Building a Continuum of Care: Case Studies in HER2-Positive Breast Cancer
Check back on December 18th, 2023, 12:00AM to complete this activity

All Credits Available
AMA PRA Category 1 Credit(s)™
ANCC Contact Hour(s)
Pharmacists
Knowledge-based ACPE
IPCE 1.00 Interprofessional Continuing Education (IPCE) credit
Target Audience and Goal Statement
This activity is intended for oncologists, obstetricians & gynecologists, pathologists, surgeons, oncology nurses and nurse practitioners (NPs), oncology pharmacists, and other members of the oncology care team.
The goal of this activity is for learners to be better able to select the most optimal anti-HER2 treatments for patients with HER2-positive breast cancer at every stage of care.
Upon completion of this activity, participants will:
- Clinical data associated with emerging anti-HER2 regimens for patients with HER2-positive breast cancer
- Selecting the most optimal anti-HER2 treatment regimens for patients with HER2-positive breast cancer
- Managing adverse events (AEs) that may present with the use of anti-HER2 therapies for the treatment of HER2-positive breast cancer
- Use the interprofessional team to manage the AEs associated with anti-HER2 therapies for treatment of HER2-positive breast cancer
Disclosures
Medscape, LLC requires every individual in a position to control educational content to disclose all financial relationships with ineligible companies that have occurred within the past 24 months. Ineligible companies are organizations whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
All relevant financial relationships for anyone with the ability to control the content of this educational activity are listed below and have been mitigated. Others involved in the planning of this activity have no relevant financial relationships.

Sara A. Hurvitz, MD, FACP
Professor of Medicine Head, Division of Hematology and Oncology Senior Vice President, Clinical Research Division Department of Medicine, UW Medicine Fred Hutchinson Cancer Center Seattle, Washington, United States

Joyce A. O’Shaughnessy, MD
Celebrating Women Chair in Breast Cancer Research Baylor University Medical Center Chair, Breast Cancer Committee Breast Cancer Research Program Texas Oncology Sarah Cannon Research Institute Dallas, Texas

Sara M. Tolaney, MD, MPH
Associate Professor of Medicine Harvard Medical School Chief, Division of Breast Oncology Dana-Farber Cancer Institute Boston, Massachusetts
Amy Furedy, RN, OCN
Medical Education Director, Medscape, LLC
Compliance Reviewer/Nurse Planner
Maria morales, msn, rn, clnc.
Associate Director, Accreditation and Compliance, Medscape, LLC
Peer Reviewer
This activity has been peer reviewed and the reviewer has no relevant financial relationships.
Accreditation Statements
In support of improving patient care, Medscape, LLC is jointly accredited with commendation by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC), to provide continuing education for the healthcare team.

