospective design is subject to recall bias and prevents any causal inferences. Second, as for any self-selected, non-probabilistic sampling, it is likely that the LGBTQI2+ persons who volunteered to participate are different from those who did not. While we used multiple, diversified recruitment strategies, the results cannot be generalized beyond the present sample. Third, as the SOGIE conversion experiences were elicited using non-validated self-reports, our indicators may not have accurately captured their prevalence.
Despite these weaknesses, this study provides a unique overview of Quebec’s LGBTQI2+ populations’ SOGIE conversion experiences, including women’s (cisgender and transgender). The results highlight that while conversion services involvement was more common among older generations, conversion attempts were more common among younger ones. Our findings also show the increased vulnerability to conversion attempts and service involvement among participants with religious upbringing, indigenous persons and people of colour, intersex, transgender, non-binary and asexual persons, as well as those who did not have a monosexual sexual orientation (bisexual, pansexual).
To protect LGBTQI2+ persons from such attempts and practices, legal bans on conversion practices are an important step as they send a strong message about their unethical and harmful nature. However, they will not be insular to faith-based practices and they will be insufficient to eliminate pressures and practices covertly operating under the guise of exploration. Professionals’ ongoing commitment is sorely needed, professional associations must expand their statements regarding sexual orientation and gender identity and expression practices, and healthcare providers need adequate training in LGBTQI2+ affirmative approaches. Religious counselors should also address the religious beliefs and cisheterosexist assumptions underlying their spiritual guidance or clinical practice. Addressing such biases does not imply deconstructing their religious beliefs, but rather exploring how their faith can impact their clinical practice [ 29 , 30 ]. Moreover, as families play a key role in pressuring children into conversion practices, they need to be supported and counseled in the acceptance of their LGBTQIA+ children. More studies are needed to better understand parental and family characteristics associated with heterosexism and cissexism.
Supporting information
S1 file. alternative language abstract..
https://doi.org/10.1371/journal.pone.0265580.s001
Acknowledgments
The Understanding the Inclusion and Exclusion of LGBTQ People research (UNIE-LGBTQ) is a research partnership of universities, public agencies, semi-public and community-based organizations, and private enterprises dedicating their efforts to better understand situations in which LGBTQI2+ people are demeaned, rejected, and belittled, and deprived of the full extent of their rights in important life domains. We extend our thanks to the research partners as well as to the participants who generously shared their experiences with us.
- 1. The Trevor Project. National Survey on LGBTQ Mental Health. [Internet]. 2019 [cited 2021 Apr 21]. https://www.thetrevorproject.org/survey-2019/
- 2. Ashley F. Model Law–Prohibiting Reparative Practices [Internet]. McGill University; 2020. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3398402
- View Article
- PubMed/NCBI
- Google Scholar
- 5. Salway T, Lachowsky N, Kwag M. Conversion Therapy & SOGIECE in Canada—Sex Now Survey results reveal prevalence of change efforts. Vancouver: Community-based Research Centre. [Internet]. 2020. https://www.cbrc.net/sex_now_survey_results_reveal_prevalence_of_change_efforts
- 10. SQ 2020, c 28 | An Act to protect persons from conversion therapy provided to change their sexual orientation, gender identity or gender expression [Internet]. CanLII; [cited 2021 Dec 6]. https://www.canlii.org/en/qc/laws/astat/sq-2020-c-28/latest/sq-2020-c-28.html
- 11. Government Bill (House of Commons) C-4 (44–1)—First Reading—An Act to amend the Criminal Code (conversion therapy)—Parliament of Canada [Internet]. [cited 2021 Dec 6]. https://www.parl.ca/DocumentViewer/en/44-1/bill/C-4/first-reading
- 12. The Trans PULSE Canada Team. QuickStat #1 –Conversion Therapy. 2019-12-20. [Internet]. 2019. https://transpulsecanada.ca/research-type/quickstats/
- 24. Rea LM, Parker RA. Designing and Conducting Survey Research: A Comprehensive Guide. John Wiley & Sons; 2014. 352 p.
- 27. Barker J. Critically sovereign: Indigenous gender, sexuality, and feminist studies. [Internet]. Critically Sovereign. Duke University Press; 2020 [cited 2021 May 28]. https://www.degruyter.com/document/doi/10.1515/9780822373162/html
- 28. Brady CE, Ernst MM. Pediatric Gender Identity: Consultation on Matters of Identity, Transgender Concerns, and Disorders/Differences of Sex Development. In: Carter BD, Kullgren KA, editors. Clinical Handbook of Psychological Consultation in Pediatric Medical Settings [Internet]. Cham: Springer International Publishing; 2020 [cited 2021 Dec 6]. p. 439–49. (Issues in Clinical Child Psychology). https://doi.org/10.1007/978-3-030-35598-2_33
- Open access
- Published: 04 February 2021
Sexual orientation, gender identity and gender expression-based violence in Catalan universities: qualitative findings from university students and staff
- Elena María Gallardo-Nieto 1 ,
- Aitor Gómez 1 ,
- Regina Gairal-Casadó ORCID: orcid.org/0000-0003-0093-7912 1 &
- María del Mar Ramis-Salas 2
Archives of Public Health volume 79 , Article number: 16 ( 2021 ) Cite this article
39k Accesses
9 Citations
11 Altmetric
Metrics details
Hate crimes have raised in Spain and the gender and sexuality-based conflicts persist worldwide which leads to this problem having an effect on health and wellbeing. Following a focus of transforming Higher Education Institutions, this research analysed the problem that affects undergraduate students in six Spanish universities. The research goal is to improve the life quality of lesbian, gay, bisexual, transgender, queer and intersex university students, breaking the silence that exists around the violence that this group suffer in Catalonia, Spain.
Following the Communicative Methodology, this study has identified violence based on sexual orientation, gender identity or gender expression in the target universities and provided guidelines to improve anti-discrimination protocols. A qualitative method has reached experiences of university students, heads of equality commissions, professors and administrative staff regarding this conflict. Focussing on the qualitative research tools, 30 semi-structured interviews were conducted with university students and staff around issues related to the violence against lesbian, gay, bisexual transgender, queer and intersex students: 1) perception of violence and discrimination, 2) institutional measures, 3) actions against violence. An analysis of exclusionary and transformative dimensions was used to identify emergent themes.
We have identified two dimensions for the analysis given their impact in contributing or overcoming violence: exclusionary and transformative. A wide range of forms of violence on the grounds of sexual orientation, gender identity and gender expression perpetrated at universities have been identified as exclusionary facts and described by participants in the study. Equality commissions have not received reports of violence based on sexual orientation, gender identity or gender expression, and university staff shows certain unfamiliarity regarding the measures and politics to prevent and intervene in cases of violence against the lesbian, gay, bisexual, transgender, queer and intersex community. Among the results identified as transformative are the ways through which actions of lesbian, gay, bisexual, transgender, queer and intersex groups against violence and the professors’ commitment to intervene have a relevant impact on student’s wellbeing. An improvement and implementation of anti-discrimination protocols with mandatory applicability has also been documented.
Conclusions
Findings highlight the need of collecting more evidence that contributes to the improvement of protocols, measures and politics to protect all the members of the university community. A better understanding of violence based on sexual orientation, gender identity and gender expression in HEI’s may guide national and international governments to improve the health and well-being of lesbian, gay, bisexual, transgender, queer and intersex persons.
Peer Review reports
Violence based on sexual orientation, gender identity or gender expression is present in our society and within the university community [ 1 , 2 , 3 ]. Numerous international studies have shown that the lesbian, gay, transgender, queer and intersex (LGBTQI+) community have more risk and probabilities to suffer sexual discrimination or harassment during their university trajectory [ 2 , 3 ]. Furthermore, the risk of being object of violence increases in the case of transgender students [ 4 , 5 , 6 ]. National politics and international agendas have given priority to the legislation and regulation to end with LGBTQI-phobia [ 7 , 8 ], even though the risk of suffering sexual harassment is still higher in the case of sexual minorities [ 1 , 6 , 9 , 10 ]. The case of Spanish universities reflects the international panorama in relation to the LGBTQI+ academic community [ 11 ]. Educating in diversity, tolerance and acceptance towards diversity is crucial, but international reports show that this is still a pending issue in Spain [ 12 ]. The lack of literature and research about how this phenomenon affects Higher Education Institutions (HEI’s) is striking and generates a significant silence towards the situation of the LGBTQI+ community and the consequences of LGBTQI-phobia in their personal, academic and health status. As a response to this reality, the research Uni4freedom seeks to contribute to breaking the silence that goes along the LGBTQI+ community at HEI’s, improving the quality of life of the academic community and the struggle against violence based on sexual orientation, gender identity and gender expression in the Catalan context.
The main challenge when studying the discrimination against the diversity of sexual orientations, gender identities and expressions is the diversity of violence manifestations. A change in the ways violence against the LGBT community is manifested, has been shown in the literature in the last years, shifting towards more subtle and unnoticed manifestations [ 6 ]. Verbal forms of violence [ 9 , 13 , 14 ], homophobic jokes [ 10 , 15 , 16 ], anti-LGBT paintings, graffities and threats [ 3 , 13 ], social distance [ 10 , 15 , 17 ], not-inclusive or acceptance spaces [ 18 ] and possible risk of suffering from unprotected forms of sex and AIDS’ contagion [ 19 ] have been identified as advanced forms of violence based on sexual orientation or gender identity or expression. On the one hand, the case of a hostile environment is conditioning the free expression of the felt gender identity and sexual orientation [ 9 , 18 , 19 , 20 , 21 , 22 ]. On the other hand, all these forms and manifestations of violence can generate a response of internalization and normalization of the homophobic actions, perpetuating the violence and affecting negatively in the life quality and wellbeing of the LGBT+ academic community [ 3 , 16 , 22 , 23 , 24 , 25 ].
According to the findings in the scientific literature, violence and discrimination based on sexual orientation and gender identity and expression, has consequences in three spheres of the LGBT university students’ life. Firstly, it affects the health status, both physically and mentally. It has been shown that LGBT students present higher symptoms of depression and anxiety [ 9 , 13 ] and suffer various forms of physical ache [ 10 , 16 ]. Secondly, it affects their academic performance, presenting a lower grade in average in comparison to hetero-cis students [ 26 ]. This difference of academic results has been analysed as an aftereffect of LGBT stigmatization creating difficulty to focus on their studies [ 19 , 27 ], having further consequences in their future possibilities and academic success [ 24 ]. Thirdly, these realities of LGBT-phobia in HEI’s promote exclusionary climates and negatively affects the cohesion and relationality of sexual minority students [ 22 ]. The seen or suffered experiences of harassment or discrimination can generate a feeling of isolation and exclusion [ 6 , 26 ] which can be reinforced by the institutional invisibility of LGBT perspectives and role models [ 13 ].
Evidence shows six different axes to prevent and intervene in front of violence based on sexual orientation and gender identity and expression within university institutions. Visibility of the LGBTQI+ collective and their situation in the university scope is key to prevent LGBTQI-phobia. Besides, generating profound awareness of university members is necessary to be able to face the problem of LGBT-phobia [ 1 , 28 ]. In order to make this awareness effective and reach the whole academic community, the inclusion of LGBT literature in academic curriculums has the highest impact in the reduction of LGBT-phobia [ 18 , 28 ]. Another protective factor for the prevention and intervention in cases of violence based in sexual orientation, gender identity and gender expression is the explicit institutional support towards the LGBTQI+ community through the implementation of politics and strategies towards the reduction of hetero-sexism [ 6 , 9 , 29 , 30 ].
This article presents qualitative evidence about how to overcome this form of gender inequality in a very relevant social institution. We have chosen a qualitative method in order to delve into the complexities of suffering or witnessing violence at HEI’s and the possibilities of intervention that participants identify in their own interpretation. This methodological choice aims to reinforcing the knowledge and contrasting the depth and complexities of the qualitative findings of the project. Very important issues to be considered when preparing policies for the prevention and intervention of LGBTQI-phobia are thus presented . In conclusion, the study aimed to give visibility to the violence based on sexual orientation, gender identity or expression that takes place in HEI’s, and to identify successful practices and decisions for the eradication of this violence.
This article has been focussed it research methodology for social impact. The voices of the end-users of the research have been incorporated in all phases of the research, in order to contribute to the social impact and social transformation of the conflict [ 31 ]. To make that possible, the methodological design is based on the Communicative Methodology of Research (CMR) [ 32 ], which stands out for its capacity to identify successful actions that contribute to overcoming inequality and to generate social policies based on these actions. CM stands out for generating scientific knowledge through the contrast of the scientific evidence (contributed by the researchers) and the contributions of the social agents’ participants in the research, defined as the world of life [ 33 , 34 , 35 ].
The study was designed to understand how, why, in which forms and circumstances this form of violence in HEI’s take place affecting university students’ life, health status and future. Given the scientific evidence on LGBTQI+ violence prevalence and the aims of the research, the main research objective is to improve the quality of life of LGTBIQ university students, breaking the silence that exists about the violence they suffer.
Following the communicative perspective, Uni4Freedom has implemented mixed-methods research [ 34 ] of which the qualitative techniques’ results are presented in this article. Semi-structured interviews Footnote 1 with communicative orientation have composed the fieldwork of the study taking place in six universities of the Catalan region [ 36 , 37 , 38 ]. The fieldwork has been designed in order to, firstly, make an approach and a diagnose of the reality that the LGBTQI+ community faces at Catalan universities and, secondly, delve into the perspective of university staff and professors, exploring the possibilities to implement and propose transformative actions for the inclusion and non-discrimination. The population target of the study is the academic community enrolled in different disciplines within the project’s six partnering Catalan universities Footnote 2 : students, university professors, administrative staff and heads of equality commissions or units at these institutions.
Communicative organization of the research
In order to ensure the social impact of the research, the voices of the LGBTQI+ community and LGBTQI+ organizations have been included in different forms and phases during the study. Their participation has been indispensable, contributing with reciprocity, advice and follow-up to guarantee that the research objectives are met and ensuring ethics’ standards in the methods. The Advisory Board is a follow-up and supervising body which has been formed by representatives of organizations of reference on LGBTQI+ rights in the territory Footnote 3 . In two different stages of the project and face-to-face meetings in 2018 and 2020, this board has debated and reviewed the methodological plan, research technics, findings and proposals grounding the materials in their experience and expertise in LGBTQI+ rights and reality. Their contribution has contributed to comply with ethical principles as well as to ensure the work and results for the improvement of the situation of the LGBTQI+ community at Catalan HEI’s.
We have conducted 12 semi-structured interviews with communicative orientation to LGBTQI+ university staff from the partner universities of the project. Besides, we have conducted 4 semi-structured interviews with communicative orientation to heads of equality units or commissions from the partner universities of the project. And finally, 12 communicative daily life stories with University students have also been done. These technics have followed the communicative orientation of the methodology by facilitating reflective dialogues between participants and researchers about the incidence of violence due to sexual orientation, identity or gender expression faced in their careers as university professor/staff or student. Proposals to make university a more LGBTQI+ friendly space were also gathered from these qualitative work. The distribution of research tools and participants has been as follows:
Research tools
The guidelines of the interviews have been designed following the communicative perspective, attending to the results of the literature review and contrasted with the Advisory Committee. This combination in the design process has allowed us to develop complex guidelines that enable the identification of situations, characteristics and circumstances that either promote or allows to transform situations of violence based on sexual orientation, gender identity or expression at HEI’s. We have identified three sections that have let us build the data collection process of the interviews. In what follows, the structure of the interview under the three sections and some of the questions of the interview’s guidelines are introduced:
To describe and presentgeneral aspects of the research method, theme, exploring different perspectives and ideas in relation to the reality of the situation of the LGBTQI+ community in University.
To study the experience or perception of violence based on grounds of sexual orientation, gender identity or expression at University or spaces related to the institution according to the results of the literature review. The opening question of this section in the case communicative daily life stories with students was the following:
“If you know of any cases of violence due to sexual orientation, gender identity or gender expression, comment on it:
Do you think that the people who suffer from any of these situations are considered victims of violence because of their sexual orientation, gender identity, or gender expression. Why? Why not?
What was your reaction to the situation of violence? Why?
What was the victim’s reaction to the violence or discrimination? Why?
If it was reported to the university, what was the institution’s response? How did they interpret it? How does the institutional response affect the victim’s decisions and behaviors?
What consequences did the fact of reporting have on the aggressor? And on the victim?
Do you know what has to be done in the case of suffering a situation of violence due to sexual orientatio, gender identity or gender expression?”