This activity was planned by and for the healthcare team, and learners will receive 1.00 Interprofessional Continuing Education (IPCE) credit for learning and change.
For Physicians
Medscape, LLC designates this live activity for a maximum of 1.0 AMA PRA Category 1 Credit(s)™ . Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Contact This Provider
Awarded 1.0 contact hour(s) of nursing continuing professional development for RNs and APNs; 1.00 contact hours are in the area of pharmacology.
For Pharmacists
Medscape designates this continuing education activity for 1.0 contact hour(s) (0.100 CEUs) (Universal Activity Number: JA0007105-0000-23-416-L01-P).
For questions regarding the content of this activity, contact the accredited provider for this CME/CE activity noted above. For technical assistance, contact [email protected] .
Instructions for Participation & Credit
There are no fees for participating in or receiving credit for this online educational activity. For information on applicability and acceptance of continuing education credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within the time designated on the title page; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity online during the valid credit period that is noted on the title page. To receive AMA PRA Category 1 Credit ™, you must receive a minimum score of 75% on the post-test.
Follow these steps to earn CME/CE credit*:
- Read about the target audience, learning objectives, and author disclosures.
- Study the educational content online or print it out.
- Online, choose the best answer to each test question. To receive a certificate, you must receive a passing score as designated at the top of the test. We encourage you to complete the Activity Evaluation to provide feedback for future programming.
You may now view or print the certificate from your CME/CE Tracker. You may print the certificate, but you cannot alter it. Credits will be tallied in your CME/CE Tracker and archived for 6 years; at any point within this time period, you can print out the tally as well as the certificates from the CME/CE Tracker.
*The credit that you receive is based on your user profile.
Check back on a future date to complete this activity
Supported by an independent educational grant from Seagen, Inc.
THIS ACTIVITY HAS EXPIRED FOR CREDIT
Medscape Education makes these downloadable slides available solely for non-commercial use by you as a reference tool. You may not use these slides for any commercial purpose or provide these slides to any third party for such party’s use for any commercial purpose. Please refer to the Medscape Terms of Use for additional details.
Activity Transcript
Abbreviations, webmd network.
Ohio State nav bar
The Ohio State University
- BuckeyeLink
- Find People
- Search Ohio State
Pathophysiology
Normal physiology of the human breast.
Prior to sexual maturity, male and female breasts are structurally and functionally similar; they are both comprised of small immature nipples, fatty and fibrous tissue and several duct-like arrangements beneath the areola.
When puberty is underway in males and females, this is where the major structural development occurs. Male breasts remain unchanged due to the lack of high levels of estrogen and progesterone. Females, on the other hand, have significant changes occur due to an assortment of hormones (estrogen, growth hormone, insulin-like growth factor-1, progesterone, and prolactin) (p.739) that cause the female breast to develop into a lactating system.
The mature female breast’s foundational unit is the lobe (each breast contains 15-20) a system of ducts which is comprised of and supported by Cooper ligaments. Each lobe is made up of 20-40 lobules (glands that produce milk). The lobules contain alveolar cells, which are complicated spaces lined with epithelial cells that secrete milk and sub-epithelial cells that contract, passing milk into the arrangement of ducts that leads to the nipple (p. 739).
The lobes and lobules are enclosed and separated by muscle strands and adipose connective tissue which varies in amount depending on weight, genetics, endocrine factors and contributes to the diversity of breast size and shape.
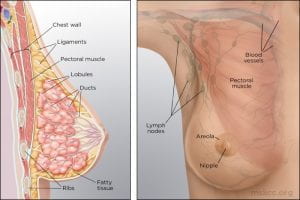
(Memorial Sloan Kettering Cancer Center)
During the reproductive years, breast tissue undergoes cyclic changes in response to hormonal changes of the menstrual cycle. After menopause, adipose deposits and connective tissue increases, glandular breast tissue becomes involuted, and breasts are reduced in size and form. Due to elevated aromatase (decreases circulating estrogen) there can be an increase in white adipose tissue inflammation (p.740).
The function of the female breast is primarily to provide a source of nourishment for the newborn; however, breasts are also a source of pleasurable sexual sensation and in Western cultures have become a sexual symbol (p.741).
(McCance, K. L., & Heuther, S. E. (2019). Pathophysiology: The biological basis for disease in adults and children (8th ed., pp.739-741). St. Louis, MO: Mosby.)
Pathophysiology of Breast Cancer
Except for skin cancer, breast cancer is the most common cancer in American women. Most breast cancer occurs in women older than 50 years. The major risk factors for breast cancer are classified as reproductive, such as nulliparity and pregnancy-associated breast cancer; familial, such as inherited gene syndromes; and environmental and lifestyle, such as hormonal factors and radiation exposure. Some examples of known carcinogenic agents with sufficient evidence in humans that contribute to the development of breast cancer are alcoholic beverages, diethylstilbestrol, estrogen-progestogen contraceptives, estrogen-progestogen menopausal therapy, X-radiation and γ-radiation (Rote, 2019). Other important factors are delayed involution of the mammary gland and increased breast density.
Overall, lifetime risk of breast cancer is reduced in parous women compared to nulliparous women, but pregnancy must occur at a young age. The influence of pregnancy on the risk of cancer also depends on family history, lactation postpartum, and overall parity. Breast gland involution after pregnancy and lactation uses some of the same tissue remodeling pathways activated during wound healing. The presence of macrophages in the involuting mammary gland contributes to carcinogenesis.
Most breast cancers are adenocarcinomas and first arise from the ductal/lobular epithelium as carcinoma in situ. Carcinoma in situ is an early-stage, noninvasive, proliferation of epithelial cells that is confined to the ducts and lobules, by the basement membrane. About 84% of all in situ disease is ductal carcinoma in situ (DCIS); the remainder is mostly lobular carcinoma in situ (LCIS) disease. Ductal carcinoma in situ (DCIS) refers to a heterogenous group of proliferative lesions limited to ducts and lobules without invasion to the basement membrane. DCIS occurs predominantly in women but can also occur in men. DCIS has a wide spectrum of risk for invasive cancers. Preinvasive lesions do not invariably progress to invasive malignancy. Lobular carcinoma in situ (LCIS) originates from the terminal duct-lobular unit. Unlike DCIS, LCIS has a uniform appearance; thus, the lobular structure is preserved. The cells grow in non-cohesive clusters, typically because of a loss of the tumor-suppressive adhesion protein E-cadherin . Also, unlike DCIS, LCIS is found as an incidental lesion from a biopsy and not mammography, is more likely to be present bilaterally.
(Winslow, 2012)
Breast cancer is a heterogeneous disease with diverse, molecular, genetic, phenotypic, and pathologic changes. Tumor heterogeneity results from the genetic, epigenetic, and microenvironmental influences (selective pressure) that tumor cells undergo during cancer progression. Cellular subpopulations from different sections of the same tumor vary in many ways including growth rate, immunogenicity, ability to metastasize, and drug response, demonstrating significant heterogeneity. The biological attributes of a tumor as a whole are strongly influenced by its subpopulation of cells with cellular populations communicating through paracrine or contact-dependent signaling (juxtacrine) from ligands and mediated from components of the microenvironment such as blood vessels, immune cells, and fibroblasts.
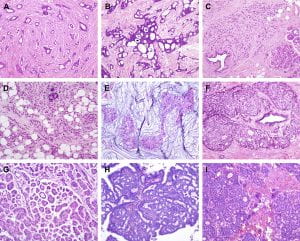
Figure 1. Histological special types of breast cancer preferentially oestrogen receptor positive. (A) Tubular carcinoma, (B) cribriform carcinoma, (C) classic invasive lobular carcinoma, (D) pleomorphic invasive lobular carcinoma, (E) mucinous carcinoma, (F) neuroendocrine carcinoma, (G) micropapillary carcinoma, (H) papillary carcinoma, (I) low grade invasive ductal carcinoma with osteoclast-like giant cells. (Weigelt, Geyer, & Reis-Filho, 2010)
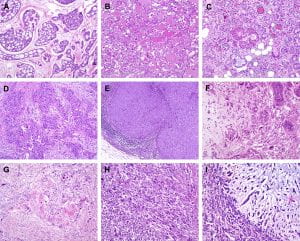
Figure 2. Histological special types of breast cancer preferentially oestrogen receptor negative. (A) Adenoid cystic carcinoma, (B) secretory carcinoma, (C) acinic-cell carcinoma, (D) apocrine carcinoma, (E) medullary carcinoma, (F) metaplastic carcinoma with heterologous elements, (G) metaplastic carcinoma with squamous metaplasia, (H) metaplastic spindle cell carcinoma, (I) metaplastic matrix-producing carcinoma. (Weigelt, Geyer, & Reis-Filho, 2010)
Gene expression profiling studies have identified major subtypes classified as luminal A, luminal B, HER2+, basal-like, Claudin-low, and normal breast. These subtypes have different prognoses and responses to therapy. Tumors can be stratified with gene expression profiles such as Oncotype Dx, Prosigna, and MammaPrint on the basis of genetic profiles. This information helps personalize breast cancer treatment and determine which women need aggressive systemic treatment for high-risk cancers versus close surveillance for indolent tumors.
Many models of breast carcinogenesis have been suggested and the expanding themes include (1) gene addiction, (2) phenotype plasticity, (3) cancer stem cells, (4) hormonal outcomes affecting cell turnover of mammary epithelium, stem cells, extracellular matrix, and immune function.
Cancer gene addiction includes oncogene addiction, whereby these driver genes play key roles in breast cancer development and progression. In non-oncogene addiction, these genes may not initiate cancer but play roles in cancer development and progression. Examples of key driver genes include HER2 and MYC, and examples of tumor-suppressor genes include TP53, BRCA1, and BRCA2. Once a founding tumor clone is established, genomic instability may assist through the establishment of other subclones and contribute to both tumor progression and therapy resistance.
Phenotypic plasticity is exemplified by a distinctive phenotype called epithelial-to-mesenchymal transition (EMT) . EMT is involved in the generation of tissues and organs during embryogenesis, is essential for driving tissue plasticity during development, and is hijacked during cancer progression. The EMT-associated programming is involved in many cancer cell characteristics, including suppression of cell death or apoptosis and senescence. It is reactivated during wound healing and is resistant to chemotherapy and radiation therapy. Remodeling or reprogramming of the breast during post-pregnancy involution is important because it involves inflammatory and “wound healing-like” tissue reactions known as reactive stroma or inflammatory stroma . The reactive stroma releases various signals and interleukins that affect nearby carcinoma cells, inducing these cells to activate their previously silent EMT programs. The activation is typically reversible (i.e., plasticity), and those EMT programs may revert through mesenchymal-epithelial (MET) to the previous phenotypic state before the induction of the EMT program. Reactive stroma increases the risk for tumor invasion and may facilitate the transition of carcinoma in situ to invasive carcinoma. Activation of an EMT program during cancer development often requires signaling between cancer cells and neighboring stromal cells. In advanced primary carcinomas, cancer cells recruit a variety of cell types into the surrounding stroma. Overall, increasing evidence suggests that interactions of cancer cells with adjacent tumor-associated stromal cells induce malignant phenotypes.
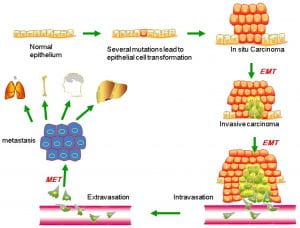
Figure 3. Putative EMT and MET in breast cancer progression. Normal epithelial cells undergo a series of transformational changes to become malignant tumor cells. Clonal proliferation of malignant cells gives rise to invasive carcinoma. Some of these cells undergo EMT and enter into the neighboring blood vessels or lymphatic vessels. These cells may remain in the circulation as circulating tumor cells or may extravasate at a distant site. The extravasated tumor cells form macrometastasis by a reverse mechanism known as MET. EMT, epithelial-mesenchymal transition; MET, mesenchymal-epithelial transition. (Liu, Gu, Shan, Geng, & Sang, 2016)
Using a mouse model of tumor heterogeneity, investigators demonstrated different clones within the heterogeneous population had distinct properties, such as the ability to dominate the primary tumor, or to contribute to metastatic populations, or to enter the lymphatic or vascular systems via vascular mimicry.
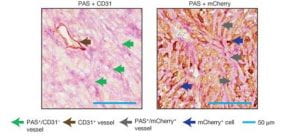
(Wagenblast et al., 2015)
Figure 4. Two adjacent sections of a mouse breast tumor. Tissue at left is stained so that normal blood vessels can be seen (brown arrow). Extending from these vessels are blood filled channels (green arrows). On the right, the tissue is stained for a fluorescent protein expressed by the tumor cells. Here it is seen that blood-filled channels are actually formed by tumor cells in a process known as vascular mimicry. The team demonstrate that the tumor cells lining these channels help drive metastasis, the process by which tumors spread. (Ravindran, 2019)
Invasion by primary tumor cells typically involves the collective migration of large cohesive groups into adjacent tissue rather than the scattering of individual carcinoma cells. However, still unknown are the precise events occurring at the invasive stage. Dormant carcinoma cells called minimal residual disease (MRD) appear to perpetuate carcinogenesis and form the precursors of eventual metastatic relapse and, sometimes, rapid cancer recurrence. Dormant cells have exited the cell cycle and are not proliferating. Thus current treatments that preferentially kill proliferating cells render dormant cells intrinsically more resistant and may remain after initial chemotherapy, radiotherapy, and surgery.
Emerging evidence supports three main prerequisites that must be met for metastatic colonization to succeed: the capacity to seed and maintain a population of tumor-initiating stem cells; the ability to create adaptive, organ-specific colonization programs; and the development of a supportive microenvironmental niche. Metastases may also occur early in the process of neoplastic transformation.
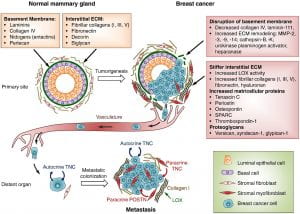
Figure 5 . Extracellular matrix (ECM) changes in breast cancer progression and metastasis. The primary components of the ECM in normal mammary gland are significantly changed in breast cancer. A desmoplastic reaction is associated with breast cancer development, due to the increased production of fibrous ECM by activated fibroblasts and cancer cells. The increased collagen deposition and crosslinking by lysyl oxidase (LOX) enzymes, together with the increased production of fibronectin and other ECM components, stiffens the ECM, which in turn promotes tumor aggressiveness. The basement membrane surrounding the mammary gland epithelium is broken down by ECM remodeling enzymes like MMPs, heparanase and others. Matricellular proteins that promote cancer cell fitness such as tenascin C, periostin, osteopontin, SPARC and thrombospondin-1 are also upregulated. Breast cancer cells from the primary tumor, that include cells with the ability to establish metastatic colonies, enter the blood circulation, disseminate and can reach distant sites. While the vast majority of disseminated cancer cells are eliminated or undergo dormancy due to the adverse environment, few cancer cells are able to resist the selective pressure and establish a metastatic colony. These cells may rely on signals from the ECM such as type I collagen (collagen I), crosslinked by LOX. Tenascin C (TNC) and periostin (POSTN), which are crucial ECM proteins of the metastatic niche, promote stem/progenitor pathways and metastatic fitness in disseminated breast cancer cells. (Insua-Rodríguez & Oskarsson, 2016)
The first clinical manifestation of breast cancer is usually a small, painless lump in the breast. Other manifestations include palpable lymph nodes in the axillae, dimpling of the skin, nipple and skin retraction, nipple discharge, ulcerations, reddened skin, and bone pain associated with bony metastases.
Treatment is based on the extent or stage of the cancer and includes surgery, radiation, chemotherapy, hormone therapy, and biologic therapy.
(Unless otherwise cited, all pathophysiology information was gathered from Danhausen, Phillippi, & McCance, 2019)
- Around the Practice
- Between the Lines
- Contemporary Concepts
- Readout 360
- Insights from Experts at Mayo Clinic on Translating Evidence to Clinical Practice
- Optimizing Outcomes in Patients with HER2+ Metastatic Breast Cancer

- Conferences
- Publications
- Career Center
Clinical Case Presentation: A 36-Year-Old Woman with Breast Cancer and Brain Metastases
- Ruta Rao, MD
Ruta Rao, MD, presents the case of a 36-year-old woman with metastatic HER2+ breast cancer and brain metastases.

EP: 1 . Clinical Case Presentation: A 36-Year-Old Woman with Breast Cancer and Brain Metastases

EP: 2 . Treatment Options in the Frontline Setting for Metastatic HER2+ Breast Cancer
EP: 3 . Second-Line and Third-Line Treatment Options for Metastatic HER2+ Breast Cancer
Ep: 4 . tucatinib for metastatic her2+ breast cancer and brain metastases: patient selection, ep: 5 . treatment options for her2+ breast cancer after progression on tucatinib, ep: 6 . clinical case presentation: a 53-year-old woman with metastatic er/pr+ her2+ breast cancer and brain metastases, ep: 7 . neratinib for metastatic her2+ breast cancer and brain metastases, ep: 8 . leptomeningeal metastases in her2+ breast cancer, ep: 9 . novel agents under evaluation for her2+ breast cancer and brain metastases, ep: 10 . clinical case presentation: a 66-year-old woman with er+ her2+ invasive ductal carcinoma and brain metastases, ep: 11 . trastuzumab deruxtecan treatment for metastatic her2+ breast cancer with brain metastases, ep: 12 . role of neurooncologists in management of her2+ breast cancer and brain metastases.
EP: 13 . Recap: Updates in Treatment of HER2-Positive Breast Cancer and Brain Metastases

31 Adjuvant Abemaciclib Plus Endocrine Therapy for HR+, HER2–, High-Risk Early Breast Cancer: Results From a Preplanned MonarchE Overall Survival Interim Analysis, Including 5-Year Efficacy Outcomes

Applying Updated Breast Cancer Findings From ASCO to Clinical Practice
Neil M. Iyengar, MD, and Paolo Tarantino, MD, discuss updated data on agents such as T-DXd and abemaciclib in breast cancer presented at 2024 ASCO.

Acupuncture Reduces Hot Flashes During Endocrine Therapy for Breast Cancer
Data also show statistically meaningful improvements in endocrine symptoms and breast cancer–specific quality of life with acupuncture.
Finding a Place for Exercise Oncology in the Treatment of Breast Cancer
Neil M. Iyengar, MD, spoke about the potential impact of exercise on patient-reported outcomes in cancer and achieving work-life balance.