To approach the perception of institutional strategies to detect, prevent and intervene in cases of LGBTQI-phobia by the research participants attending to their different roles in the community. Two questions from the semi-structured interviews with university staff from this third section were the followings:
“In the section on harassment and discrimination, the inclusion of sexual orientation and gender identity/expression in anti-discrimination policies and the approval of protocols against LGBTI-phobia is considered. Some universities, such as Oxford, Tuft and UCL, have explicit online policies regarding sexual orientation, and other ones have specific policies concerning the trans* community, as well as policies to ensure inclusive language.
Do you think that this would be convenient at your university? Do you think it would be appropriate? Do you think it would be viable? Why? What benefits would it have and how would students experience it?”
“Finally, on training for members of the university community to detect, prevent and act against LFBTI-phobia. Universities like Pennsylvania and Washington train the community to ensure Safe Zones, zones free of any violence, and others like Cambridge and Oxford train the community in successful actions, such as bystander intervention and providing online resources.
Ethical validation
The study has received the ethical validation of the ethical committees of Girona University and Lleida University in 2019. After submitting a detailed protocol for the fieldwork, containing consent forms and interview guidelines, the Ethics and Biosafety Committee of the University of Girona approved the start of the fieldwork. For the second ethical approval, the Committee for the approval of research studies at the Faculty of Nursing and Physiotherapy of the University of Lleida approved the fieldwork plan, consent forms and guidelines for interviews under the ethical requirements of confidentiality and good praxis without any objections.
Consent forms were systematically signed by all research participants and by the researchers implementing the tools, in order to ensure the former’s rights in the research. These forms helped us to protect their right to confidentiality, anonymity, wilfulness, possibility to stop or leave the study at any moment and receive all necessary information for their involvement by the researcher.
Aside of the institutional validation, the research counted with an Advisory Board which supervised, followed-up and advised the research team in three different phases: approval of the literature review, fieldwork plan and preliminary results of the study. This board was composed by members of the LGBTQI+ community, university students and representatives of active organizations for LGBTQI+ rights of the territory Footnote 4 . Their belonging to the targeted community was due to the need of including the voices of the end-users of the research throughout the whole process of the research. The role of the board has been to relate the theory and scientific evidence to the daily reality of the LGBTQI+ community, reinforcing the transformative role of the research through their very contributions in the study.
Data analysis
The analysis chart has been designed to collect contributions from interviews and communicative daily life stories considering all the dimensions and categories selected (Table 1 – Result analysis chart). Dimensions are located in the rows and refer to the two sorts of results depending on their contribution or transformation of the target conflict, referring to the Communicative Methodology. Categories are the concepts that are being used in the research process to analyse the results of the fieldwork and they are located in the columns (Table 1 – Result analysis chart). The categories have been defined through a deductive method of definition, meaning that they have been determined before fieldwork through the study of scientific literature regarding LGBTQI-phobia in HEI’s. The categories resulting from this study are: LGBTQI-phobic violence, actions against the violence and university politics and measures against the violence.
The research team has processed the qualitative results of the fieldwork ensuring the anonymity of the participants in all the phases of the study. Members of the research team have transcribed the interviews and daily life stories verbatim. Then, the research team has coded the transcription by using the numbers of the designed analysis chart (Table 1 – Result analysis chart), identifying results and matches between the targeted categories and dimensions on the transcriptions. We have not made use of any software or program for the systematization of this process.
In this section, we have made an in depth approach to the research target: studying violence against LGBTQI+ community in HEI’s. On the one hand, we have analysed the results that do not contribute to overcoming the problem of violence based in sexual orientation, gender identity or expression, encompassed within the exclusionary dimension. On the other hand, we have analysed the contributions that have an influence in transforming and overcoming the targeted violence in HEI’s, included in the transformative dimension. All of the results presented belong to the research tools and the research participants already mentioned in the fieldwork subsection (Table 2 - Fieldwork distribution).
Violence’s normalization and internalization
Normalization and internalization of LGBTQI-phobia are the most present consequences of the violence in HEI’s. These results show the need to promote measures of awareness-raising to promote respect to diversity. Under this category, we highlight the normalization of violence in the daily discourses at universities as a consequence of the constant violence against the LGBTQI+ community. The normalization of violence is funded on naturalizing discriminatory comments towards the LGBTQI+ community, which can happen even within classrooms, as stated by a LGBTQI+ university professor in an interview:
Then, inside the class, let me think... at the break and when we leave and so on, I’ve seen someone say to another "hey faggot, you didn't get the work done today!" maybe they said that and, I don't know, I have it so incorporated that I don’t realize either.
In this sense, students have also shared in everyday life stories experiences that prove the naturalization of discriminatory discourses towards the LGBTQI+ community, as stated by a female undergraduate and LGBTQI+ student in a communicative daily life story:
Well, I don’t know, if in class or between classes, we are talking, or they are talking, so in a group, and they want to refer to a boy as being a freak or weaker than the rest they refer to him as a faggot.
The LGBTQI+ participant students in the research have claimed the consequences of the normalization of the violence. Following their discourse, they have found that reproduction of homo and lesbo-phobic comments and the self-internalization of the violence are results of having received a LGBTQI-phobic socialization. As a female and LGBTQI+ student expresses in a communicative daily life story:
Many times, I think they overlook these comments because we are used to them. For me what happens to me is like, if one day I hear someone say butch or something, it's not hard for me to pass but I guess I would think that he’s an asshole, you know? But then I would think that, he’s silly and that's it and I wouldn't take it as something personal, but as something more social that looks normal.
Transgender vulnerability in the conflict
Research has shown that transgender people are the most prone to have difficulties and to suffer violence or discrimination at HEI’s [ 4 , 5 , 6 ]. This form of vulnerability in the university context is even more disturbing when the results show the complexity and accumulation of forms of violence that only transgender students suffer. There can be specific circumstances that transgender students live, such as the social transition and the bodily changes, elements that can make their educational process at university even harder when belonging to the LGBTQI+ community. As a transgender student states in a communicative daily life story regarding the transitioning:
Then I made the transition and it's like that, with the medication and that, I was like super confused with many things, I was relocating mental issues, because in the end I didn't know many things either, because the medication numbed me and I don't know. Of course, I did notice suspicion and misunderstanding and a feeling of being something weird, feelings of disgust, by some colleagues and I realized it but well, as I’m saying I tried to ignore it because I have enough problems.
The exclusionary discourses, looks and refusal perception is clear in the voice of the interviewed people, showing the need of promoting measures of awareness raising that advocate the respect to diversity and differences. In this sense, the need of intervention and respect towards the transgender groups is especially relevant, as it has been shown in the interviews’ fragments.
Unfamiliarity of institutional mechanisms and interventions
Secondly, findings on university policies and measures have indicated the lack of actions, university policies and measures to fight violence and, at the same time, they prove the ignorance of professors and staff about the mechanisms to prevent and intervene in cases of LGBTQI-phobia. Furthermore, the lack of cases of violence due to sexual orientation, gender identity or expression reported at equality offices indicates the complexity of this form of violence and the likely unawareness about violence based on the grounds of sexual orientation, gender identity and gender expression by officials at universities. The fact that some Heads of University Equality Offices claim not to have received complaints regarding violence based on sexual orientation, gender identity or expression is relevant, as one experienced worker on an Equality Office shared regarding the cases of LGBTQI-phobia in an interview:
The truth is that no. I have not dealt with any cases at the observatory, no petitions nor expositions have been received of violence based on gender identity or sexual orientation. We haven’t realized it. For me, it hasn’t come directly to me as a teacher or as a colleague. It hasn’t reached me. I know it’s a college reality, but the truth is I can’t say it’s a reality for me because I haven’t seen it.
The figure ‘0’ of cases of violence based on sexual orientation, gender identity or expression at universities can be explained by the lack of mechanisms and abilities by university professors and staff to identify and detect the violence [ 6 , 39 , 40 ]. Moreover, it could also be justified by the attempts to generate safe and friendly spaces for the LGBTQI+ community to make the process of filing a complaint of LGBTQI-phobia easier. As we can see in the following fragment from a communicative daily life story with a transgender student which has already faced the process of name change, he reflects on other possibilities to it within HEI’s:
I think that a trans person should not go through an equality unit to request a name change, right? But I think that this could already be done in a much easier administrative process of administrative, that is, how you do your... You fill out your application for the first time, that is, in that database, what if there were what is called a chosen name?
The lack of knowledge from university professors, staff and officials about measures, resources and officials of reference in cases of LGBTQI-phobia has been stated in the interviews as a constant reality, as mentioned by a female university professor in an interview: “I’m not responsible. I don’t know if within the management team there is someone in charge of this policies in case there is a problem.”
We have identified other indicators apart from unawareness which could respond to the lack of a support network for victims of LGBTQI-phobic violence within HEI’s. Many university policies and educational protocols for the prevention and intervention in cases of violence based on sexual orientation, gender identity or expression have been developed in the last years from Equality Units and Commissions and other spaces towards equality and against discrimination in HEI’s. The ignorance of the international scientific evidence about the existig policies carries a limitation in the struggle against the violence towards the LGBTQI+ community. This is due to the lack of knowledge and training on the measures and the roots of LGBTQI-phobia for the implementation. In order to understand the notions on institutional measures to intervene in conflicts based on sexual orientation, gender identity or expression, we can see an active LGBTQI+ university professor’s discourse where he discusses the thoughts on the transgender name-change process as it follows a fragment of an interview:
The doubt that I was holding is the legal part. Without a doubt the university has to support straight away and if it is necessary to change, it is changed [referring to the name], if you have special needs, it has to be attended, they have to be listened to and we have to see what can be done, of course. What confuses me a little is the legal issue. (…) To the official lists, they appear with the birth name, but they can be changed, and it seems viable, and they are comparable because at the end, that’s the name that they identify with. “I do not identify myself with Antonio José... I identify myself with Toni.” And it seems very comparable. If this person wants to change the name of Maria to Peter because he identifies himself as Peter, so Peter be it and that’s it. What I find most complicated is at a more internal level, for example in the records, that you have the name changed because there would probably be a conflict of legal identity.
In this sense, students agree in recognizing that ignorance complicates the process of identification and support in particular situations of LGBTQI-phobia at universities. For that reason, training and awareness raising on LGBTQI+ issues are both considered very necessary towards turning all university members into agents of change, whether being or not part of the LGBTQI+ community, as a cis-heterosexual female student points out in a communicative daily life story:
I think so, I have not experienced these situations, and I don’t know these type of situations. I'm sure it happened. I think that it should be known both for those who do not know it and for those who suffer it or have seen it, to know that they are not alone that someone is aware of the issue and that they take measures against these situations and that there are those points of help. There are also people who do not want to come out of the closet and they may have problems but they will not ask for help because they have not yet come out of the closet, so it would be good for them to know that there are actions that can help them without anyone knowing anything and keeping their secret. It is an option for those people to have help.
University as a safe space
Secondly, on the variable LGBTQI+ actions against violence findings point at the existence of three protective factors that lead to overcoming violence and discrimination: HEI’s perceived as safer spaces compared to other places, compromise and predisposition of professors to successfully prevent and intervene in cases of violence and university protocols and measures of intervention including all university community. This is due to the role of Equality Units, their familiarity, respect and openness has an important effect in the prevention and intervention of cases of LGBTQI-phobia. We have identified that HEI’s offer a very wide window of possibilities for intervention, acceptance and respect compared to other spaces, as a LGBTQI+ female student points out in a communicative daily life story:
Sexual diversity is more comfortable at university than in other places and that’s why I also think it’s sometimes easier to make more demands within university, right? Because as there is this freedom or this friendly climate, right? Friendly to make claims, to make demands for improvement, so it’s easy to get it and therefore I think that precisely freedom encourages more freedom of expression, right? And more diversity.
Another protective factor within HEI’s towards the LGBTQI+ community and for the transformation of the violence and discrimination is related to the compromise of professors to prevent and intervene. The alliance between students and professors is especially valuable when having the support of a more powerful group within the educational institution in terms of decision and action. This particular support can be offered for different reasons, firstly for the training, awareness and activism in terms of rights by professors. Next, the importance and urgency of intervening in order to transform and stop the conflict based on gender or sexual diversity is made explicit by one of the LGBTQI+ university professors interviewed:
Having just one victim is enough to talk about it and explain that these things are happening, anonymously. If not, we have to orient ourselves differently, lead it in a way that if things happen socially, we try not to let them happen here. Obviously, they shouldn’t take place anywhere. We protect the space; I think we have to find a balance in that so as not to create an alarm.
The compromise to intervene in cases of violence based on sexual orientation, gender identity or expression has been expressed in different forms in the discourses of LGBTQI+ staff. The following case goes one step further as, aside of an open commitment with LGBTQI+ issues, this social conflict is taken into consideration as part of the very teaching praxis. As a result of this, we see how a safer space in the classrooms can be created, by making sexual and gender diversity an issue in the lectures. A LGBTQI+ male professor - committed to openly talking and discussing about matters of gender, sexuality and diversity in class-, talks about the reaction of his students when addressing these issues:
No! Not in class, maybe that's because we criticize it, and make people think and everything is politically correct...to let them see their experiences based on that and then see how they act...of course, in class I guess that they are aware that it would not look very good for them to do joke about it if we are working for them not to do so in their own environments.
When breaking the silence on the issue of LGBTQI-phobia so that the topic becomes a recurring theme in the classroom, students become active upstanders questioning themselves and intervening in cases of violence [ 41 ]. In this sense, another cis-heterosexual university professor highlighted in the interview the need to break the silence and generate mechanisms facilitating that people dare to complain:
It may also be that things are happening and we don’t know it because there aren’t protocols, so this is also a way to encourage people who are going through things to report it. Because violence is always hidden actions. If this is giving them a little encouragement to report and explain what is happening, even if the violence is not physical, that is verbal, that is behavioural, exclusionary...
The value of receptiveness and alliances
Thirdly, on the variable university policies and measures, we have identified evidence of the openness towards sexual and gender diversity by university professors, also considering the need of prevention and intervention plans and measures of high quality in order to transform the reality. This is the case of protocols and measures of intervention generated by the Equality Units at HEI’s that have been interviewed. They highlight the quality and connection with the reality of the LGBTQI+ community of their regulations and intervention measures in their own Units. This is due to the success of negotiation processes between HEI’s and Equality Units, thanks to the sanctions that exist in case of not implementation and to the inclusion of gender identity and sexual orientation perspectives in the regulations. This is introduced by a long experienced worker on the service of the Head of an Equality Office at one participant university in an interview:
We have a regulation for the prevention of gender violence. The difference between regulation and protocol is that all other universities have protocols, ours has sanctions. The others do not have it typed. Our regulation -which was one of the first to be done, but which had two years of negotiation with the University-, is a comprehensive one because it covers the entire university community (officials, staff, professors, students) and it is also a one that entails penalties that many of the university’s protocols do not have. Then what we have done is the adaptation of it, when we already made the regulation, we put for example everything that was harassment due to sex and sexual orientation, we added all the sexual orientation tag.
The interviewees have shown willingness to learn the measures and implement them in the Catalan University contexts, even though if they have not received any training in LGBTQI+ issues. The following fragment refers to a LGBTQI+ male university professor’s interview referring to the measures of trans-inclusion at their institution:
Of course, as the number does not change, so there is no problem, and everything is linked to the ID number and instead you can change the name. I think it’s ok, if there is a real need for it and it is a request from individuals or the community itself, I do not see it difficult and do not see a problem. I think it would bother me to call this person by the name with which they do not feel identified. If they tell me to change the name, I tell them that way, because otherwise there is not an effective dialogue, so I think that if possible, I think it’s perfect and go ahead.
Predisposition and interest by professors have appeared in the qualitative fieldwork together with the claim of needing scientific evidence as well as the inclusion of voices of the own community and of experts in the field. Then they could advise and orientate regarding measures and politics at HEI’s. A university professor claimed it during the interview as follows:
Totally, but I think that the experts here are somehow the ones who have to take the lead because I do not consider myself an expert on the subject, I am a total ignorant, because I find it hard to find the right words to talk about this community, if we are referring to differentiated groups. Mm, I feel I can talk about certain things, but when I think about it, I think that maybe I had not realized it. My normal life is not affected, but there might be other people’s life who is (…) and then if the need exists and the university has the measures to make it feel normal, so that this becomes of normality, then I will be happy to follow any training that is needed because for me it is also an exciting topic, not morbid-like, but to know. Because it is becoming more and more visible.In the same way that this professor commented, another student also claimed the need of measures and politics to have some support in case of suffering violence based on sexual orientation, gender identity or expression. The following statement is a fragment of LGBTQI+ activities and university student’s communicative daily life story, reflecting clearly on the need of feeling institutional protection in order to feel integrated at University:
That people feel safer, better, that they have a real moral and psychological support because until now, they are not considering themselves part of anywhere. Having such a policy would help us a lot to feel that we belong and that we are considered part of something because, of course, we are having to face these LGTB-phobic behaviours and they have to be counteracted with something, right?