33 MammaPrint® and BluePrint® Predict Anthracycline Chemosensitivity in Patients With HR+HER2– Early-Stage Breast Cancer Enrolled in FLEX
34 How Mobile Computing Devices Offer Support for Classic and Molecular Multidisciplinary and Tumor Boards
2 Commerce Drive Cranbury, NJ 08512
609-716-7777


- Get new issue alerts Get alerts
Secondary Logo
Journal logo.
Colleague's E-mail is Invalid
Your message has been successfully sent to your colleague.
Save my selection
The effects of case management for breast cancer patients
A protocol for systematic review and meta-analysis.
Chai, Yong MN a,b ; Li, Li BS a ; Wu, Yun-Lian BS a ; Wang, Tao MN b ; Jia, Yu-Ming BS a ; Lin, Xiao-Li MN b ; Chen, Xi BS a ; Zhong, Hui BS a ; Liu, Li-Xia BS a ; Tao, Lian-De BS a,∗
a The Second People's Hospital of Yibin, Yibin, Sichuan, China
b International School of Nursing, Hainan Medical University, Haikou, Hainan, China.
∗Correspondence: Lian-De Tao, The Second People's Hospital of Yibin, Yibin, Sichuan 644000, China (e-mail: [email protected] ).
Abbreviations: CM = case management, RCT = randomized controlled trial.
How to cite this article: Chai Y, Li L, Wu YL, Wang T, Jia YM, Lin XL, Chen X, Zhong H, Liu LX, Tao LD. The effects of case management for breast cancer patients: a protocol for systematic review and meta-analysis. Medicine . 2022;101:9(e28960).
YC and LL contributed equally to this work.
This project is supported by Sichuan Provincial Science and Technology Department Project of China (22KJPX0021) and Yibin Science and Technology Bureau Project of China (2019SF002). The funders had no role in the design, execution, or writing of the study.
The authors have no conflicts of interest to disclose.
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
This is an open access article distributed under the Creative Commons Attribution License 4.0 (CCBY), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. http://creativecommons.org/licenses/by/4.0
Background:
Female breast cancer is the most common cancer nowadays, and its treatment has a significant impact on patients both physically and psychologically. Many randomized trials have proved that case management (CM) can effectively care for patients. However, there is a lack of systematic scientific evaluation, so this systematic evaluation aims to explore the impact of CM on breast cancer patients.
Methods:
PubMed, Embase, Cochrane Library, Scopus, CINAHL were searched. Chinese repositories included China National Knowledge, Infrastructure Database (CNKI), Wan fang Database, China Biology Medicine Database. We will also search unpublished literature at ClinicalTrials.gov. Randomized controlled trials were collected from them. The literature will be screened according to inclusion and exclusion criteria, and 2 researchers will extract the literature independently. The primary outcome indicator for this study will be patient satisfaction. Statistics were performed using RevMan 5.4 software. The quality of each outcome will be evaluated using the Grading of Recommendations Assessment, Development, and Evaluation.
Results:
This study will provide the most recent evidence for evaluating the impact of CM on breast cancer patients.
Conclusion:
To evaluate the impact of CM on patients with breast cancer.
Registration number:
DOI:10.17605/OSF.IO/ZJKHX.
1 Introduction
According to statistics, female breast cancer has become the most common cancer in the world, with 2.3 million new cases each year, [1] and the incidence rate of which is showing a younger trend, and the current treatment for breast cancer patients is mainly surgery, supplemented by chemotherapy, radiotherapy, targeted and other treatment modalities, [2] so that patients’ survival time is constantly extended. Breast cancer patients, however, have to endure hematoma, infection, skin flap necrosis, chest wall pain, arm complications, and damage to secondary sexual characteristics caused by surgical treatment in addition to the adverse effects of treatment that other cancer patients will face, [3–5] which creates a general sense of uncertainty in breast cancer patients and causes patients to suffer from anxiety, depression, and other adverse emotions, making them suffer from the double blow of physical and psychological disorders, [6] which has a negative impact on patients’ quality of life and disease regression.
To sum up the need for a new model of care that addresses the individual characteristics and needs of the patient and meets the patient's need for long-term supportive care in the form of rehabilitation guidance, information support, and psychological support has become a new challenge in breast cancer care.
According to the Case Management Society of America, the case management (CM) process is a multidisciplinary and collaborative model that includes assessment, planning, implementation, care coordination, monitoring, and evaluation to improve the quality of care through individualized assessment and rational selection of health care resources to meet the supportive care needs of patients and families. [7–9]
CM has now been applied in the disease transition evaluation system for the elderly, which can significantly reduce readmission rates and days in hospital, [10] achieve better results in improving health outcomes in diabetes, chronic obstructive pulmonary disease, and coronary heart disease, [11] and can improve depression levels in cardiac patients to some extent. [12] In breast cancer, studies have shown that patients who participate in CM have lower rates of psychological anxiety and depression and better functional recovery and quality of life of the affected limb after surgery. [13] Some studies have shown that CM can effectively help patients care for their wounds and improve their hospital satisfaction. [14] However, there are limitations in the current CM approaches, which vary in supporting care for breast cancer patients. Some studies have small sample sizes, limited quality, and lack research support from evidence-based medicine, so there is a need to assess the impact of CM on breast cancer patients through systematic evaluation and meta-analysis.
2 Objectives
To explore the impact of CM on breast cancer patients and provide evidence-based clinical care support.
3 Methods and analysis
3.1 study registration.
We are registered at the OSF ( https://osf.io/zjkhx ). The registration number is DOI: 10.17605/OSF.IO/ZJKHX.
3.2 Inclusion criteria
3.2.1 type of research.
- (1) All randomized controlled trials (RCTs) which compared CM with other forms of care for breast cancer will be retrieved and recorded, RCTs selected female adults (participants aged >18 years) without regional and language restrictions.
- (2) Conference papers, reviews, case reports, animal studies, research protocols, supplementary questions, letters will be excluded.
3.2.2 Type of participants
Female patients with a diagnosis of breast cancer are included. Male patients with breast cancer, patients with metastatic breast cancer, patients with previous mental illness, or impaired consciousness will be excluded.
3.2.3 Type of interventions
The trial group will be patients with breast cancer who have received CM.
3.2.4 Types of comparators
Types of comparators: Patients with breast cancer who received conventional care or other methods of care.
3.2.5 Types of outcome measures
3.2.5.1 primary outcomes.
The primary outcome will be the patient satisfaction.
3.2.5.2 Secondary outcomes
The secondary outcomes will be quality of life, pain, depressive disorder, and anxiety.
3.3 Exclusion criteria
Duplicate publications; literature where full text is not available; literature where valid outcomes cannot be extracted; and non-RCT literature.
3.4 Study search
The search includes PubMed, Embase, Cochrane Library, Scopus, CINAHL, and Chinese repositories such as China National Knowledge, Infrastructure Database (CNKI), Wan fang Database, China Biology Medicine Database (CBM). We will also search for unpublished literature at ClinicalTrials.gov. The search strategy will be adjusted to the various databases ( Table 1 ).
| Database | Search strategy |
| PubMed | #1 “breast Neoplasms”[Mesh] |
3.5 Selection of studies
The literature retrieved from the data will be imported into Endnote software (X9.2, Chandler, AZ). After removing duplicates, 2 researchers (YC and LL) will independently screen the titles and abstracts of the literature based on the inclusion criteria, eliminating those that do not meet the requirements. Then 2 researchers will read the full text of the remaining literature for further screening. The original author and the fourth researcher (XLL) will be contacted for evaluation if necessary. The flow of the study is shown in Figure 1 .