Our study demonstrates the urgency of the conflict taking place at HEI’s on the grounds of sexual orientation, gender identity and gender expression. It has also provided us with the scientific evidence and the protagonists’ discourses by bringing to discussion how both dimensions match and complement each other when facing conflicts, needs and discrimination based on sexual orientation, gender identity and gender expression. Furthermore, the study has added relevant knolwedge to previous research with an evidence-based approach and successful cases to improve protocols and strategies for the struggle against the problem of LGBTQI-phobia taking into account the voices of the university community in the Catalan context. Contributing to the previous research on gender violences at Catalan and Spanish universities [ 31 ], our study has gone further in studying the problem of gender violence against the LGBTQI community in HEI’s for the first time in Catalonia. The complementarity of both the generation of evidence and new proposals of avenues for the improvement of current protocols, policies and measures towards the inclusion of the LGBTQI+ community sets a precedent on how to turn HEI’s into more LGBTQI+ inclusive institutions.
Challenges in identifying violence
There is plenty of evidence about how the conflict of violence based on sexual orientation, gender identity or expression is a current reality, which is visible and has become a relevant subject for the development of international policies and agendas in Europe [ 42 ]. Furthermore, the scientific literature describes how this conflict can permeate social institutions, affecting subjects in different spaces, dimensions and degrees. The main challenge identified in the struggle against this social conflict is its identification and detection in institutions, as it has been mutating and changing its form to avoid being detected [ 6 ].
Our study has, not only proven the existance of a variety of forms of direct violence that take place in HEI’s, but it has also identified more subtle and unnoticed forms of violence. Verbal forms of violence, such as homophobic and transphobic comments and jokes, paintings and non-inclusive spaces and classrooms are just the more apparent forms of violence pointed out in the research [ 9 , 10 , 13 , 14 , 15 , 16 , 18 ]. What has made the situation in the Catalan context more complex is the generalized reaction of internalization shown by LGBTQI+ victims and other agents. As the literature highlights, this response of normalization and naturalization of the violence against sexual or gender diversity contributes in the reproduction of the violence against the LGBTQI+ community [ 3 , 16 , 23 , 24 , 25 ].
Besides the reaction of the victims and the LGBTQI+ community, the responses from the rest of institutional agents facing the conflict are especially significant. As mapped by the research, the role of other students and peers [ 27 ], professors and staff is key when approaching the cases of LGBTQI-phobia at university, as the relationality, authority and influence is compelling [ 8 , 20 , 21 , 22 ]. As the findings have shown, their availability, openness and attitude towards the LGBTQI+ community and sex and gender diversity can have an impact on the perception of classrooms and university campuses as free and safe spaces. Additionally, we have found how previous debates or workshops of LGBTQI+ issues at university classrooms can prevent some forms of LGBTQI-phobia from happening. As well, these previous experiences on discussing gender could facilitate processes of social transition, reception of reports of violence or discrimination, improving the perception of the university as a friendlier and safer space. In addition, the heads of Equality Units’ figure entails two different roles: as social agent and worker as well as a representative in terms of equality and non-discrimination in the institution. In any case, this readiness and preparation does not suffice while numbers show that there are no cases of LGBTQI-phobia arriving to institutional instances in some of the participant HEI’s.
Damage on wellbeing of LGBTQI+ students
Given the findings about the prevalence of violence on the grounds of sexual orientation, gender identity and gender expression in Catalan universities, the negative impact on the well-being and life quality of LGBTQI+ students is a fact. If the existence of violence against sexual and gender diversity in university spaces is a reality, the probability of having students suffering physically and mentally, presenting symptoms of depression, anxiety and various forms of physical ache are a worrying reality for the institution [ 9 , 13 , 16 ]. Furthermore, this difficulty affecting only a group of students would generate a gap in the access, quality and academic success compared to the rest of the community due to their health status [ 25 ]. The lack of social cohesion within the university community and students, has a high impact in the present and future of LGBTQI+ students in Catalonia. LGBTQI+ stigmatization also results in impediments for LGBTQI+ students to reach the same academic level and success than the rest of the students [ 19 , 23 , 43 , 44 ].
The findings about the damage of the LGBTQI+ students at University has given visibility to the risk that the LGBTQI+ community suffers which also affects their wellbeing. This evidence indicates that the generation of successful strategies to prevent, detect and intervene in cases of violence on the grounds of sexual orientation, gender identity and gender expression is urgent. This emergency lies on the institutional duty of offering quality higher education for everyone without of any type of discrimination. In order to eliminate any form of discrimination effective anti-discrimination strategies based on scientific evidence need to be developed.
University policies and measures a the LGBTQI-phobia
Given the results about the implemented strategies to fight and prevent forms of violence on the grounds of sexual orientation, gender identity and gender expression, issues on the evaluation, quality and follow-up of these measures are still pending. The evidence shows that the current strategies to fight, prevent and intervene in cases of LGBTQI+ realities in Catalonia are configured as responses to concrete and specific situations. This conception of the LGBTQI+ reality as a transitory conflict and circumstance implies that the forms of intervention planned only take into account the specific conflict, without paying attention to a reality that is present in all the spheres of the university. This can respond to the lack of continuous and more transversal actions that educational systems implement to carry out more equitable actions for the inclusion of LGBTQI+ realities within HEI’s.
Giving visibility and raising awareness of the LGBTQI+ circumstance is a very pressing issue present both in the literature and in the results of the research, as it can prevent different forms of LGBT-phobia. These actions are identified as protective factors in the prevention and intervention of discrimination and violence on the grounds of sexual orientation, gender identity and gender expression, as well as for generating and imporving the LGBTQI+ students’ feelings of belongingness to HEI’s. More in depth, literature and participants have identified the need of training professors and other university staff about LGBTQI+ perspective [ 1 , 28 ]. This could have an impact on the way conflicts and discrimination on the grounds of sexual orientation, gender identity and gender expression is managed with professionals, ensuring safe follow-up and accompaniment processes by educators and staff -who would be trained on the situation of the LGBTQI+ community through scientific evidence-.
In order to translate this process of making LGBTQI+ issues a closer reality to the university community, the inclusion of literature from a LGBT+ perspective in the academic curriculum has been identified as having the highest impact for the reduction of violence and discrimination on the grounds of sexual orientation, gender identity and gender expression [ 20 , 28 ]. Its implementation would require HEI’s to include LGBTQI+ issues horizontally in all university degrees’ classrooms, considering as an institutional duty the need of ensure freedom of living and expressing sexual and gender diversity. Another way of institutionally protecting the LGBTQI+ community is by explicitly supporting the community as has been informed by the literature [ 6 , 9 , 29 , 30 ]. Lastly, the urgency of addressing the transgender issues at universities is present in both the project’s results and literature [ 45 ], highlighting the need of articulating successful practices and accompanying processes to transgender students for the improvement of their health [ 43 ]. This would require that universities start conceiving the transgender reality as a continuous, individual and changing phenomenon that goes beyond the name and gender change in the identification documents, affecting the live of students with different intensity and in different stages and social circles.
Altogether, the complexity of assessing and reviewing the success and impact of university protocols, measures and strategies to intervene is both a scientific and socio-political issue, attending to the changing political circumstances that affects the European and Spanish context. The research limitations that have affected the study have been closely related to the human interactions during the fieldwork, the protection of the anonymity, the search for gender and sexual minority participants and the issues of visibility and public recognition of participants. For that reason, we have worked very hard in the ethical framework and approval to ensure everyone’s safety, respect, confidentiality and support during and after the fieldwork. Otherwise, the qualitative method and results of the study have also set limits on the applicability and transferability of the findings. Although quality-centred findings do not offer results that can be generalized to the whole Catalan university community, they have allowed us to delve into the reality of the Catalan HEI’s through the discourses of university staff and students.
Following our research goal of improving the quality of life of LGBTQI+ university students, through the CM and breaking the silence that exist about this sort of violence, the study identified protective and exclusionary factors likely to have a high impact in the quality of life of University LGBTQI+ students in the Catalan region. This innovative and transformative focus has provided the dialogue-based methodology on the study of the conflict of gender and sexual diversity in the most relevant educational institution.
The need of studying the conflict of LGBTQI-phobia at universities lies on the importance of higher education in the lives of students and in their future possibilities. It also falls on the strong impact of suffering violence and discrimination for several years while the right of living one’s sexual orientation, gender identity and gender expression freely is not guaranteed. All of this shows how gender and sex norms permeate educational institutions [ 46 , 47 ], making visible the current positioning of Catalan HEI’s against LGBTQI-phobia and towards a more inclusive and diverse university community.
New avenues and research targets on this matter could contribute to identifying other needs and axes of actions that could be essential in the struggle against LGBTQI-phobia. On the one hand, investigating the positioning of professors in the classrooms and their previous training on gender and LGBTQI+ perspective with a base on scientific evidence could open new lines of research for the prevention of violence. Furthermore, the inclusion of LGBTQI+ literature to be addressed in classrooms and the impact of normalizing gender and sex diversity in educational institutions would also be relevant. Our study highlights the importance of the alliance of university professors in the struggle against LGBTQI-phobia as upstanders in the conflict, an issue that must be paramount in new research lines and actions against violence on the grounds of sexual orientation, gender identity and gender expression. On the other hand, studying the case of transgender needs and trajectories in HEI’s is still a pending issue. Tackling the need to underst transgender identities and non-binary gender expressions within the institutional framework would contribute to detect and explain forms of violence yet to be identified as well as the strategies to counter these.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Interviews had an approximate duration of 40 min and the place was chosen by both participant and researcher. Interviews were normally implemented in public spaces which allowed the researcher to generate an atmosphere of trust, such as cafeterias or university offices. The materials result of the interviews were the manual transcriptions made by members of the research team of the Uni4Freedom project. Then, the analysis took place as it follows in the Data Analysis subsection.
The partner universities of Uni4Freedom are: Rovira i Virgili University; University of Barcelona; University of Girona; University of Lleida; Ramón Llull University and University of Vic.
Participant entities and organizations on the Advisory Board:
Col·lectiu H2O · Gais, Lesbianes, Bisexuals i Transsexuals del Camp de Tarragona.
SAI Tarragona - Servei d’Atenció Integral a les Diversitats Sexuals i de Gèneres de Tarragona.
Xarxa Solidària de Vctimes de Violència de Gènere a la Universitat.
Gènere Lliure.
Col·lectiu de gèneres i sexualitats dissidents (GSD).
The participant entities in the Advisory Committee have been:
- Col·lectiu H2O (Gais, Lesbianes, Bisexuals i Transsexuals del Camp de Tarragona).
- SAI Tarragona - Servei d’Atenció Integral a les Diversitats Sexuals i de Gèneres de Tarragona: suport social, informació i atenció piscològica i jurídica.
The participant universities in the study are:
Rovira i Virgili University.
Girona University.
Lleida University.
Vic University.
Barcelona University.
Ramón Llull University.
Abbreviations
Communicative Methodology
Higher Educational Institution
Community of lesbian, gay, bisexual, transgender, queer, intersexual and other groups with non-conforming and dissident identities, orientations or expressions
Costa AB, Peroni RO, de Camargo ES, Pasley A, Nardi HC. Prejudice toward gender and sexual diversity in a Brazilian Public University: prevalence, awareness, and the effects of education. Sex Res Soc Policy. 2015;12(4):261–72.
Article Google Scholar
McGinley M, Wolff JM, Rospenda KM, Liu L, Richman JA. Risk factors and outcomes of chronic sexual harassment during the transition to college: examination of a two-part growth mixture model. Soc Sci Res. 2016;60:297–310.
Rankin SR. Campus climates for sexual minorities. New Dir Stud Serv. 2005;111(Special Issue: Gender Identity and Sexual Orientation: Research, Policy, and Personal):17–23.
Google Scholar
Coulter RWS, Rankin SR. College sexual assault and campus climate for sexual- and gender-minority undergraduate students. J Interpers Violence. 2017;35(5–6):1351–66.
Goodrich KM. Lived experiences of college-age transsexual individuals. J Coll Couns. 2012;15(3):215–32.
Hong JS, Woodford MR, Long LD, Renn KA. Ecological covariates of subtle and blatant heterosexist discrimination among LGBQ college students. J Youth Adolesc. 2016;45(1):117–31.
Council of Europe C. Discrimination on grounds of sexual orientation and gender identity in Europe [Internet]. Paris; 2011 p. 134–134. Available from: https://www.coe.int/t/Commissioner/Source/LGBT/LGBTStudy2011_en.pdf . Accessed 26 Jan 2021.
ILGA-Europe. Annual Review of the Human Rights Situation of Lesbian, Gay, Bisexual, Trans, and Intersex People in Spain covering the period of January to December 2018 [Internet]. 2018 p. 1–2. Available from: https://ilga-europe.org/sites/default/files/spain.pdf . Accessed 26 Jan 2021.
Ellis SJ. Diversity and inclusivity at university: a survey of the experiences of lesbian, gay, bisexual and trans (LGBT) students in the UK. High Educ. 2009;57(6):723–39.
Woodford MR, Han Y, Craig S, Lim C, Matney MM. Discrimination and mental health among sexual minority college students: the type and form of discrimination does matter. J Gay Lesbian Ment Health. 2014;18(2):142–63.
Gallardo Nieto, E. M., Gómez González, A., Gairal Casadó, R., & Ramis Salas, M. del M. (2020). Sexual orientation, Gender Identity and Gender Expression-Based Violence in Catalan Universities: Qualitative Findings from University Students and Staff Research Square https://doi.org/10.21203/rs.3.rs-97327/v1 .
Ávila R. LGBTQI inclusive education report [internet]. Brussles: IGLYO (International Lesbian, Gay, Bisexual, Transgender, Queer & Intersex Youth & Student Organisation); 2018. Available from: https://web.unican.es/unidades/igualdad/SiteAssets/guia-de-recursos/acoso/IE-Full-Report-May-18.pdf . Accessed 26 Jan 2021.
Alessi EJ, Sapiro B, Kahn S, Craig SL. The first-year university experience for sexual minority students: a grounded theory exploration. J LGBT Youth. 2017;14(1):71–92.
Roffee JA, Waling A. Rethinking microaggressions and anti-social behaviour against LGBTIQ+ youth. Safer Communities. 2016;15(4):190–201.
Jewell LM, Morrison MA. “But There’s a Million Jokes About Everybody . . .”: Prevalence of, and Reasons for, Directing Negative Behaviors Toward Gay Men on a Canadian University Campus. J Interpers Violence. 2010;25(11):2094–112.
Woodford MR, Howell ML, Kulick A, Silverschanz P. “That’s so gay”: heterosexual male undergraduates and the perpetuation of sexual orientation Microagressions on campus. J Interpers Violence. 2013;28(2):416–35.
Hamilton L. Trading on heterosexuality - college women’s gender strategies and homophobia. Gend Soc. 2007;21(2):145–72.
Evans NJ, Broido EM. The Experiences of Lesbian and Bisexual Women in College Residence Halls. J Lesbian Stud. 2002;6(3–4):29–42 1.
Mohammadi Gharehghani MA, Khosravi B, Irandoost SF, Soofizad G, Yoosefi LJ. Barriers to condom use among female sex Workers in Tehran, Iran: a qualitative study. Int J Women's Health. 2020;12:681–9.
Lapinski J, Sexton P. Still in the closet: the invisible minority in medical education. BMC Med Educ. 2014;14(1):171.
Rankin SR, Hesp GA, Weber GN. Experiences and perceptions of gay and bisexual fraternity members from 1960 to 2007: a cohort analysis. J Coll Stud Dev. 2013;54(6):570–90.
Rothmann J. The (de)professionalisation of the gay male academic identity: locking the closet door on south African university campuses. South Afr Rev Sociol. 2016;47(4):40–59.
Clarke V. Wearing a gay slogan t-shirt in the higher education classroom: a cautionary tale. Fem Psychol. 2016;26(1):3–10.
Kheswa JG. Exploring the Impact of Discrimination on the Psychological Well-being of Lesbian Students at South African University Campus. Rupkatha J Interdiscip Stud Humanit. 2016;VIII(2):148–55.
Martin-Storey A, August EG. Harassment due to gender nonconformity mediates the association between sexual minority identity and depressive symptoms. J Sex Res. 2016;53(1):85–97.
Woodford MR, Kulick A. Academic and social integration on campus among sexual minority students: the impacts of psychological and experiential campus climate. Am J Community Psychol. 2015;55(1–2):13–24.
Jackman K, Kreuze EJ, Caceres BA, Schnall R. Bullying and Peer Victimization of Minority Youth: Intersections of Sexual Identity and Race/Ethnicity. J School Health. 2020;90(5):368–77.
Deniz C. Reconceptualization sexuality and rethinking homophobia in metropolitan campus spaces. J Crit Educ Policy Stud. 2017;15(1):228–51.
Waldo CR, Kemp JL. Should I come out to my students? An Empirical Investigation. J Homosex. 1997;34(2):79–94.
Article CAS Google Scholar
Garvey JC, BrckaLorenz A, Latopolski K, Hurtado SS. High-impact practices and student–faculty interactions for students across sexual orientations. J Coll Stud Dev. 2018;59(2):210–26.
Puigvert L, Valls R, Garcia Yeste C, Aguilar C, Merrill B. Resistance to and transformations of gender-based violence in Spanish universities: a communicative evaluation of social impact. J Mix Methods Res. 2017;13(3):361–80.
Valls Carol R, Padrós M. Using dialogic research to overcome poverty: from principles to action. Eur J Educ - Wiley Online Libr. 2011;46(2):173–83.
Pulido C, Elboj C, Campdepadrós R, Cabré J. Exclusionary and transformative dimensions: communicative analysis enhancing solidarity among women to overcome gender violence. Qual Inq. 2014;20(7):889–94.
Flecha R, Soler M. Communicative Methdology: successful actions and dialogic democracy. Curr Sociol. 2014;62(2):232–42.
Puigvert L. Preventive socialization of gender violence: moving forward using the communicative methodology of research. Qual Inq. 2014;20(7):839–43.
Vidu A, Schubert T, Muñoz B, Duque E. What students say about gender violence within universities. Qual Inq. 2014;20(7):883–8.
Denzin NK, Lincoln Y. The SAGE handbook of qualitative research. Los Angeles: SAGE; 2017.
Denzin NK. The reflexive interview and a performative social science. Qual Res. 2001;1(1):23–46.
Duhigg JM, Rostosky SS, Gray BE, Wimsatt MK. Development of heterosexuals into sexual-minority allies: a qualitative exploration. Sex Res Soc Policy. 2010;7(1):2–14.
Coleman K. The Difference Safe Spaces Make: The Obstacles and Rewards of Fostering Support for the LGBT Community at HBCUs. SAGE Open. 2016;6(2) Available from: http://journals.sagepub.com/doi/10.1177/2158244016647423 . Accessed 26 Jan 2021.
Valls R, Puigvert L, Melgar P, Garcia-Yeste C. Breaking the silence at Spanish universities: findings from the first study of violence against women on campuses in Spain. Violence Women. 2016;22(13):1519–39.
United Nations. Discriminatory laws and practices and acts of violence against individuals based on their sexual orientation and gender identity [Internet]. United Nations. Human Rights Council; 2011 p. 25. Available from: https://www.ohchr.org/documents/issues/discrimination/a.hrc.19.41_english.pdf . Accessed 26 Jan 2021.
Nicolazzo Z. Trans* in college. Transgender students’ strategies for navigating campus life and the institutional politics of inclusion. Sterling, VA: Stylus Publishing; 2017.
Horn SS, Schriber SE. Bullied and punished: exploring the links between bullying and discipline for sexual and gender minority youth. J Res Adolesc. 2020;30(1):1–18.
Sherman ADF, Clark KD, Robinson K, Noorani T, Poteat T. Trans* community connection, health, and wellbeing: a systematic review. LGTB Health. 2020;7(1):1–14.
Zhang L, Osberg L, Phipps S. Is all bullying the same? Arch Public Health. 2014;72(1):19.
Ferfolja T, Asquith N, Hanckel B, Brady B. In/visibility on campus? Gender and sexuality diversity in tertiary institutions. High Educ [Internet]. 2020 [cited 2020 Jul 8]; Available from: https://doi.org/10.1007/s10734-020-00526-1 .
Download references
Acknowledgements
The authors would like to thank the research participants and collaborators for their important contribution in the study. In particular, we would like to thank to ACUP for their advice and support in all phases of the research. We would also like to acknowledge the support in the data collection to the Advisory Council and all entities participating in it: Col·lectiu H20, SAI Tarragona and Xarxa Solidària de Victimes de Violència de Gènere a la Universitat. We also want to thank the University consortium that enabled the project to take part, formed by Rovira i Virgili University, Lleida University, Girona University, Vic University, Barcelona University and Ramon Llull University. To conclude, we would like to thank all the project collaborators which contribute significantly in data collection and transcription tasks of the fieldwork.
The research leading to these results has received funding from the RecerCaixa program (2017ACUP00235).
Author information
Authors and affiliations.
Universitat Rovira i Virgili, Tarragona, Spain
Elena María Gallardo-Nieto, Aitor Gómez & Regina Gairal-Casadó
Universitat de Barcelona, Barcelona, Spain
María del Mar Ramis-Salas
You can also search for this author in PubMed Google Scholar
Contributions
The first author EMGN contributed to the data collection and writing of the manuscript along with other project collaborators. The second author AGG contributed with the methodological review of the manuscript. The third author RGC participated in the analysis of the results of the study. The fourth author MMRS contributed to the review of the manuscript offering feedback on editing and stylistic issues. All the authors read and approved the manuscript.
Corresponding author
Correspondence to Regina Gairal-Casadó .
Ethics declarations
Ethics approval and consent to participate.
All study protocols were approved by the Ethics Committee of Girona University on December 19th of 2018 and the Committee for the approval of research studies of the Nursing and Physiotherapy Faculty of Lleida University on May 17th of 2019. As well, all participants gave assent to complete the research tools. Development and monitoring of these protocols involved a study advisory group, which included LGBTQI+ academic community and LGBTQI+ organizations of the local territory.
Consent for publication
Consent procedures permitted use of verbatim quotations from participants in suitably anonymised form.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Gallardo-Nieto, E.M., Gómez, A., Gairal-Casadó, R. et al. Sexual orientation, gender identity and gender expression-based violence in Catalan universities: qualitative findings from university students and staff. Arch Public Health 79 , 16 (2021). https://doi.org/10.1186/s13690-021-00532-4
Download citation
Received : 10 November 2020
Accepted : 18 January 2021
Published : 04 February 2021
DOI : https://doi.org/10.1186/s13690-021-00532-4
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Discrimination
- Social problem
- Health education
- Universities
- Sexual orientation
- Gender identity
Archives of Public Health
ISSN: 2049-3258
- General enquiries: [email protected]
MINI REVIEW article
Sexual orientation and gender identity: review of concepts, controversies and their relation to psychopathology classification systems.

- Instituto Universitário de Lisboa ISCTE-IUL, CIS, Lisboa, Portugal
Numerous controversies and debates have taken place throughout the history of psychopathology (and its main classification systems) with regards to sexual orientation and gender identity. These are still reflected on present reformulations of gender dysphoria in both the Diagnostic and Statistical Manual and the International Classification of Diseases, and in more or less subtle micro-aggressions experienced by lesbian, gay, bisexual and trans patients in mental health care. The present paper critically reviews this history and current controversies. It reveals that this deeply complex field contributes (i) to the reflection on the very concept of mental illness; (ii) to the focus on subjective distress and person-centered experience of psychopathology; and (iii) to the recognition of stigma and discrimination as significant intervening variables. Finally, it argues that sexual orientation and gender identity have been viewed, in the history of the field of psychopathology, between two poles: gender transgression and gender variance/fluidity.
Numerous controversies and debates have taken place throughout the history of psychopathology and mental health care with regards to lesbian, gay, bisexual and transgender (LGBT) people. The present paper aims to review relevant concepts in this literature, its historical and current controversies, and their relation to the main psychopathology classification systems.
Concepts and Definitions
Concepts and definitions that refer to sexual orientation and gender identity are an evolving field. Many of the terms used in the past to describe LGBT people, namely in the mental health field, are now considered to be outdated and even offensive.
Sexual orientation refers to the sex of those to whom one is sexually and romantically attracted ( American Psychological Association, 2012 ). Nowadays, the terms ‘lesbian’ and ‘gay’ are used to refer to people who experience attraction to members of the same sex, and the term ‘bisexual’ describe people who experience attraction to members of both sexes. It should be noted that, although these categories continue to be widely used, sexual orientation does not always appear in such definable categories and, instead, occurs on a continuum ( American Psychological Association, 2012 ), and people perceived or described by others as LGB may identify in various ways ( D’Augelli, 1994 ).
The expression gender identity was coined in the middle 1960s, describing one’s persistent inner sense of belonging to either the male and female gender category ( Money, 1994 ). The concept of gender identity evolved over time to include those people who do not identify either as female or male: a “person’s self concept of their gender (regardless of their biological sex) is called their gender identity” ( Lev, 2004 , p. 397). The American Psychological Association (2009a , p. 28) described it as: “the person’s basic sense of being male, female, or of indeterminate sex.” For decades, the term ‘transsexual’ was restricted for individuals who had undergone medical procedures, including genital reassignment surgeries. However, nowadays, ‘transsexual’ refers to anyone who has a gender identity that is incongruent with the sex assigned at birth and therefore is currently, or is working toward, living as a member of the sex other than the one they were assigned at birth, regardless of what medical procedures they may have undergone or may desire in the future (e.g., Serano, 2007 ; American Psychological Association, 2009a ; Coleman et al., 2012 ). In this paper we use the prefix trans when referring to transsexual people.
Since the 1990’s the word transgender has been used primarily as an umbrella term to describe those people who defy societal expectations and assumptions regarding gender (e.g., Lev, 2004 ; American Psychological Association, 2009a ). It includes people who are transsexual and intersex, but also those who identify outside the female/male binary and those whose gender expression and behavior differs from social expectations. As in the case of sexual orientation, people perceived or described by others as transgender – including transsexual men and women – may identify in various ways (e.g., Pinto and Moleiro, 2015 ).
Discrimination and Impact on Mental Health
Lesbian, gay, bisexual and transgender people often suffer from various forms of discrimination, stigma and social exclusion – including physical and psychological abuse, bullying, persecution, or economic alienation ( United Nations, 2011 ; Bostwick et al., 2014 ; European Union Agency for Fundamental Rights, 2014 ). Moreover, experiences of discrimination may occur in various areas, such as employment, education and health care, but also in the context of meaningful interpersonal relationships, including family (e.g., Milburn et al., 2006 ; Feinstein et al., 2014 ; António and Moleiro, 2015 ). Accordingly, several studies strongly suggest that experiences of discrimination and stigmatization place LGBT people at higher risk for mental distress ( Cochran and Mays, 2000 ; Dean et al., 2000 ; Cochran et al., 2003 ; Meyer, 2003 ; Shilo, 2014 ).
For example, LGB populations may be at increased risk for suicide ( Hershberger and D’Augelli, 1995 ; Mustanski and Liu, 2013 ), traumatic stress reactions ( D’Augelli et al., 2002 ), major depression disorders ( Cochran and Mays, 2000 ), generalized anxiety disorders ( Bostwick et al., 2010 ), or substance abuse ( King et al., 2008 ). In addition, transgender people have been identified as being at a greater risk for developing: anxiety disorders ( Hepp et al., 2005 ; Mustanski et al., 2010 ); depression ( Nuttbrock et al., 2010 ; Nemoto et al., 2011 ); social phobia and adjustment disorders ( Gómez-Gil et al., 2009 ); substance abuse ( Lawrence, 2008 ); or eating disorders ( Vocks et al., 2009 ). At the same time, data on suicide ideation and attempts among this population are alarming: Maguen and Shipherd (2010) found the percentage of attempted suicides to be as high as 40% in transsexual men and 20% in transsexual women. Nuttbrock et al. (2010) , using a sample of 500 transgender women, found that around 30% had already attempted suicide, around 35% had planned to do so, and close to half of the participants expressed suicide ideation. In particular, adolescence has been identified as a period of increased risk with regard to the mental health of transgender and transsexual people ( Dean et al., 2000 ).
In sum, research clearly recognizes the role of stigma and discrimination as significant intervening variables in psychopathology among LGBT populations. Nevertheless, the relation between sexual orientation or gender identity and stress may be mediated by several variables, including social and family support, low internalized homophobia, expectations of acceptance vs. rejection, contact with other LGBT people, or religiosity ( Meyer, 2003 ; Shilo and Savaya, 2012 ; António and Moleiro, 2015 ; Snapp et al., 2015 ). Thus, it seems important to focus on subjective distress and in a person-centered experience of psychopathology.
On the History of Homosexuality and Psychiatric Diagnoses
While nowadays we understand that higher rates of psychological distress among LGB people are related to their minority status and to discrimination, by the early 20th century, psychiatrists mostly regarded homosexuality as pathological per se ; and in the mid-20th century psychiatrics, physicians, and psychologists were trying to “cure” and change homosexuality ( Drescher, 2009 ). In 1952, the American Psychiatric Association published its first edition of the Diagnostic and Statistical Manual (DSM-I), in which homosexuality was considered a “sociopathic personality disturbance.” In DSM-II, published in 1968, homosexuality was reclassified as a “sexual deviation.” However, in December 1973, the American Psychiatric Association’s Board of Trustees voted to remove homosexuality from the DSM.
The most significant catalyst to homosexuality’s declassification as a mental illness was lesbian and gay activism, and its advocacy efforts within the American Psychiatric Association ( Drescher, 2009 ). Nevertheless, during the discussion that led to the diagnostic change, APA’s Nomenclature Committee also wrestled with the question of what constitutes a mental disorder. Concluding that “they [mental disorders] all regularly caused subjective distress or were associated with generalized impairment in social effectiveness of functioning” ( Spitzer, 1981 , p. 211), the Committee agreed that homosexuality by itself was not one.
However, the diagnostic change did not immediately end the formal pathologization of some presentations of homosexuality. After the removal of the “homosexuality” diagnosis, the DSM-II contained the diagnosis of “sexual orientation disturbance,” which was replaced by “ego dystonic homosexuality” in the DSM-III, by 1980. These diagnoses served the purpose of legitimizing the practice of sexual “conversion” therapies among those individuals with same-sex attractions who were distressed and reported they wished to change their sexual orientation ( Spitzer, 1981 ; Drescher, 2009 ). Nonetheless, “ego-dystonic homosexuality” was removed from the DSM-III-R in 1987 after several criticisms: as formulated by Drescher (2009 , p. 435): “should people of color unhappy about their race be considered mentally ill?”
The removal from the DSM of psychiatric diagnoses related to sexual orientation led to changes in the broader cultural beliefs about homosexuality and culminated in the contemporary civil rights quest for equality ( Drescher, 2012 ). In contrast, it was only in 1992 that the World Health Organization ( World Health Organization, 1992 ) removed “homosexuality” from the International Classification of Diseases (ICD-10), which still contains a diagnosis similar to “ego-dystonic homosexuality.” However, this is expected to change in the next revision, planned for publication in 2017 ( Cochran et al., 2014 ).
Controversies on Gender Dysphoria and (Trans)Gender Diagnoses
Mental health diagnoses that are specific to transgender and transsexual people have been highly controversial. In this domain, the work of Harry Benjamin was fundamental for trans issues internationally, through the Harry Benjamin International Gender Dysphoria Association (presently, the World Professional Association for Transgender Health, WPATH). In the past few years, there has been a vehement discussion among interested professionals, trans and LGBT activists, and human rights groups concerning the reform or removal of (trans)gender diagnoses from the main health diagnostic tools. However, discourses on this topic have been inconclusive, filled with mixed messages and polarized opinions ( Kamens, 2011 ). Overall, mental health diagnoses which are specific to transgender people have been criticized in large part because they enhance the stigma in a population which is already particularly stigmatized ( Drescher, 2013 ). In fact, it has been suggested that the label “mental disorder” is the main factor underlying prejudice toward trans people ( Winter et al., 2009 ).