3.6 Data extraction and management
All data included in the trial were extracted independently by 2 researchers (YC and LL), recorded on a data extraction form and analyzed for: general information (author information, year of publication, country of publication, and funding); trial-type; participant characteristics; interventions; trial outcomes. In a disagreement between 2 researchers, a third researcher (RLW) will arbitrate, and incomplete data will be provided by contacting the original author.
3.7 Assessment of the methodological quality
We will use the Cochrane risk assessment tool to assess the quality of the RCT trial literature, which consists of 7 items: random sequence generation, allocation concealment, implementation bias, measurement bias, follow-up bias, reporting bias, and other biases. Each risk bias was judged on the following criteria: low risk of bias, high risk of bias, unclear.
3.8 Measures of treatment effect
Data will be analyzed and quantitative data will be synthesized using RevMan V.5.4, London. United Kingdom. Dichotomous variables will be expressed as risk ratios, and continuous variables will be expressed as mean differences or standards mean differences. Evidence-based final effect size estimates and 95% confidence intervals will be given.
3.9 Dealing with missing data
In the case of missing data, attempts will be made to contact the authors to obtain them, and if no response is received, these will be clarified and excluded from the literature.
3.10 Assessment of heterogeneity
We will use chi-square tests and I 2 statistics to test for heterogeneity, using I 2 statistics to determine whether to use a fixed-effects model ( I 2 < 50%) or a random-effects model ( I 2 ≥ 50%), with high heterogeneity being determined when I 2 > 75% and descriptive analyses will be conducted.
3.11 Data synthesis
When the number of included studies exceeds 10, bias will be assessed jointly using funnel plots to observe the symmetry of the funnel plots and to assess the presence of bias. [15]
3.12 Subgroup analysis
Subgroup analysis will be performed if there is sufficient literature included or a high degree of heterogeneity, depending on the type of patient outcome.
3.13 Sensitivity analysis
A sensitivity analysis will be performed using Revman 5.4 software to evaluate the reliability of the meta-analysis. If heterogeneity is high, we will verify the heterogeneity of all included literature 1 by 1, exclude low-quality studies as needed, and then re-run the meta-analysis, comparing the results with the previous meta-analysis. If the results are generally stable, they will be considered reliable.
3.14 Grading the quality of evidence
The quality of evidence for all outcomes was graded and recommended using the Grading of Recommendations Assessment, Development, and Evaluation, which classifies the quality of evidence as high, moderate, low, or very low. Evidence from RCT will start at high quality and be selected to be downgraded by 1 or 2 levels depending on risk factors such as the risk of bias, imprecision, inconsistency, indirectness, and publication bias. [16,17] The level of recommendation in Grading of Recommendations Assessment, Development, and Evaluation is divided into strong and weak recommendations based on the level of certainty of the evidence, the desirability of the results, the strength of patient values and willingness, or the cost of resources. [18]
3.15 Ethics
The study was approved by the hospital ethics committee and did not require ethical approval.
4 Discussion
Breast cancer is by far the most common malignancy and the leading cause of death among female oncology patients, [19] and its prevention and treatment is an essential issue in public health. The multiple treatment modalities for breast cancer may lead to patients experiencing pain, infection, and lymphedema, which significantly reduces their quality of life. [20] Numerous care programs have emerged, but few of them, like CM, concentrate on pre-admission assessment, pre-operative guidance, postoperative care, multidisciplinary consultations, psychological support, physical rehabilitation, discharge continuity of care, etc. Although some RCTs have demonstrated that CM can improve the patient experience, there is a lack of systematic scientific evaluation of the impact of CM on breast cancer patients, so this paper aims to provide evidence-based evidence of its effectiveness. This review also has some limitations. however, as differences in the level of CM may lead to heterogeneity, and there may be incomplete results due to the inability to contact the authors.
Author contributions
Conceptualization: Yong Chai, Yun-Lian Wu, Lian-De Tao.
Data curation: Yong Chai, Li Li.
Formal analysis: Yu-Ming Jia, Xiao-Li Lin.
Methodology: Xi Chen, Hui Zhong.
Software: Li-Xia Liu.
Supervision: Tao Wang.
Writing – original draft: Yong Chai, Li Li.
Writing – review & editing: Yun-Lian Wu, Lian-De Tao.
- Cited Here |
- PubMed | CrossRef |
- Google Scholar
- View Full Text | PubMed | CrossRef |
case management; breast cancer; protocol; systematic review
- + Favorites
- View in Gallery
How Breast Cancer Risk Assessment Tools Work
June 27, 2024 , by Sharon Reynolds

After using a breast cancer risk assessment tool, people should talk with their doctor about what the risk estimates mean for them, NCI experts advised.
In March 2024, the actress Olivia Munn announced that she had been diagnosed with breast cancer. Ms. Munn also highlighted the role a cancer risk assessment tool played in the process that led to her diagnosis. In this Q&A, Ruth Pfeiffer, Ph.D., and Peter Kraft, Ph.D., of NCI’s Division of Cancer Epidemiology and Genetics discuss how these tools are created and how people can use them to understand and manage their risk.
Can cancer risk assessment models predict whether an individual woman will develop breast cancer?
Dr. Pfeiffer: Women want to know: Will I get breast cancer? Unfortunately, these models cannot predict the future with certainty for any one individual. They present population averages.
For example, if a woman’s risk estimate over a predefined time period is 5%, that means that out of 100 women who have the same risk factors as her, such as age and family history of breast cancer, 5 will develop breast cancer over that period. But we can’t identify the exact 5 women out of that 100 who will develop breast cancer.
Dr. Kraft: And it’s important to remember that these estimates of risk do not guarantee a specific outcome . So, you could have a relatively high-risk value on a given tool, but that doesn’t necessarily mean you will get breast cancer. And just because you have a low value doesn’t mean you won’t get breast cancer.
Dr. Pfeiffer: No woman should think, “I don’t need to get screened because my breast cancer risk is low.” On the flip side, there is no need to panic if her risk is high.
There are multiple breast cancer risk models out there. How are they different?
Dr. Pfeiffer: One big difference is the [risk] factors the models consider. In addition, some take into account that a woman might die from causes other than breast cancer. NCI’s risk assessment models for breast cancer, colorectal cancer, and melanoma do this. Other models estimate what we call pure risk: the probability that a woman will get breast cancer if she couldn’t die from anything else. These models produce higher estimates of risk.

Ruth Pfeiffer, Ph.D.
DCEG Biostatistics Branch
All models use slightly different information, but all models use information on factors that have been shown to be associated with breast cancer risk. They consider things like a woman’s family history of cancer, number of childbirths and her age at those births, and whether she has had a benign breast disease . Benign breast diseases are conditions that may show up on a mammogram and lead a woman to have a biopsy, but they are not breast cancer.
These factors do not necessarily cause breast cancer, but, for whatever reason, they predict one’s risk of breast cancer.
What can people do with the information from a risk assessment tool?
Dr. Kraft: It’s really important that they talk with a health care provider about what the risk estimates mean for them. That’s the opportunity to discuss: Am I at high risk? If so, what can I do about it? What are the recommendations for me?
Dr. Pfeiffer: There are also breast cancer risk prediction models out there that include potentially modifiable risk factors, like body mass index , alcohol consumption, and hormone replacement therapy use. So someone could play around with these factors and ask: What would be my risk if I did not drink alcohol? Or if my body mass index was in the normal range ? That could help someone make personal decisions about certain lifestyle changes.
Other decisions, like those about screening or taking medications that can reduce your cancer risk, which can come with side effects, need to be made together with a health care provider. But that shouldn’t deter anybody from going online and just seeing what their risk is.
Knowledge is power. And that knowledge could encourage women to reach out to their [health care provider] for help putting such information in context.
What is NCI doing to make risk models more useful or accurate?

Peter Kraft, Ph.D.
Director, DCEG Trans-Divisional Research Program
Dr. Kraft: The NCI Breast Cancer Risk Assessment Tool and others like it use factors that people know about themselves. They don’t include the risk that you may have from your genetic makeup.
Unfortunately, most studies of the inherited risk of breast cancer have been done in people of European ancestry. These genetic studies have not had large numbers of Black Americans, Latinos, Asian Americans, or Pacific Islanders, for example. Models that incorporate genetic information, such as whether someone has certain gene changes, may not perform as well in these population groups.
At NCI we’ve launched the Confluence Project , which is looking at the genetics of breast cancer across diverse populations.
One of Confluence’s main tasks is to increase the sample size from diverse groups. This can improve model performance for everybody, but especially for people who have been historically excluded from genetic studies.
Then, the Breast Cancer Risk Prediction Project is bringing together the new genetic results from Confluence with some of the existing models.
Dr. Pfeiffer: The more data we have, and the more representative those data are of the populations in which we would use a model, the better that model will perform.
For example, NCI researchers developed a breast cancer risk model for Hispanic women . That model distinguishes between Hispanic women born in the United States and those born in other countries, because the data we have tell us that their risks are different.
Learn more about breast cancer risk .
Featured Posts
June 5, 2024, by Linda Wang
May 3, 2024, by Carmen Phillips
May 1, 2024, by Edward Winstead
- Biology of Cancer
- Cancer Risk
- Childhood Cancer
- Clinical Trial Results
- Disparities
- FDA Approvals
- Global Health
- Leadership & Expert Views
- Screening & Early Detection
- Survivorship & Supportive Care
- February (6)
- January (6)
- December (7)
- November (6)
- October (7)
- September (7)
- February (7)
- November (7)
- October (5)
- September (6)
- November (4)
- September (9)
- February (5)
- October (8)
- January (7)
- December (6)
- September (8)
- February (9)
- December (9)
- November (9)
- October (9)
- September (11)
- February (11)
- January (10)

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Wiley Open Access Collection
The hidden breast lesions: A case report of bilateral breast cancer
Chaochao dai.
1 Department of Ultrasonography, Affiliated Hangzhou First People's Hosptital, Zhejiang University School of Medicine, Hangzhou China
Lingyun Bao
Yanjuan tan, chenxiang jiang, associated data.
All data and images generated or used during the study appear in the submitted article.
Bilateral breast cancer (BBC) is rare and is associated with an unfavorable prognosis. Consequently it is crucial to improve diagnostic performance of breast cancer in the clinical setting. We report a case of BBC in a 66‐year‐old woman and describe the imaging findings, including mammography, hand‐held ultrasound, automated breast ultrasound, anatomical intelligence for breast ultrasound (AI‐breast), and magnetic resonance imaging. Only AI‐breast ultrasound successfully located the two tumors, while other imaging examinations failed to detect the tumor in the right breast.
AI Breast successfully located the two tumors, while in the automated breast ultrasound scanning, HHUS scanning and MRI examination, the tumor in the right breast was miss‐detected. we evaluated the efficiency of AI Breast in breast lesion scanning and detection was investigated.

1. INTRODUCTION
The occurrence of bilateral breast cancer (BBC) is increasing nowadays with a reported incidence ranging between 1.4% and 12%. 1 , 2 However, in recent literature, patients with BBC showed a significantly worse distant relapse‐free survival (RFS) as compared to those with unilateral breast cancer (UBC), as distant metastases were frequently reported in patients with BBC. 2 , 3 Early detection and treatment of BBC is important to improve the overall prognosis of patients with breast cancer.
2. CASE REPORT
A 66‐year‐old female patient with a palpable mass in the left breast found by self‐examination came to our hospital for further investigation. Mammographic findings from another hospital included focal asymmetric density in the upper inner quadrant of the left breast. The patient had annual breast cancer screening by hand‐held ultrasound (HHUS), but no breast lesions were found in the past 3 years. There was no family history of breast cancer. The patient had a history of total hysterectomy for endometrioid adenocarcinoma, and partial thyroidectomy for thyroid adenoma and nodular goiter. The values of CA125 and CEA were normal.
Physical examination identified a less mobile, hard mass with unclear border measuring 15 mm in diameter in the upper inner quadrant of the left breast. The examinations of the right breast and axillary lymph nodes were unremarkable. With these clinical examination findings, there was suspicious indication for surgery. The combination of HHUS and automated breast ultrasound scanning was recommended for further evaluation. Automated breast ultrasound scanning was used to acquire datasets for two‐view scans: the lateral and the anteroposterior (AP) view. By reviewing the acquired scanning datasets, an ill‐defined heterogeneous hypoechoic zone (18 × 13 × 18 mm) with posterior acoustic shadowing was observed in the 10‐ to 11‐o'clock position, 7 cm away from the nipple of the left breast. There were no microcalcifications, architectural distortion or mass within the territory (Figure 1 ). The convergence sign was not observed on the coronal plane. No lesion was detected in the right breast. By conventional HHUS, color Doppler was performed on the hypoechoic lesion in the left breast and no internal color flow signals were detected. Elastography resulted in a Tsukuba stiffness score of 3 (Figure 2 ). According to the Ultrasound Breast Imaging Reporting and Data System (BIRADS), the lesion was classified as BIRADS 4A.

The left breast lesion in automated breast ultrasound (US). The left anteroposterior view reveals a non‐mass‐like breast lesions in the 10‐ to 11‐o'clock position 7 cm away from the nipple (blue arrows)

Ultrasonic finding of the left lesion by hand‐held ultrasound (HHUS). (A) Color Doppler sonogram shows no internal vascularity within the lesion. (B) Gray‐scale transverse view of the left breast demonstrates a heterogeneous hypoechoic lesion in the 10 o'clock position. (C) Elastography revealed a Tsukuba stiffness score of 3
The US Department was running a prospective clinical trial to study the efficiency of AI‐breast and HHUS in breast lesion screening. This patient met the inclusion criteria and agreed to participate in the trial. Therefore, AI‐breast scanning was additionally performed on the patient to detect breast lesions. The general radiologist interpreting the scan images and a technician for AI‐breast were both blinded to the results of other US examinations. In AI‐breast scanning, besides the same lesion detected in the left breast (Figure 3A ), another lesion was detected in the right breast (Figure 3B ). The lesion located in the 2‐o'clock position 7 cm away from the nipple of the right breast was irregular and indistinct with posterior acoustic shadowing. Calcifications observed within the mass were mostly macro‐calcifications.