The discussion reached a high point during the recent revision process of the DSM-5 ( American Psychiatric Association, 2013 ), in which the diagnosis of “gender identity disorder” was revised into one of “gender dysphoria.” Psychiatric diagnosis was thus limited to those who are, in a certain moment of their lives, distressed about living with a gender assignment they experience as incongruent with their gender identity ( Drescher, 2013 ). The change of criteria and nomenclature “is less pathologizing as it no longer implies that one’s identity is disordered” ( DeCuypere et al., 2010 , p. 119). In fact, gender dysphoria is not a synonym for transsexuality, nor should it be used to describe transgender people in general ( Lev, 2004 ); rather, “[it] is a clinical term used to describe the symptoms of excessive pain, agitation, restless, and malaise that gender-variant people seeking therapy often express” ( Lev, 2004 , p. 910). Although the changes were welcomed (e.g., DeCuypere et al., 2010 ; Lev, 2013 ), there are still voices arguing for the “ultimate removal” ( Lev, 2013 , p. 295) of gender dysphoria from the DSM. Nevertheless, attention is presently turned to the ongoing revision of the ICD. Various proposals concerning the revision of (trans)gender diagnoses within ICD have been made, both originating from transgender and human rights groups (e.g., Global Action for Trans ∗ Equality, 2011 ; TGEU, 2013 ) and the health profession community (e.g., Drescher et al., 2012 ; World Professional Association for Transgender Health, 2013 ). These include two main changes: the reform of the diagnosis of transsexualism into one of “gender incongruence”; and the change of the diagnosis into a separate chapter from the one on “mental and behavioral disorders.”
Mental Health Care Reflecting Controversies
There is evidence that LGBT persons resort to psychotherapy at higher rates than the non-LGBT population ( Bieschke et al., 2000 ; King et al., 2007 ); hence, they may be exposed to higher risk for harmful or ineffective therapies, not only as a vulnerable group, but also as frequent users.
Recently, there has been a greater concern in the mental health field oriented to the promotion of the well-being among non-heterosexual and transgender people, which has paralleled the diagnostic changes. This is established, for instance, by the amount of literature on gay and lesbian affirmative psychotherapy which has been developed in recent decades (e.g., Davis, 1997 ) and, also, by the fact that major international accrediting bodies in counseling and psychotherapy have identified the need for clinicians to be able to work effectively with minority clients, namely LGBT people. The APA’s guidelines for psychotherapy with lesbian, gay, and bisexual client ( American Psychological Association, 2000 , 2012 ) are a main reference. These ethical guidelines highlight, among several issues, the need for clinicians to recognize that their own attitudes and knowledge about the experiences of sexual minorities are relevant to the therapeutic process with these clients and that, therefore, mental health care providers must look for appropriate literature, training, and supervision.
However, empirical research also reveals that some therapists still pursue less appropriate clinical practices with LGBT clients. In a review of empirical research on the provision of counseling and psychotherapy to LGB clients, Bieschke et al. (2006) encountered an unexpected recent explosion of literature focused on “conversion therapy.” There are, in fact, some mental health professionals that still attempt to help lesbian, gay, and bisexual clients to become heterosexual ( Bartlett et al., 2009 ), despite the fact that a recent systematic review of the peer-reviewed journal literature on sexual orientation change efforts concluded that “efforts to change sexual orientation are unlikely to be successful and involve some risk of harm” ( American Psychological Association, 2009b , p. 1).
Moreover, there is evidence of other forms of inappropriate (while less blatant) clinical practices with LGBT clients (e.g., Garnets et al., 1991 ; Jordan and Deluty, 1995 ; Liddle, 1996 ; Hayes and Erkis, 2000 ). Even those clinicians who intend to be affirmative and supportive of LGBT individuals can reveal subtle heterosexist bias in the work with these clients ( Pachankis and Goldfried, 2004 ). Examples of such micro-aggressions ( Sue, 2010 ) might be automatically assuming that a client is heterosexual, trying to explain the etiology of the client’s homosexuality, or focusing on the sexual orientation of a LGB client despite the fact that this is not an issue at hand (e.g., Shelton and Delgado-Romero, 2011 ). Heterosexual bias in counseling and psychotherapy may manifest itself also in what Brown (2006 , p. 350) calls “sexual orientation blindness,” i.e., struggling for a supposed neutrality and dismissing the specificities related to the minority condition of non-heterosexual clients. This conceptualization of the human experience mostly in heterosexual terms, found in the therapeutic setting, does not seem to be independent of psychotherapist’s basic training and the historical heterosexist in the teaching of medicine and psychology ( Simoni, 1996 ; Alderson, 2004 ).
With regards to the intervention with trans people, for decades the mental health professionals’ job was to sort out the “true” transsexuals from all other transgender people. The former would have access to physical transition, and the later would be denied any medical intervention other than psychotherapy. By doing this, whether deliberately or not, professionals – acting as gatekeepers – pursued to ‘ensure that most people who did transition would not be “gender-ambiguous” in any way’ ( Serano, 2007 , p. 120). Research shows that currently trans people still face serious challenges in accessing health care, including those related to inappropriate gatekeeping ( Bockting et al., 2004 ; Bauer et al., 2009 ). Some mental health professionals still focus on the assessment of attributes related to identity and gender expressions, rather than on the distress with which trans people may struggle with ( Lev, 2004 ; Serano, 2007 ). Hence, trans people may feel the need to express a personal narrative consistent with what they believe the clinicians’ expectations to be, for accessing hormonal or surgical treatments ( Pinto and Moleiro, 2015 ). Thus, despite the revisions of (trans)gender diagnoses within the DSM, more recent diagnoses seem to still be used as if they were identical with the diagnosis of transsexualism – in a search for the “true transsexual” ( Cohen-Kettenis and Pfäfflin, 2010 ). It seems clear that social and cultural biases have significantly influenced – and still do – diagnostic criteria and the access to hormonal and surgical treatments for trans people.
Controversies and debates with regards to medical classification of sexual orientation and gender identity contribute to the reflection on the very concept of mental illness. The agreement that mental disorders cause subjective distress or are associated with impairment in social functioning was essential for the removal of “homosexuality” from the DSM in the 1970s ( Spitzer, 1981 ). Moreover, (trans)gender diagnoses constitute a significant dividing line both within trans related activism (e.g., Vance et al., 2010 ) and the health professionals’ communities (e.g., Ehrbar, 2010 ). The discussion has taken place between two apposite positions: (1) trans(gender) diagnoses should be removed from health classifying systems, because they promote the pathologization and stigmatization of gender diversity and enhance the medical control of trans people’s identities and lives; and (2) trans(gender) diagnoses should be retained in order to ensure access to care, since health care systems rely on diagnoses to justify medical treatment – which many trans people need. In fact, trans people often describe experiences of severe distress and argue for the need for treatments and access to medical care ( Pinto and Moleiro, 2015 ), but at the same time reject the label of mental illness for themselves ( Global Action for Trans ∗ Equality, 2011 ; TGEU, 2013 ). Thus, it may be important to understand how the debate around (trans)diagnoses may be driven also by a history of undue gatekeeping and by stigma involving mental illness.
The present paper argues that sexual orientation and gender identity have been viewed, in the history of the field of psychopathology, between two poles: gender transgression and gender variance/fluidity.
On the one hand, aligned with a position of “transgression” and/or “deviation from a norm,” people who today are described as LGBT were labeled as mentally ill. Inevitably, classification systems reflect(ed) the existing social attitudes and prejudices, as well as the historical and cultural contexts in which they were developed ( Drescher, 2012 ; Kirschner, 2013 ). In that, they often failed to differentiate between mental illness and socially non-conforming behavior or fluidity of gender expressions. This position and the historical roots of this discourse are still reflected in the practices of some clinicians, ranging from “conversion” therapies to micro-aggressions in the daily lives of LGBT people, including those experienced in the care by mental health professionals.
On the other hand, lined up with a position of gender variance and fluidity, changes in the diagnostic systems in the last few decades reflect a broader respect and value of the diversity of human sexuality and of gender expressions. This position recognizes that the discourse and practices coming from the (mental) health field may lead to changes in the broader cultural beliefs ( Drescher, 2012 ). As such, it also recognizes the power of medical classifications, health discourses and clinical practices in translating the responsibility of fighting discrimination and promoting LGBT people’s well-being.
In conclusion, it seems crucial to emphasize the role of specific training and supervision in the development of clinical competence in the work with sexual minorities. Several authors (e.g., Pachankis and Goldfried, 2004 ) have argued for the importance of continuous education and training of practitioners in individual and cultural diversity competences, across professional development. This is in line with APA’s ethical guidelines ( American Psychological Association, 2000 , 2012 ), and it is even more relevant when we acknowledge the significant and recent changes in this field. Furthermore, it is founded on the very notion that LGBT competence assumes clinicians ought to be aware of their own personal values, attitudes and beliefs regarding human sexuality and gender diversity in order to provide appropriate care. These ethical concerns, however, have not been translated into training programs in medicine and psychology in a systematic manner in most European countries, and to the mainstreaming of LGBT issues ( Goldfried, 2001 ) in psychopathology.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Alderson, K. G. (2004). A different kind of outing: training counsellors to work with sexual minority clients. Can. J. Couns. 38, 193–210.
Google Scholar
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders , 5th Edn. Arlington, VA: American Psychiatric Publishing.
American Psychological Association (2000). Guidelines for psychotherapy with lesbian, Gay Bisexual Clients. Am. Psychol. 55, 1440–1451.
American Psychological Association (2009a). Report of the Task Force on Gender Identity and Gender Variance. Available at: http://www.apa.org/pi/lgbt/resources/policy/gender-identity-report.pdf
American Psychological Association (2009b). Report of the American Psychological Association Task Force on Appropriate Therapeutic Responses to Sexual Orientation. Available at: https://www.apa.org/pi/lgbt/resources/therapeutic-response.pdf
American Psychological Association (2012). Guidelines for psychological practice with lesbian, gay, and bisexual clients. Am. Psychol. 67, 10–42. doi: 10.1037/a0024659
PubMed Abstract | CrossRef Full Text | Google Scholar
António, R., and Moleiro, C. (2015). Social and parental support as moderators of the effects of homophobic bullying on psychological distress in youth. Psychol. Schools 52, 729–742. doi: 10.1002/pits.21856
CrossRef Full Text | Google Scholar
Bartlett, A., Smith, G., and King, M. (2009). The response of mental health professionals to clients seeking help to change or redirect same-sex sexual orientation. BMC Psychiatry 9:11. doi: 10.1186/1471-244X-9-11
Bauer, G. R., Hammond, R., Travers, R., Kaay, M., Hohenadel, K. M., and Boyce, M. (2009). “I don’t think this is theoretical; this is our lives”: how erasure impacts health care for transgender people. J. Assoc. Nurses AIDS Care 20, 348–361. doi: 10.1016/j.jana.2009.07.004
Bieschke, K. J., McClanahan, M., Tozer, E., Grzegorek, J. L., and Park, J. (2000). “Programmatic research on the treatment of lesbian, gay, and bisexual clients: the past, the present, and the course for the future,” in Handbook of Counseling and Psychotherapy with Lesbian, Gay, and Bisexual Clients , eds R. M. Perez, K. A. DeBord, and K. J. Bieschke (Washington DC: American Psychological Association), 309–335.
Bieschke, K. J., Paul, P. L., and Blasko, K. A. (2006). “Review of empirical research focused on the experience of lesbian, gay, and bisexual clients in counseling and psychotherapy,” in Handbook of Counseling and Psychotherapy with Lesbian, Gay, Bisexual, and Transgender Clients , eds K. Bieschke, R. Perez, and K. DeBord (Washington DC: American Psychological Association), 293–316.
Bockting, W., Robinson, B., Benner, A., and Scheltema, K. (2004). Patient satisfaction with transgender health services. J. Sex Marital Ther. 30, 277–294. doi: 10.1080/00926230490422467
Bostwick, W. B., Boyd, C. J., Hughes, T. L., and McCabe, S. E. (2010). Sexual orientation and the prevalence of mood and anxiety disorders in the United States. Am. J. Public Health 100, 468–475. doi: 10.2105/AJPH.2008.152942
Bostwick, W. B., Boyd, C. J., Hughes, T. L., West, B. T., and McCabe, S. E. (2014). Discrimination and mental health among lesbian, gay, and bisexual adults in the United States. Am. J. Orthopsychiatry (Am. Psychol. Assoc.) 84, 35–45. doi: 10.1037/h0098851
Brown, L. S. (2006). “The neglect of lesbian, gay, bisexual and transgendered clients,” in Evidence-Based Practices in Mental Health , eds J. C. Norcross, L. E. Beutler, and R. F. Levant (Washington, DC: American Psychological Association), 346–353.
PubMed Abstract | Google Scholar
Cochran, S., Drescher, J., Kismödi, E., Giami, A., García-Moreno, C., Atalla, E., et al. (2014). Proposed declassification of disease categories related to sexual orientation in the international statistical classification of diseases and related health problems (ICD-11). Bull. World Health Organ. Bull. 92, 672–679. doi: 10.2471/BLT.14.135541
Cochran, S. D., and Mays, V. M. (2000). Relation between psychiatric syndromes and behaviourally defined sexual orientation in a sample of the U.S. population. Am. J. Public Health 92, 516–523.
Cochran, S. D., Sullivan, J. G., and Mays, V. M. (2003). Prevalence of mental disorders, psychological distress, and mental health services among lesbian, gay, and bisexual adults in the United States. J. Couns. Clin. Psychol. 71, 53–61.
Cohen-Kettenis, P. T., and Pfäfflin, F. (2010). The DSM diagnostic criteria for gender identity disorder in adolescents and adults. Arch. Sex. Behav. 39, 499–513. doi: 10.1007/s10508-009-9562-y
Coleman, E., Bockting, W., Botzer, M., Cohen - Kettenis, P., DeCuypere, G., Feldman, J., et al. (2012). Standards of care for the health of transsexual, transgender, and gender nonconforming people, 7th version. Int. J. Transgend. 13, 165–232.
D’Augelli, A. R. (1994). “Identity development and sexual orientation: toward a model of lesbian, gay, and bisexual development,” in Human Diversity: Perspectives on People in Context , eds E. J. Trickett, R. J. Watts, and D. Birman (San Francisco, CA: Jossey-Bass).
D’Augelli, A. R., Pilkington, N. W., and Hershberger, S. L. (2002). Incidence and mental health impact of sexual orientation victimization of lesbian, gay, and bisexual youths in high school. School Psychol. Q. 17, 148–167. doi: 10.1521/scpq.17.2.148.20854
Davis, D. (1997). “Towards a model of gay affirmative therapy,” in Pink Therapy: A Guide for Counsellors and Therapists Working with Lesbian, Gay and Bisexual Clients , eds D. Davies and C. Neal (Buckingham: Oxford University Press), 24–40.
Dean, L., Meyer, I. H., Robinson, K., Sell, R. L., Sember, R., Silenzio, V. M. B., et al. (2000). Lesbian, gay, bisexual, and transgender health: findings and concerns. J. Gay Lesbian Med. Assoc. 4, 102–151. doi: 10.1023/A:1009573800168
DeCuypere, G. D., Knudson, G., and Bockting, W. (2010). Response of the world professional association for transgender health to the proposed dsm 5 criteria for gender incongruence. Int. J. Transgend. 12, 119–123. doi: 10.1080/15532739.2010.509214
Drescher, J. (2009). Queer diagnoses: parallels and contrasts in the history of homosexuality. Gender Variance, and the Diagnostic and Statistical Manual. Arch. Sex. Behav. 39, 427–460. doi: 10.1007/s10508-009-9531-5
Drescher, J. (2012). The removal of homosexuality from the dsm: its impact on today’s marriage equality debate. J. Gay Lesbian Mental Health 16, 124–135. doi: 10.1080/19359705.2012.653255
Drescher, J. (2013). Controversies in gender diagnoses. LGBT Health 1, 10–14.
Drescher, J., Cohen-Kettenis, F., and Winter, S. (2012). Minding the body: situating gender identity diagnoses in the ICD-1. Int. Rev. Psychiatry 24, 568–577. doi: 10.3109/09540261.2012.741575
Ehrbar, R. D. (2010). Consensus from differences: lack of professional consensus on the retention of the gender identity disorder diagnosis. Int. J. Transgend. 12, 60–74. doi: 10.1080/15532739.2010.513928
European Union Agency for Fundamental Rights (2014). European LGBT Survey: Main Results. Luxembourg: Publications Office of the European Union.
Feinstein, B. A., Wadsworth, L. P., Davila, J., and Goldfried, M. R. (2014). Do parental acceptance and family support moderate associations between dimensions of minority stress and depressive symptoms among lesbians and gay men? Prof. Psychol. Res. Pract. 45, 239–246. doi: 10.1037/a0035393
Garnets, L., Hancock, K. A., Cochran, S. D., Goodchilds, J., and Peplau, L. A. (1991). Issues in psychotherapy with lesbians and gay men. A Survey of Psychologists. Am. Psychol. 46, 964–972. doi: 10.1037/0003-066X.46.9.964
Global Action for Trans ∗ Equality (2011). It’s Time for Reform. Trans ∗ Health Issues in the International Classification of Diseases. A Report on the GATE Experts Meeting. Available at: http://globaltransaction.files.wordpress.com/2012/05/its-time-for-reform.pdf
Goldfried, M. R. (2001). Integrating lesbian, gay, and bisexual issues into mainstream psychology. Am. Psychol. 56, 977–988. doi: 10.1037/0003-066X.56.11.977
Gómez-Gil, E., Trilla, A., Salamero, M., Godás, T., and Valdés, M. (2009). Sociodemographic, clinical, and psychiatric characteristics of transsexuals from Spain. Arch. Sex. Behav. 38, 378–392. doi: 10.1007/s10508-007-9307-8
Hayes, J., and Erkis, A. (2000). Therapist homophobia, client sexual orientation, and source of client HIV infection as predictors of therapist reactions to clients with HIV. J. Couns. Psychol. 47, 71–78. doi: 10.1037/0022-0167.47.1.71
Hepp, U., Kraemer, B., Schynder, U., Miller, N., and Delsignore, A. (2005). Psychiatric comorbidity in gender identity disorder. J. Psychosom. Res. 58, 259–261. doi: 10.1016/j.jpsychores.2004.08.010
Hershberger, S. L., and D’Augelli, A. R. (1995). The impact of victimization on the mental health and suicidality of lesbian, gay, and bisexual youths. Dev. Psychol. 31, 65–74. doi: 10.1037/0012-1649.31.1.65
Jordan, K. M., and Deluty, R. H. (1995). Clinical Interventions by psychologists with lesbians and gay men. J. Clin. Psychol. 51, 448–456.
Kamens, S. R. (2011). On the proposed sexual and gender identity diagnoses for dsm-5: history and controversies. Hum. Psychol. 39, 37–59. doi: 10.1080/08873267.2011.539935
King, M., Semlyen, J., Killaspy, H., Nazareth, I., and Osborn, D. (2007). A Systematic Review of Research on Counselling and Psychotherapy for Lesbian, Gay, Bisexual & Transgender People. London: British Association for Counselling & Psychotherapy.
King, M., Semlyen, J., Tai, S. S., Killaspy, H., Osborn, D., Popelyuk, D., et al. (2008). A systematic review of mental disorder, suicide, and deliberate self harm in lesbian, gay and bisexual people. BMC Psychiatry 8:70. doi: 10.1186/1471-244X-8-70
Kirschner, S. R. (2013). Diagnosis and its discontents: critical perspectives on psychiatric nosology and the DSM. Fem. Psychol. 23, 10–28. doi: 10.1177/0959353512467963
Lawrence, A. A. (2008). “Gender identity disorders in adults: diagnosis and treatment,” in Handbook of Sexual and Gender Identity Disorders , eds D. L. Rowland and L. Incrocci (New York, NY: Wiley), 423–456.
Lev, A. I. (2004). Transgender Emergence: Therapeutic Guidelines for Working with Gender-Variant People and their Families. New York, NY: Haworth Clinical Practice Press.
Lev, A. I. (2013). Gender dysphoria: two steps forward, one step back. Clin. Soc. Work J. 41, 288–296. doi: 10.1007/s10615-013-0447-0
Liddle, B. J. (1996). Therapist sexual orientation, gender, and counseling practices as they relate to ratings of helpfulness by gay and lesbian clients. J. Couns. Psychol. 43, 394–401. doi: 10.1037/0022-0167.43.4.394
Maguen, S., and Shipherd, J. (2010). Suicide risk among transgender individuals. Psychol. Sex. 1, 34–43. doi: 10.1080/19419891003634430
Meyer, I. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual. (issues)and research evidence. Psychol. Bull. 129, 674–697. doi: 10.1037/0033-2909.129.5.674
Milburn, N. G., Ayala, G., Rice, E., Batterham, P., and Rotheram-Borus, M. J. (2006). Discrimination and exiting homelessness among homeless adolescents. Cultur. Divers Ethn. Minor Psychol. 12, 658–672. doi: 10.1037/1099-9809.12.4.658
Money, J. (1994). The concept of gender identity disorder in childhood and adolescence after 39 years. J. Sex Marital Ther. 20, 163–177. doi: 10.1080/00926239408403428
Mustanski, B., and Liu, R. T. (2013). A longitudinal study of predictors of suicide attempts among lesbian, gay, bisexual, and transgender youth. Arch. Sex. Behav. 42, 437–448. doi: 10.1007/s10508-012-0013-9
Mustanski, B. S., Garofalo, R., and Emerson, E. M. (2010). Mental health disorders, psychological distress, and suicidality in a diverse sample of lesbian, gay, bisexual, and transgender youths. Res. Pract. 100, 2426–2432. doi: 10.2105/AJPH.2009.178319
Nemoto, T., Bodeker, B., and Iwamoto, M. (2011). Social support, exposure to violence, and transphobia: correlates of depression among male-to-female transgender women with a history of sex work. Am. J. Public Health 101, 1980–1988. doi: 10.2105/AJPH.2010.197285
Nuttbrock, L., Hwahng, S., Bockting, W., Rosenblum, A., Mason, M., Macri, M., et al. (2010). Psychiatric impact of gender-related abuse across the life course of male-to-female transgender persons. J. Sex Res. 47, 12–23. doi: 10.1080/00224490903062258
Pachankis, J. E., and Goldfried, M. R. (2004). Clinical issues in working with lesbian, gay, and bisexual clients. Psychotherapy Theor. Res. Pract. Train. 41, 227–246. doi: 10.1037/0033-3204.41.3.227
Pinto, N., and Moleiro, C. (2015). Gender trajectories: transsexual people coming to terms with their gender identities. Prof. Psychol. Res. Pract. 46, 12–20. doi: 10.1037/a0036487
Serano, J. (2007). Whipping Girl. A Transsexual Woman on Sexism and the Scapegoating of Femininity. Berkeley, CA: Seal Press.
Shelton, K., and Delgado-Romero, E. A. (2011). Sexual orientation microaggressions: the experience of lesbian, gay, bisexual, and queer clients in psychotherapy. J. Couns. Psychol. 58, 210–221. doi: 10.1037/a0022251
Shilo, G. R., and Savaya, R. (2012). Mental health of lesbian, gay, and bisexual youth and young adults: differential effects of age, gender, religiosity, and sexual orientation. J. Res. On Adolesc. 22, 310–325.
Shilo, G. Z. (2014). The Impact of Minority Stressors on the Mental and Physical Health of Lesbian. Gay, and Bisexual Youths and Young Adults. Health Soc. Work 39, 161–171.
Simoni, J. M. (1996). Confronting heterosexism in the teaching of psychology. Teach. Psychol. 23, 220–226. doi: 10.1207/s15328023top2304_3
Snapp, S. D., Watson, R. J., Russell, S. T., Diaz, R. M., and Ryan, C. (2015). Social support networks for lgbt young adults: low cost strategies for positive adjustment. Fam. Relations 64, 420–430. doi: 10.1111/fare.12124
Spitzer, R. L. (1981). The diagnostic status of homosexuality in the DSM-III: a reformulation of the issues. Am. J. Psychiatry 138, 210–215. doi: 10.1176/ajp.138.2.210
Sue, D. W. (2010). Microaggressions in Everyday Life: Race, Gender, and Sexual Orientation. Hoboken, N.J: Wiley.
TGEU (2013). TGEU’s Position on the Revision of the ICD z10. Available at: http://www.tgeu.org/sites/default/files/TGEU%20Position%20ICD%20Revision_0.pdf
United Nations (2011). Discriminatory Laws and Practices and Acts of Violence Against Individuals Based on their Sexual Orientation and Gender Identity. Report of the United Nations High Commissioner for Human Rights. Available at: http://www2.ohchr.org/english/bodies/hrcouncil/docs/19session/A.HRC.19.41_English.pdf
Vance, S., Cohen-Kettenis, P. T., Drescher, J., Meyer-Bahlburg, H. F., Pfäfflin, F., and Zucker, K. J. (2010). Opinions about the dsm gender identity disorder diagnosis: results from an international survey administered to organizations concerned with the welfare of transgender people. Int. J. Transgend. 12, 1–14. doi: 10.1080/15532731003749087
Vocks, S., Stahn, C., Loenser, L., and Tegenbauer, U. (2009). Eating and body image disturbances in male-to-female and female-to-male transsexuals. Arch. Sex. Behav. 38, 364–377. doi: 10.1007/s10508-008-9424-z
Winter, S., Chalungsooth, P., Teh, Y., Rojanalert, N., Maneerat, K., Wong, Y., et al. (2009). Transpeople, transprejudice and pathologization: a seven-country factor analysis study. Int. J. Sex. Health 21, 96–118. doi: 10.1080/19317610902922537
World Health Organization (1992). International Statistical Classification of Diseases and Related Health Problems (10th rev.). Geneva: World Health Organization.
World Professional Association for Transgender Health (2013). WPATH ICD-11 Consensus Meeting. Available at: http://www.wpath.org/uploaded_files/140/files/ICD%20Meeting%20Packet-Report-Final-sm.pdf
Keywords : sexual orientation, gender identity, transgender, discrimination, psychopathology, mental health care
Citation: Moleiro C and Pinto N (2015) Sexual orientation and gender identity: review of concepts, controversies and their relation to psychopathology classification systems. Front. Psychol. 6:1511. doi: 10.3389/fpsyg.2015.01511
Received: 29 July 2015; Accepted: 18 September 2015; Published: 01 October 2015.
Reviewed by:
Copyright © 2015 Moleiro and Pinto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY) . The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carla Moleiro, Instituto Universitário de Lisboa ISCTE-IUL, CIS, Avenida das Forças Armadas, 1649-026 Lisbon, Portugal, [email protected]
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Last updated 09/07/24: Online ordering is currently unavailable due to technical issues. We apologise for any delays responding to customers while we resolve this. For further updates please visit our website: https://www.cambridge.org/news-and-insights/technical-incident
We use cookies to distinguish you from other users and to provide you with a better experience on our websites. Close this message to accept cookies or find out how to manage your cookie settings .
Login Alert
- > Journals
- > BJPsych Bulletin
- > Volume 45 Issue 5
- > Sex, gender and gender identity: a re-evaluation of...

Article contents
Homosexuality and conversion therapy, beyond sexual orientation, conversion therapy relating to gender, definitions of sex, gender and gender identity, children and adolescents, suicide, self-harm and current controversies, clinical implications, feminist concerns, conclusions, sex, gender and gender identity: a re-evaluation of the evidence.
Published online by Cambridge University Press: 21 July 2020
- Supplementary materials
- eLetters (5)
In the past decade there has been a rapid increase in gender diversity, particularly in children and young people, with referrals to specialist gender clinics rising. In this article, the evolving terminology around transgender health is considered and the role of psychiatry is explored now that this condition is no longer classified as a mental illness. The concept of conversion therapy with reference to alternative gender identities is examined critically and with reference to psychiatry's historical relationship with conversion therapy for homosexuality. The authors consider the uncertainties that clinicians face when dealing with something that is no longer a disorder nor a mental condition and yet for which medical interventions are frequently sought and in which mental health comorbidities are common.
In 2018 the Royal College of Psychiatrists (RCPsych) issued a position statement to promote good care when dealing with transgender and gender-diverse people that relates to ‘conversion therapy’. 1 In this article we reappraise the phenomenology of gender identity, contrast ‘treatments’ for homosexuality with those for gender non-conformity, analyse the relationship between gender dysphoria and mental disorders with particular reference to the younger cohort of transgender patients, and ask how psychiatrists can address distress related to gender while upholding the central tenet of ‘first do no harm’.
Male homosexuality was outlawed in the UK in 1865 until the Sexual Offences Act 1967 decriminalised sexual acts between men. During that time, homosexuality was shameful, stigmatised and conceptualised as a mental disorder. Psychiatry was instrumental in its treatment, which continued even after the legal change. Reference King 2
Attempts to ‘cure’ same-sex desire included psychotherapy, hormone treatment and various behavioural interventions. These interventions are now considered ‘conversion’ or ‘reparative’ therapy. Reference Haldeman 3 One high-profile failure for such ‘treatments’ was Alan Turing. After being found guilty of gross indecency in 1951, he was prescribed oestrogen, which rendered him impotent and caused gynaecomastia. He died by suicide in 1954. Reference Hodges 4
Conversion therapies lost popularity as evidence emerged of their ineffectiveness, Reference Serovich, Craft, Toviessi, Gangamma, McDowell and Grafsky 5 coupled with more tolerant social attitudes. Homosexuality was removed from the World Health Organization (WHO) ICD-10 classification in 1992. In 2014, the RCPsych published a position statement explicitly rejecting conversion therapy and supporting a ban. 6 Same-sex orientation is regarded as a normal, acceptable variation of human sexuality.
Enshrined in the Equality Act 2010, lesbians and gay men in the UK now enjoy the same civil rights as heterosexuals in terms of healthcare, marriage and raising of children, and equal employment. Although they enjoy equal status and increased visibility in most Western societies, there remain countries and cultures where same-sex practice is taboo or criminal, and where people still seek treatment.
In recent years, increasing links have been forged between lesbian and gay communities and those representing other gender identities. Stonewall describes ‘any person whose gender expression does not conform to conventional ideas of male or female’ as falling under the umbrella term ‘trans’. 7
Definitions have evolved beyond those included in the 1992 ICD-10 under ‘gender identity disorders’, with which psychiatrists might be familiar. 8 Transsexualism was widely understood to mean ‘a desire to live and be accepted as a member of the opposite sex, and an accompanied discomfort of one's anatomic sex’. 8 Underlying mechanisms are poorly understood, although there are similarities and overlaps with both body dysmorphia and body integrity identity disorder. Reference Bray 9 , Reference Ostgathe 10 Sufferers might embark on social and medical intervention to help them ‘pass’ as the opposite sex. Historically, a diagnosis of gender dysphoria would have been required for doctors to intervene in this group. 11
Transgender, however, has become a much broader category ( Fig. 1 ). New terminology reflects a conceptual shift from clinical disorder to personal identity. Reference Reiff Hill 12 Crucially, gender dysphoria is no longer integral to the condition. The World Health Organization has renamed ‘gender identity disorder’ as ‘gender incongruence’ and reclassified it as a ‘condition related to sexual health’ rather than retaining it in the chapter pertaining to ‘mental and behavioural disorders’, Reference Reed, Drescher, Krueger, Atalla, Cochran and First 13 a somewhat discrepant placement, reflecting a political rather than scientific decision-making process.

Fig. 1 A page from The Gender Book Reference Reiff Hill 12 (reproduced with permission of www.thegenderbook.com ).
By contrast, DSM-5 has removed ‘gender identity disorder’, renaming it ‘gender dysphoria’. It is possible to meet the criteria for a diagnosis of gender dysphoria within DSM-5 without experiencing body dysphoria relating to primary or secondary sexual characteristics, 14 and the American Psychiatric Association emphasises that ‘not all transgender people suffer from gender dysphoria’. Reference Drescher and Pula 15
The following is from the 2018 ICD-11: 16
‘Gender incongruence of childhood is characterized by a marked incongruence between an individual's experienced/expressed gender and the assigned sex in prepubertal children. It includes a strong desire to be a different gender than the assigned sex; a strong dislike on the child's part of his or her sexual anatomy or anticipated secondary sex characteristics and/or a strong desire for the primary and/or anticipated secondary sex characteristics that match the experienced gender; and make-believe or fantasy play, toys, games or activities and playmates that are typical of the experienced gender rather than the assigned sex.’
Definitions are inadequate in explaining how anyone experiences the gender of the opposite sex. Without further explanation of ‘toys, games or activities’ that are typical of each sex, this is left to parents, teachers and doctors to determine. The inference might be that gender-congruent behaviours have some objective existence and not fulfilling them might indicate a ‘trans’ identity. Children who do not conform to social norms and expectations come to dislike their sexual characteristics: that embodiment of their gender dissonance.