Ultrasonic findings of the bilateral breast lesions by AI‐breast US. (A) A heterogeneous hypoechoic lesion detected in the left breast in the 10‐ to 11‐o'clock position 6 cm away from the nipple. (B) A nodule with calcifications within the mass detected in the right breast in the 2‐o'clock position 7 cm away from the nipple
Upon reviewing the data of the AP view of the right breast, a nodule which was not whole was observed on the edge of the 2 o'clock position. The patient was recalled for second‐look US on the right breast and the medial view was added. With reference to the position of the lesion located by AI‐breast scanning, a hypoechoic nodule (8 × 5 × 6 mm) in the right breast with calcifications in the mass was detected (Figure 4 ), which was irregular, indistinct and parallel to the chest wall. Similar ultrasonic findings were observed which were consistent with the findings of AI‐breast ultrasound. No vessel was detected by color Doppler scanning. The lesion in the right breast was finally classified as BIRADS 4A.

Ultrasonic finding of the right lesion by HHUS and automated breast US. (A) An irregular and indistinct hypoechoic nodule with calcifications detected in the 2‐o'clock position of the fat layer. (B) Color Doppler US reveals no internal color flow signals. (C) Elastography revealed a Tsukuba stiffness score of 2. (D, E) Anteroposterior (AP) view and medial (MED) view by AI‐breast US demonstrates a hypoechoic nodule 7 cm away from the nipple of the right breast (blue arrows), but only part of the lesion is shown on AP view
To further confirm the surgical plan, a recommendation was made for contrast‐enhanced magnetic resonance imaging (MRI) examination. MRI revealed an irregular zone (22 × 12 × 12 mm) with focal heterogeneous non‐mass enhancement in the left breast (Figure 5A ). The time–signal intensity curve (TIC) showed a type II enhancement curve (plateau pattern, Figure 5B ). On the maximum signal intensity projection image, enlarged blood vessels were observed surrounding the lesion in the left breast and mild diffusion limitation was found on the diffusion‐weighted image (Figure 5C and D). Based on all the MRI findings, the lesion in the left breast was classified as BIRADS 4. No characteristics suggestive of malignancy were observed in the right breast.

Findings of MRI examination. (A) An area of non‐mass enhancement is detected. (B) A type II enhancement curve is observed. (C) Maximum signal intensity projection image indicates enlarged blood vessels surrounding the lesion in the left breast. (D) Diffusion‐weighted imaging examination reveals mild diffusion limitation
US‐guided biopsy was performed on the two lesions, and histological examination results revealed both were invasive breast carcinoma (non‐special type, NST). The patient underwent double mastectomy, and intraoperative sentinel node biopsy was negative. Surgical specimens of the lesions were stained for pathological confirmation. The lesion in the left breast was invasive breast carcinoma (NST) measuring 14 mm (stage III, Figure 6 ) and the lesion in the right breast was also revealed to be invasive breast carcinoma (NST) measuring 6 mm (stage II, Figure 7 ).

Pathologic findings of the left breast lesion. Microscopic examination shows an invasive breast carcinoma measuring 14 mm (stage III, hematoxylin and eosin stain, ×200)

Pathologic findings of the right breast lesion. Microscopic examination shows an invasive breast carcinoma measuring 6 mm (stage II, hematoxylin and eosin stain, ×200)
3. DISCUSSION
The patient had BBC with one palpable tumor located in the marginal area of the upper inner quadrant of the left breast and one non‐palpable tumor located in the marginal area of the upper inner quadrant of the right breast. As described, AI‐breast US successfully located the two tumors, while automated breast ultrasound scanning, HHUS scanning, mammography (MG) and MRI examination all failed to detect the tumor in the right breast.
By MRI examination, no area with an enhancement pattern for malignancy was observed in the right breast, therefore no tumor in the right breast was reported. The macro‐calcifications and untypical blood flow of the tumor might lead to mis‐detection or mis‐diagnosis by MRI. 4 , 5 As reported, the diagnostic performance of the two‐view scan technique in automated breast ultrasound was similar to the results of three‐view scans in women with small breasts. In this case, the two‐view scan was chosen because the patient had a breast cup size of B. The medial coverage was considerated to be proper in AP view because there was absence of abrupt cutoff of the fibroglandular tissue at the margin of view and including the fatty tissue. 6 , 7 But the lesion of right breast was located in the fatty tissue far from the nipple, with a second reading of the scanning data by automated breast ultrasound, only part of the lesion in the right breast was shown in AP view. Women with dense breasts have been found to have a lower detection rate of breast cancer by MG due to the masking effect of dense tissue in Asian women. Some subtle MG findings or other lesions present in a marginal anatomic area have therefore been overlooked or misinterpreted. 8 , 9
The bilateral breast lesions were missed by HHUS screening at another hospital. The accuracy of breast screening is related to the radiologist's experience. In this case, the most important reason for missed diagnosis of the left breast lesion was the lack of understanding of a non‐mass lesion, which is defined as a discrete and identifiable area which shows altered echotexture compared with that of the surrounding breast tissue and does not conform to a mass shape. The failure to detect the tumor in the right breast by HHUS screening might be caused by atrophy of the patient's breast glands and the particular position of the tumor. The tumor was located in the marginal area of the breast and no obvious glandular tissue was observed surrounding it. In breast US scanning, the general radiologist usually takes the margins of glandular tissue as reference to identify the margins, leading to insufficient coverage. Another reason for the mis‐detection might be that the sonographers were more focused on evaluation of the palpable tumor in the left breast due to the relative low incidence of BBC and evaluation of the right breast was therefore lax. Standardized scanning reducing human errors or biases are important in breast US scanning. 10 , 11 , 12
AI‐breast US 13 is a standardized breast scanning technique based on conventional 2D US scanning and electromagnetic tracking and positioning technology by introducing a mattress electromagnetic field generator and integrating tracking coils in the transducer. AI‐breast US provides a calibrated GPS map of the scanned images in relation to the breast anatomy to document full coverage of the breast during the acquisition phase. In this case, for AI‐breast scanning, the technician utilized the up/down scanning leveraging experiences from automated breast ultrasound scanning. With the intuitive tool of AI‐breast to visualize the scanning procedure by brushing the screened areas green and displaying the result in a thumbnail of the breast anatomy, full coverage of the breast was ensured during scanning. By reviewing the scanning data without any blind areas, the two tumors were successfully detected. Compared with conventional HHUS, AI‐breast US firstly increases the diagnostic confidence of US doctors by reducing blind areas during scanning and also speeds up the workflow by the use of intuitive tools. Secondly, AI‐breast reduces dependence on the examiner's experience in breast US scanning by adopting standardized scanning technology which is easy for technicians to master. Thirdly, all of the breast US scanning data can be recorded in AI‐breast, including auto‐annotation of the lesion information, bookmarks of key frames within the loop, and quick access to the orthogonal plan from a reference point, which makes the longitudinal follow‐up of patients with breast lesions more convenient.
Cases of BBC are rare, and early diagnosis, which can significantly improve disease‐specific survival, depends on breast imaging. The most common method of screening for breast cancer in Asian women is US, but the performance of ultrasonologists varies to a large extent. Unlike HHUS, AI‐breast US uses a reproducible and less operator‐dependent process for image acquisition. In this case, AI‐breast US demonstrated its value in the detection of BBC, indicating its advantages in the diagnosis and follow‐up of patients with bilateral breast lesions. Meanwhile, with the trial to separate the screening procedure and detection or diagnosis procedure in this study, AI‐breast may initiate new workflows for breast US examination to improve coverage. Misdiagnosis and missed diagnosis are common in cases of BBC because of lack of attention to the contralateral breast after observation of a suspect lesion. Sonographers must not be satisfied with finding just one lesion, but must search carefully for others, whether ipsilateral or contralateral.
Dai C, Bao L, Tan Y, Jiang C. The hidden breast lesions: A case report of bilateral breast cancer . J Clin Ultrasound . 2022; 50 ( 3 ):422‐427. doi: 10.1002/jcu.23117 [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
Chaochao Dai is the first author.
Funding information This work is supported by the Construction Fund of Medical Key Disciplines of Hangzhou.
DATA AVAILABILITY STATEMENT
No end in sight as record-breaking heat wave continues
The heat caused a road in Washington to buckle, officials said.
The ongoing scorching heat in the West caused a road to buckle in Washington this week while at least a dozen California cities broke all-time high-temperature records.
A heat wave enveloping much of the nation has been especially sweltering on the West Coast, where some areas have experienced multiple days of triple-digit weather that has turned deadly.
More than 70 million people are under heat alerts in the West as a scorching heat wave continues.