There is a lack of consensus demonstrated as to the exact nature of the condition. Questions remain for psychiatrists regarding whether gender dysphoria is a normal variation of gender expression, a social construct, a medical disease or a mental illness. If merely a natural variation, it becomes difficult to identify the purpose of or justification for medical intervention.
The RCPsych gives a description within the position statement of ‘treatments for transgender people that aim to suppress or divert their gender identity – i.e. to make them exclusively identify with the sex assigned to them at birth’. 1 Conversion therapy is described as ‘any approach that aims to persuade trans people to accept their sex assigned at birth’. It goes on to include ‘placing barriers [to] medical transition’. Unfortunately, the statement does not define ‘approach’ beyond alluding to psychoanalytic or behavioural talking therapies. Thus, conversion therapy for transgender people appears conflated with that for homosexuality. Furthermore, there is little evidence that it is taking place in the UK. Reference Wright, Candy and King 17 Historically, a diagnosis of gender dysphoria was required before medical intervention; Reference Ostgathe 10 this is a part of standard gatekeeping that is now being criticised as a ‘barrier’ instead of regular safe medical practice. Reference King 2 Now, a self-declaration of being ‘trans’ appears to be indication enough for a patient to expect their doctor provide a range of complex medical treatments, with no evidence of dysphoria being required. Reference Ashley 18
The position statement 1 could also be read as suggesting that full medical transition is an ultimate goal in gender-diverse patients, rather than considering a range of possible goals, which might include limited interventions or reconciliation with one's own (sexed) body. With regard to conversion therapy in children, the statement does not refer to desistance; evidence suggests that the majority of children left alone reconcile their identity with their biological sex; the feelings of 60–80% of children with a formal diagnosis of gender dysphoria remit during adolescence. Reference Ristori and Steensma 19 – Reference Wallien and Cohen-Kettenis 21
Gender theorists propose that all people must have a gender identity; it is not waivable. For those people whose internal identity aligns with their sex, the word cisgender and ‘cis’ terminology are used. Those whose identity is wholly that of the opposite sex are described as transgender or ‘trans’. However, there are other identities for those whose internal sense lies somewhere between or outside a neat fit into either gender-binary category. Fluidity and fluctuation in gender identity is also recognised, with categories such as ‘non-binary’, ‘gender-fluid’, ‘genderqueer’, ‘pangender’ and ‘genderfuck’ all recorded by clinicians at the UK's Gender Identity Development Service (GIDS) for under-18-year-olds. Reference Twist and de Graaf 22 The social networking site Tumblr presently describes over 100 different genders. 23 Without a strong male or female identification, ‘agender’ becomes itself another gender identity.
Some consider gender identity to be fixed and absolute, with some neuroscientists asserting that it develops in utero in the second-trimester brain. Reference Bao and Swaab 24 , Reference Savic, Garcia-Falgueras and Swaab 25 However, there is little to no convincing evidence to support fundamental differences between the brains of females and males. Reference Joel, Berman, Tavor, Wexler, Gaber and Stein 26 If one's ‘internal sense of being a man or a woman’ no longer refers to a ‘man’ or ‘woman’ as defined by biological sex 27 then the definition of gender identity risks becoming circular.
Within current debates, if gender identity becomes uncoupled from both biological sex and gendered socialisation ( Box 1 ), it develops an intangible soul-like quality or ‘essence’. As a pure subjective experience, it may be overwhelming and powerful but is also unverifiable and unfalsifiable. If this identity is held to be a person's innermost core concept of self, then questioning the very existence of gender identity becomes equated with questioning that person's entire sense of being, and consequently risks being considered a threat to the right to exist, or even as a threat to kill. Behaviours such as ‘misgendering’ or ‘dead-naming’ are understood by proponents of gender theory to be destructive, debasing and dehumanising. Reference Freeman 28 This might explain why the prevailing discourse has become as sensitive and at times inflammatory as it has.
Box 1 Sex, gender and gender identity
Humans are sexually dimorphic: there are only two viable gametes and two sexes, whose primary and secondary sexual characteristics determine what role they play in human reproduction. Sex is determined at fertilisation and revealed at birth or, increasingly, in utero . The existence of rare and well-described ‘disorders (differences) of sexual differentiation’ does not negate the fact that sex is binary. The term ‘assigned at birth’ suggests a possibly arbitrary allocation by a health professional, rather than the observed product of sexual reproduction.
Gender describes a social system that varies over time and location and involves shaping of a set of behaviours deemed appropriate for one's sex. It operates at an unconscious level via strong social norms, yet is also rigidly enforced by coercive controls and sometimes violence. Reference Ashley 18 The ‘rules’ exist regardless of how individuals feel about them. Gender can thus be perceived as oppressive and potentially painful to all people of both sexes within patriarchal societies, the dominant form of social structure across most, although not all, of the globe. Feminist theory holds that gender operates as a hierarchy, with men occupying the superior position and women the subordinate. As long as this hierarchy exists, all women are harmed to some extent, whether or not they conform to their sex stereotypes. Reference Ristori and Steensma 19
Gender identity
If sex refers to biology, and gender to socialisation and role, then gender identity may be viewed as the psychological aspect. The American Psychological Association defines it as ‘someone's internal sense of being a man or a woman’. Reference Steensma and Cohen-Kettenis 20 Gender identity is thus distinguished from biological sex and gendered socialisations. Reference Wallien and Cohen-Kettenis 21
Nonetheless, notions of gender identity are still contested and raise some ethical questions for professionals working at the interface of physical and mental disorder. Most psychiatrists reject Cartesian dualism, whereby the mind is something imprisoned inside the body, or the ‘ghost in the machine’. Reference Ryle 29 How should doctors consider the body? We are born as, and die as, a body; we are our bodies. How can someone be born in the wrong body? Many patients bring a ‘wrong’ or ‘wronged’ body to their doctor; these may be traumatised, wounded, diseased or disliked bodies. How should doctors react when someone informs them that, although they inhabit the body of a man, they are in all other respects female? We must deal with all our patients with compassion but also make safe medical decisions when demonstrable material reality is at odds with a patient's subjectivity.
The Gender Identity Development Service (GIDS), Britain's only specialised gender service for children and adolescents and based at the Tavistock Centre, London, has recorded a 25-fold rise in referrals since 2009, most marked in biological girls (‘assigned female at birth’), who make up the majority of referrals presently ( Fig. 2 ). 30

Fig. 2 Referral rates to the Gender Identity Development Service at the Tavistock Centre (Tavistock and Portman NHS Trust) in London between 2009 and 2019. 30
Despite gender dysphoria no longer falling within the remit of mental illness in ICD-11, there is a substantial body of evidence of increased levels of mental illness among adults, usually attributed to societal responses to gender non-conformity or ‘minority stress’. Reference Dhejne, Van Vlerken, Heylens and Arcelus 31 De Vries et al measured psychiatric comorbidity among those referred to a child and adolescent gender clinic in The Netherlands and also found increased rates of depression, anxiety and suicidal ideation in this younger group. Reference de Vries, Doreleijers, Steensma and Cohen-Kettenis 32 However, a potentially worrying picture regarding causes and consequences emerges from more recent research in this young, increasingly natal-female population.
Kaltiala-Heino et al examined referrals to an adolescent gender identity clinic in Finland over a 2-year period, finding high rates of mental health problems, social isolation and bullying ( Fig. 3 ). Reference Kaltiala-Heino, Sumia, Työläjärvi and Lindberg 33 Most bullying pre-dated the onset of gender dysphoria and was unrelated to gender incongruence.

Fig. 3 Referrals to an adolescent gender identity clinic in Finland over a 2-year period (from 2011–2013). Reference Kaltiala-Heino, Sumia, Työläjärvi and Lindberg 33
Similarly, in the UK, Holt et al Reference Holt, Skagerberg and Dunsford 34 found that associated difficulties were common in children and adolescents referred to the GIDS in London ( Fig. 4 ). Same-sex attraction was particularly common among natal females, with only 8.5% of those referred to the GIDS describing themselves as primarily attracted to boys. This raises important questions about current societal acceptance of young lesbians even within youth LGBTQ+ culture. It is possible that at least some gender-non-conforming girls come to believe themselves boys or ‘trans masculine non-binary’ as more acceptable or comfortable explanations for same-sex sexual attraction, Reference Burki 35 a kind of ‘internalised homophobia’. Autism spectrum disorders are consistently overrepresented in referred children and adolescents. Reference van der Miesen, de Vries, Steensma and Hartman 36

Fig. 4 Referrals to the Gender Identity Development Service at the Tavistock Centre (Tavistock and Portman NHS Trust) in London between 1 January 2012 and 31 December 2012. Reference Holt, Skagerberg and Dunsford 34 ASD, autism spectrum disorder.
The RCPsych's position statement acknowledges these elevated rates of mental illness within the transgender population, 1 but appears to attribute them primarily to hostile external responses to those not adhering to gender norms (or sex-specific stereotypes). Reference Arcelus, Claes, Witcomb, Marshall and Bouman 37 , Reference Bouman, Claes, Brewin, Crawford, Millet and Fernandez-Aranda 38 A deeper analysis of mental illness and alternative gender identities is not undertaken, and common causal factors and confounders are not explored. This is worrying, as attempts to explore, formulate and treat coexisting mental illness, including that relating to childhood trauma, might then be considered tantamount to ‘conversion therapy’. Although mental illness is overrepresented in the trans population it is important to note that gender non-conformity itself is not a mental illness or disorder. As there is evidence that many psychiatric disorders persist despite positive affirmation and medical transition, it is puzzling why transition would come to be seen as a key goal rather than other outcomes, such as improved quality of life and reduced morbidity. When the phenomena related to identity disorders and the evidence base are uncertain, it might be wiser for the profession to admit the uncertainties. Taking a supportive, exploratory approach with gender-questioning patients should not be considered conversion therapy.
Transgender support groups have emphasised the risk of suicide. After controlling for coexisting mental health problems, studies show an increased risk of suicidal behaviour and self-harm in the transgender population, although underlying causality has not been convincingly demonstrated. Reference Marshall, Claes, Bouman, Witcomb and Arcelus 39 Then, expressed in the maxim ‘better a live daughter than a dead son’, parents, teachers and doctors are encouraged to affirm unquestioningly the alternative gender for fear of the implied consequences. There is a danger that poor-quality data are being used to support gender affirmation and transition without the strength of evidence that would normally determine pathways of care. One 20-year Swedish longitudinal cohort study showed persisting high levels of psychiatric morbidity, suicidal acts and completed suicide many years after medical transition. Reference Dhejne, Lichtenstein, Boman, Johansson, Långström and Landén 40 These results are not reassuring and might suggest that more complex intrapsychic conflicts remain, unresolved by living as the opposite sex.
Established risk factors for self-harm and suicidal behaviour appear to be age related (younger trans patients are at higher risk) and include comorbid mental health problems, particularly depression, and a history of sexual abuse. Reference Marshall, Claes, Bouman, Witcomb and Arcelus 39 Thus, all new patients of any age warrant thorough assessment and formulation using a biopsychosocial model; the best evidence-informed interventions should be provided. If this is followed by an individual desisting it should not be considered conversion therapy. That term should perhaps be reserved for coercive treatments.
Best psychiatric practice avoids oversimplification of the causes and treatment of suicidal behaviour and self-harm. Preliminary data from a small ‘before and after’ pilot study of the use of puberty blockers at the Tavistock Centre in selected children found a reduction in body image problems in adolescents following a year of puberty suppression. However, positive effects were offset by increases in self-harm and suicidal thoughts. 41 Surprisingly, this unpublished study was deemed a success such that prescribing of puberty blockers was introduced as standard practice and commissioned with scaling up of services. There was no development of alternative psychological approaches, nor were randomised controlled comparisons made.
Evidence suggests that almost 100% of children commencing puberty blockade go on to receive cross-sex hormones. Reference de Vries, Steensma, Doreleijers and Cohen-Kettenis 42 This requires further interrogation to ascertain whether the high figures are due to robust, effective selection and gatekeeping or to a less palatable interpretation that preventing physical and sexual maturation crystallises gender dysphoria as a first step on a cascade of interventions. Reference Wren 43 The GIDS remains under intense scrutiny regarding research criticisms. Reference Cohen and Barnes 44 Although in the early 2000s it was criticised for being too conservative and not offering puberty blockers, there appears to have been a volte-face made in response to external pressure, Reference Giordano 45 without the publishing of robust data showing that this intervention is effective and safe.
Puberty blockers are known to affect bone and, possibly, brain development. They put users at risk of developing osteoporosis Reference Klink, Caris, Heijboer, van Trotsenburg and Rotteveel 46 and are associated with reductions in expected IQ. Reference Schneider, Spritzer, Soll, Fontanari, Carneiro and Tovar-Moll 47 They are described as ‘buying time’ for adolescents to make up their mind about whether to proceed with transition. Long-term effects are not known, but infertility appears inevitable when cross-sex hormones are introduced shortly after puberty blockers. Reference Johnson and Finlayson 48 Loss of sexual maturation will also be associated with lack of adult sexual function, although it is unlikely that a pre-pubertal child can truly understand this side-effect at the time of consent.
Those seeking transition are a vulnerable population who suffer from high levels of suicidality, psychiatric morbidity and associated difficulties. Medical and surgical transition is sought to relieve these psychiatric symptoms. Plausibly, there is an initial reduction in distress following transition, although no controlled trials exist. Therefore, the long-term outcome of medical and surgical transition in terms of mortality and quality of life remains unknown. No long-term comparative studies exist that satisfactorily demonstrate that hormonal and surgical interventions are superior to a biopsychosocial formulation with evidence-based therapy in reducing psychological distress, body dysphoria and underlying mental illness.
It is unclear what the role of psychiatry is in the assessment and treatment of gender dysphoria, now that it is no longer considered a diagnosable mental illness, and whether there is still a place for a routine psychosocial assessment. It could be argued that patients should be deterred from gender intervention pathways while comorbid mental illness is treated ( Fig. 5 ). Without long-term follow-up data, it is not possible to identify those who might reconcile with their sex and those who might come to deeply regret their medical and/or surgical transition. Moreover, it is not transparent where ultimate and legal responsibility for decision-making lies – with the patient, parents (if the patient is a child), psychologist, endocrinologist, surgeon or psychiatrist.

Fig. 5 Are these scenarios examples of good clinical practice or conversion therapy?
Psychiatrists understand that human development is necessary, but not always comfortable. Puberty, although a normal physiological process, is associated with particularly high levels of psychological and bodily discomfort. Psychiatrists’ role is to journey with patients as change is navigated and to provide support through sharing uncertainty and difficult decision-making. But in the current climate, psychiatrists may be unsure whether addressing psychological and social antecedents will lead to accusations of conversion therapy. Attempts to reconcile a sufferer's discomfort with their actual body would be good practice in other conditions involving body image disturbance, such as anorexia nervosa.
The magnitude of any benefits of medical and surgical transition is not clear. Follow-up studies are sparse, and with the new cohort of adolescents, clinicians step even further into the unknown. Reference Richards, Maxwell and McCune 49 These young people are not comparable to adult, mainly male-to-female, research participants on whom existing empirical clinical guidelines were based. Doctors are now questioning the wisdom of gender-affirmation treatment of children and young people, citing poor diagnostic certainty and low-quality evidence. Reference Laidlaw, Van Meter, Hruz, Van Mol and Malone 50 A recent review of evidence for the use of gender-affirming hormones for children and adolescents states that these drugs ‘can cause substantial harms, including death’ and concludes ‘the current evidence base does not support informed decision making and safe practice’. Reference Heneghan 51
Among a plethora of online videos by teenagers proudly displaying their mastectomy scars a worrying increase in detransitioner testimonies can now be found 52 ( Fig. 6 ). These are mainly young women who have rejected their trans identities and are reconciling with their birth sex.

Fig. 6 Reasons given for detransitioning in a female detransition and re-identification survey run between 16 and 30 August 2016 and shared through online social networking sites. 52
In theory, universal human rights should not pit disadvantaged groups against one another, but in practice, disputes occur. Women's rights activists point to persistent global inequalities, sex discrimination and violence against women and girls. They are concerned that ignoring sex as a reality risks no longer being able to name, measure and ameliorate sex-based harms. Endorsing old sex and gender stereotypes in an attempt to validate young patients may inadvertently shore up outdated notions of how men and women should look and behave. There is no reason to believe that women have an innate love of pink and wearing high heels and find map-reading difficult, any more than men have a natural leaning towards blue and playing football and make excellent leaders.
Inherent in the notion of ‘gender identity’ is that there already exists a specific subjective experience of being a man or a woman. However, there cannot be a significant intrinsic experiential difference between male and female human beings when we cannot know what those differences are. One cannot possibly know how it feels to be anything other than oneself. Medicine may be in danger of reinforcing social norms and reifying a concept that is impossible to define over and above material biological reality. At present, many health, social, educational and legal policies are being adapted to give gender primacy over sex. 53 – 57
Language that confuses or conflates sex and gender identity, while appearing inclusive, might have the unintended consequence of closing down the means to understand complexity and respond appropriately to patients’ emotional and material reality. The medical profession must be compassionate, accept differences and fight for those who are marginalised and discriminated against.
However, viewing transgender as a fixed or stable entity, rather than a state of mind with multiple causative factors, closes down opportunities for doctors and patients to explore the meaning of any discomfort. Being gender non-conforming, or wishing to opt out of gender altogether, is not only not indicative of mental disorder – it is, in many ways, an entirely rational response to present capitalist reliance on rigid gender norms and roles. However, when multiple medical interventions are required on an otherwise healthy body or doctors are expected to deny the concept of sex or the sexed body, the situation becomes less coherent. The notion of conversion therapy for those seeing themselves as transgender relies on another binary – that of ‘cisgender’ and ‘transgender’ – being set, closed, biologically anchored categories without overlap, rather than a more plausible hypothesis that one's gender identity is flexible, informed by one's culture, personality, personal preferences and social milieu.
The push for early bodily modification and hormones by some transgender patients is a cause for concern. New services, modelled on commissioning guidance from NHS England for adults of 17 years and above, will allow for self-referral, preclude psychological formulation or therapeutic intervention as standard practice, and recommend hormonal intervention after two appointments. 58 This will further scale up hormonal and surgical interventions in young patients, who will miss out on pubertal development and necessary mental health treatment in their quest for interventions that may harm and that they may later regret.
In the rapidly moving and politicised debate, psychiatrists look to the RCPsych for guidance. Those providing and interpreting the scanty evidence from published research need to be independent and impartial, using best-quality measures rather than ideology. It is confusing to liken open-minded working with young patients as they figure out who they are to conversion therapy. Holding an empathic neutral middle ground, which might or might not include medical transition, should not be equated with this. Psychiatrists need to feel empowered to explore the meaning of identity with their patients, treat coexisting mental illness and employ a trauma-informed model of care when appropriate.
The General Medical Council's Good Medical Practice demands of clinicians compassion, shared decision-making and safeguarding of young people's open futures. 59 The counterargument to unquestioning gender affirmation is that the process of medical transition may itself prove to be another form of conversion therapy, creating a new cohort of life-long patients dependent on medical services and turning at least some lesbian and gay young people into simulacra of straight members of the opposite sex. Psychiatry sits on this knife-edge: running the risk of being accused of transphobia or, alternatively, remaining silent throughout this uncontrolled experiment. Respectful debate, careful research and measurement of outcomes are always required.
About the authors
Lucy Griffin , MBBS, BSc, MRCPsych, is a consultant psychiatrist at The Priory Hospital Bristol, UK. Katie Clyde , MBChB, MRCPsych, DGM, is a consultant psychiatrist with Southern Health NHS Foundation Trust, Hampshire, UK. Richard Byng , MB BChir, MRCGP, MPH, PhD, is a general practitioner and Professor of Primary Care Research at the University of Plymouth, UK. Susan Bewley , MD, FRCOG, MA, is Professor (Emeritus) of Obstetrics and Women's Health, Department of Women & Children's Health, King's College London, UK.
Acknowledgements
We consulted a trans woman and a detransitioner for this article. We thank them for their input.
Author contributions
L.G.: undertook a search and analysis of the literature, and conceived and wrote the paper. K.C.: undertook a search and analysis of the literature, and contributed to the drafting of the paper. R.B.: participated in the conception and evolution of the analysis, critically reviewing the paper and suggesting amendments incorporated into the final paper. S.B.: participated in the conception and evolution of the analysis, critically reviewing the paper and suggesting amendments incorporated into the final paper.
Declaration of interest
ICMJE forms are in the supplementary material, available online at https://doi.org/10.1192/bjb.2020.73 .

Fig. 1 A page from The Gender Book 12 (reproduced with permission of www.thegenderbook.com ).

Fig. 3 Referrals to an adolescent gender identity clinic in Finland over a 2-year period (from 2011–2013). 33

Fig. 4 Referrals to the Gender Identity Development Service at the Tavistock Centre (Tavistock and Portman NHS Trust) in London between 1 January 2012 and 31 December 2012. 34 ASD, autism spectrum disorder.

Griffin et al. supplementary material
Griffin et al. supplementary material 1
Griffin et al. supplementary material 2
Griffin et al. supplementary material 3
Griffin et al. supplementary material 4
This article has been cited by the following publications. This list is generated based on data provided by Crossref .
- Google Scholar
View all Google Scholar citations for this article.
Save article to Kindle
To save this article to your Kindle, first ensure [email protected] is added to your Approved Personal Document E-mail List under your Personal Document Settings on the Manage Your Content and Devices page of your Amazon account. Then enter the ‘name’ part of your Kindle email address below. Find out more about saving to your Kindle .
Note you can select to save to either the @free.kindle.com or @kindle.com variations. ‘@free.kindle.com’ emails are free but can only be saved to your device when it is connected to wi-fi. ‘@kindle.com’ emails can be delivered even when you are not connected to wi-fi, but note that service fees apply.
Find out more about the Kindle Personal Document Service.
- Volume 45, Issue 5
- Lucy Griffin (a1) , Katie Clyde (a2) , Richard Byng (a3) and Susan Bewley (a4)
- DOI: https://doi.org/10.1192/bjb.2020.73
Save article to Dropbox
To save this article to your Dropbox account, please select one or more formats and confirm that you agree to abide by our usage policies. If this is the first time you used this feature, you will be asked to authorise Cambridge Core to connect with your Dropbox account. Find out more about saving content to Dropbox .
Save article to Google Drive
To save this article to your Google Drive account, please select one or more formats and confirm that you agree to abide by our usage policies. If this is the first time you used this feature, you will be asked to authorise Cambridge Core to connect with your Google Drive account. Find out more about saving content to Google Drive .
Reply to: Submit a response
- No HTML tags allowed - Web page URLs will display as text only - Lines and paragraphs break automatically - Attachments, images or tables are not permitted
Your details
Your email address will be used in order to notify you when your comment has been reviewed by the moderator and in case the author(s) of the article or the moderator need to contact you directly.
You have entered the maximum number of contributors
Conflicting interests.
Please list any fees and grants from, employment by, consultancy for, shared ownership in or any close relationship with, at any time over the preceding 36 months, any organisation whose interests may be affected by the publication of the response. Please also list any non-financial associations or interests (personal, professional, political, institutional, religious or other) that a reasonable reader would want to know about in relation to the submitted work. This pertains to all the authors of the piece, their spouses or partners.
- Share full article
Advertisement
Supported by
Guest Essay
I’m a Psychiatrist. Here’s How I Talk to Transgender Youth and Their Families About Gender Identity.

By Jack Turban
Dr. Turban is a child and adolescent psychiatrist.
Talking about gender understandably brings up a lot of feelings. We’re having heated discussions around bathroom bills , gender-affirming medical care and transgender athletes . Politicians opine about the dangers of “ gender ideology ” in schools and children being “ mutilated and sterilized .” Others have decried the rise in adolescents identifying as transgender and nonbinary as a “ social contagion ,” likening gender diversity to a disease.
It’s easy to get overwhelmed and want to run away from these discussions altogether. But engaging with questions around gender identity with nuance is essential as national debates escalate. Gender identity, for all of us, isn’t simple or binary; it’s neither just biology nor just a social construct. There’s dramatic variability in how people experience gender identity beyond cisgender (people who identify as the sex they are assigned at birth) and transgender or male and female. Younger people especially are opening up about gender and thinking about this part of their identities with more nuance and clarity than older generations typically have.
In my clinical practice, I often help parents talk to their trans children about gender identity using a three-part framework that I’ve found allows people to better understand one another. Perhaps it can help all of us engage with today’s political debates with more understanding and even help us — regardless of our gender identities — understand ourselves on a deeper level.
The most basic part of gender identity is what I call our transcendent sense of gender. In a way that goes beyond language, people often just feel male or female, and some more strongly than others. This can manifest in different ways. Some of my young patients draw themselves as a certain gender and have a “wow, this is me” feeling. Others have strong positive feelings when people use certain pronouns for them, or strong negative feelings when people use other pronouns. As is the case with many emotions, it’s hard to describe this transcendent feeling in words. But it is the foundation of our gender identity, the scaffolding we’re born with. Research , including studies focused on twins , suggests these transcendent gender feelings have a strong innate biological basis.
The next part of our gender identity is the social domain. As we move through life, we build on the biology of gender identity with language and social experience, influenced by everything from the TV shows we watch to how we interact with classmates and our families. Maybe you were raised to think women are nurturing, passive and creative while men are assertive and strong, or that dolls are for girls and football is for boys. What my work has taught me is that very few of us actually relate 100 percent to male or female social categories. Some people may love ballet and wrestling. Or they may enjoy pickup trucks and knitting. To make it even more complicated, these feelings can evolve over time — the way an 18-year-old college student thinks about her womanhood is likely different from how she thinks about it when she becomes a 40-year-old mother of three.
The social aspect can cut both ways. For some people, rejecting gender role stereotypes is even more vital to their gender identity than adhering to them. I’ve had patients, for example, who hate the expectations placed on women in American society. They began using they/them pronouns as a way to express rejection of those expectations. However, they loved their birth names and bodies and had no interest in gender-affirming medical interventions. There are others who identify strongly as cisgender and express their rejection of gender stereotypes in other ways. The existence of one type of person does not invalidate the experience of another.
We are having trouble retrieving the article content.
Please enable JavaScript in your browser settings.
Thank you for your patience while we verify access. If you are in Reader mode please exit and log into your Times account, or subscribe for all of The Times.
Thank you for your patience while we verify access.
Already a subscriber? Log in .
Want all of The Times? Subscribe .
IMAGES
VIDEO
COMMENTS
Gender identity. If sex refers to biology, and gender to socialisation and role, then gender identity may be viewed as the psychological aspect. The American Psychological Association defines it as 'someone's internal sense of being a man or a woman'. 20 Gender identity is thus distinguished from biological sex and gendered socialisations. 21.
A Global Perspective on Gender Roles and Identity. Among the social determinants that affect the health and well-being of young people throughout the world, gender is a pivotal influence, with both subtle and overt, immediate as well as longer term influences on adolescent development, resources and opportunities, and ultimately, adolescent and ...
The concept of gender identity evolved over time to include those people who do not identify either as female or male: a "person's self concept of their gender (regardless of their biological sex) is called their gender identity" (Lev, 2004, p. 397). The American Psychological Association (2009a, p. 28) described it as: "the person's ...
1 |. INTRODUCTION. Gender identity and sexual orientation are fundamental independent characteristics of an individual's sexual identity. 1 Gender identity refers to a person's innermost concept of self as male, female or something else and can be the same or different from one's physical sex. 2 Sexual orientation refers to an enduring pattern of emotional, romantic and/or sexual ...
The 21st century has seen shifts in social and scientific understandings of gender and sexuality in the United States. From the legitimization of same-sex marriage to the heightened visibility of transgender identities, nonbinary gender, and forms of intimate diversity such as asexuality, kink, and polyamory, core cultural and scientific assumptions about gender and sexuality have been challenged.
Larger scale and higher quality longitudinal research on gender identity development in children is needed. Some externally funded longitudinal studies are currently in progress internationally. Findings from these studies will enhance understanding of outcomes over time in relation to gender identi …
Gender identity encompasses children's appraisals of compatibility with, and motivation to fit in with, gender collectives; it is a multidimensional construct. Five dimensions of gender identity are considered in depth: felt same-gender typicality, felt other-gender typicality, gender contentedness, felt pressure for gender conformity, and ...
The evidence base informing best practice for the care of children and young people (CYP) (<18 years) with gender dysphoria (GD) is continually developing (Coleman et al., 2012; Hembree et al., 2017).In addition to increases in referral rates to specialised gender services in recent years (Giovanardi, 2017), there also appear to be changes in referral patterns observed both in the UK (de Graaf ...
28 May 2024. Heed lessons from past studies involving transgender people: first, do no harm. Decades of neuroscientific work have focused on exploring a biological basis for transgender identity ...
Traditional models of gender identity development for individuals who do not identify with their assigned birth sex have generally treated medical intervention as normative, and non-binary identification as relatively rare. However, changing demographics within gender diverse populations have highlighted the need for an updated framework of gender identity development. To address this gap in ...
In the early 2000s, researchers shifted from focusing solely on binary gender identity labels (i.e., boy vs. girl) to include self-perceived typicality of one's gender, experiencing pressure from others to conform to gender stereotypes, or the idea that one's own gender is superior to another gender (Egan & Perry, Citation 2001).
Gender identity is a collection of thoughts and feelings about one's own gender, which may or may not correspond to the sex assigned at birth 1,2,3,4,5.This multifaceted, subjective sense of ...
Increasing numbers of children and adolescents are being referred to gender services for gender-related concerns. Various instruments are used with these patients in clinical care, but their clinical validity, strengths, and limitations have not been systematically reviewed. In this systematic review, we searched MEDLINE, PubMed, and PsycINFO databases for available tools that assess gender ...
In addition, for many of our respondents, gender identity was made up of overlapping factors, including the relationship between gender and transgender identities. These findings challenge researchers to reconsider how identity is understood as and through data. Drawing from critical data studies, feminist and queer digital media studies, and ...
Gender socialization processes, in line with the social role theory (Eagly and Steffen, 1986) inculcate gender roles throughout childhood (Lippa, 2005), that are strengthened at mature ages by the ...
Background Despite greater acceptance of sexual and gender diversity and the scientific consensus that same-gender attraction, creative gender expression, and transness are not mental illnesses, LGBTQI2+ persons are still commonly told that they can or should change their sexual orientation, gender identity, or gender expression (SOGIE). The aim of this study was to describe the prevalence of ...
Violence based on sexual orientation, gender identity or gender expression is present in our society and within the university community [1,2,3].Numerous international studies have shown that the lesbian, gay, transgender, queer and intersex (LGBTQI+) community have more risk and probabilities to suffer sexual discrimination or harassment during their university trajectory [2, 3].
The concept of gender identity evolved over time to include those people who do not identify either as female or male: a "person's self concept of their gender (regardless of their biological sex) is called their gender identity" (Lev, 2004, p. 397). The American Psychological Association (2009a, p. 28) described it as: "the person's ...
The Multi-Gender Identity Questionnaire (Multi-GIQ; Joel et al., Citation 2014) is an alternative to the BSRI. Similar to the BSRI, Multi-GIQ defines femininity and masculinity as two independent dimensions. However, instead of measuring personality traits, the Multi-GIQ items assess self-identification with femininity and masculinity on levels ...
Understandings of sexual and gender identity have expanded beyond traditional binaries, yet we know little about adolescents' appropriation of identity labels across diverse communities. In a mixed-methods study of adolescents recruited from lesbian, gay, bisexual, transgender, and queer (LGBTQ+) spaces in communities differing in support of ...
Bornstein, a trans woman who finds gender deeply problematic, sums up this resistance nicely in her 1995 book title, Gender Outlaw: On Men, Women and the Rest of Us1. It is commonly argued that biological differences between males and females determine gender by causing enduring differences in capabilities and dispositions.
Box 1 Sex, gender and gender identity. Sex. Humans are sexually dimorphic: there are only two viable gametes and two sexes, whose primary and secondary sexual characteristics determine what role they play in human reproduction. Sex is determined at fertilisation and revealed at birth or, increasingly, in utero.
gender quotas (e.g., Beaman et al., 2009, Beath, Christia, Enikolopov, 2012) may need to account for the intersectionality of gender with social identity, and possibly allocate gender quotas based on the socio-economic background of women. As part of the large body of empirical evidence on gender unequal treatment in South Asia2,
Dr. Turban is a child and adolescent psychiatrist. Talking about gender understandably brings up a lot of feelings. We're having heated discussions around bathroom bills, gender-affirming ...