In Oregon, the Multnomah County Medical Examiner's Office reported Monday that it is investigating at least four suspected heat-related deaths since the state of emergency was declared on July 5 amid dangerously hot temperatures.
Those who perished in the soaring heat included an 87-year-old man, a 75-year-old man and a 64-year-old man, all living in the Portland area, the medical examiner's office said. A 33-year-old man was taken to a Portland hospital from outside Multnomah County, and also died from a suspected heat-related illness.

The temperature hit 101 degrees in Portland on Monday and 104 degrees in Eugene and Salem, Oregon, according to the National Weather Service (NWS). All three cities set new daily high-temperature records, the weather service said.
Portland is forecast to see its fourth straight day of triple-digit weather on Tuesday, where thermometers are expected to climb to 105 degrees, according to the NWS.
Road buckles in Washington
In Washington, extreme temperatures caused State Route 111 in Skagit County to buckle on Monday, creating potentially dangerous conditions for drivers, according to the Washington State Department of Transportation.
"Our crews were dispatched and found that the concrete panels under the asphalt had buckled due to the heat," Madison Sehlke, a spokesperson for the Washington State Department of Transportation, told ABC affiliate station KOMO in Seattle.

Washington saw temperatures on Monday climb to the high 90s in some areas. In Olympia, the temperature hit 99 degrees on Monday, breaking a daily record set in 2010, according to the National Weather Service. Seattle also broke a daily temperature record on Monday when the temperature reached 91 degrees, according to the NWS.

Excessive heat warnings in most of California
The entire state of California was either under an excessive heat warning or a heat advisory on Tuesday.
Palm Springs, which set an all-time heat record on Sunday when the temperature peaked at 124 degrees, was forecast to reach 121 degrees on Tuesday, according to the NWS.

A long-duration heat wave is expected to continue through this week in California's Central San Joaquin Valley.
Fresno is forecast on Tuesday to see its seventh straight day of temperatures hitting 105 degrees or higher, Andy Bollenbacher of the NWS office in Hanford, California, told ABC News.
MORE: Video Extreme heat blamed for a bridge being stuck open across Harlem River
Bollenbacher said the record for consecutive days of 105 degrees or higher in Fresno is 14. He said the extended forecast shows a temperature in Fresno of 105 degrees or higher lasting through at least Sunday.
The temperature on Tuesday in Fresno is forecast to hit 109 degrees, Bollenbacher said.
Death Valley, California, remains the hottest spot in the nation. At 11 a.m. local time on Tuesday, the temperature in Death Valley was 112 degrees and forecast to reach 128, according to the NWS.

The highest temperature ever recorded in Death Valley was 134 degrees set in 1913, which is also the highest temperature ever recorded on Earth, according to the NWS.
At least 12 cities in California have seen all-time heat records broken since Saturday, including Redding in Northern California which hit 119 degrees on Monday and Dagget in Southern California which reached 118 on Sunday, according to the National Weather Service.
Dangerous heat to drag on in Arizona
Oppressive heat is forecast to continue through the remainder of the week in Arizona, where an excessive heat warning was extended for the Phoenix metro area.
In Phoenix, the temperature is expected to peak at 117 degrees on Tuesday and remain above 109 degrees through at least Monday, according to the NWS. Lake Havasu City is forecast to hit 120 degrees on Tuesday, Wednesday and Thursday before cooling down to 117 on Friday and 110 on Sunday, according to the NWS.
A 50-year-old man hiking in the Grand Canyon died after being found unresponsive over the weekend, marking the third death in the national park within the last three weeks.

A man was unresponsive when he was found on the Bright Angel Trail in the Grand Canyon about 100 feet from the trailhead on Sunday, according to the Grand Canyon Regional Communications Center.
NPS said temperatures on exposed parts of the trail can reach over 120 degrees in the shade.
Las Vegas expected to break consecutive hot-day record
Just days after recording its hottest day ever, Las Vegas is aiming to break another record: consecutive days of 110 degrees or higher.
The NWS is forecasting high temperatures of 114 to 118 degrees for the rest of this week, putting Las Vegas in a position to break the current record of five straight days of 110 degrees or higher.
Las Vegas has a 90% chance of breaking its all-time record for consecutive days of 110 degrees or above, meteorologist Matt Woods of the NWS office in Las Vegas told ABC News.
MORE: Rescue underway for 13 hikers trapped in fire zone
Tuesday's temperature in Las Vegas is forecast to reach 117, making it the seventh straight day it surpassed the 110-degree mark, Woods said.
Las Vegas' record of 10 consecutive days of 110-degree weather was set in 1961 and tied in July 2023.
"Tomorrow through Saturday we have a 90% chance of reaching a 110," Woods said. "So it's very likely we're going to shatter the record."
On Sunday, Las Vegas reached 120 degrees, breaking the record for the city's hottest day ever.
Hot weather in other parts of the nation
By this weekend, the record heat will move into the Rockies, where cities like Denver, Colorado, and Rapid City, South Dakota, could see record highs.
Numerous cities along the East Coast are forecast to hit the century mark or get close.
In Washington, D.C., the temperature hit 98 degrees on Tuesday afternoon and is forecast to reach 96 degrees on Wednesday. Philadelphia hit 94 degrees on Tuesday afternoon. Further south, the temperature Tuesday afternoon in Richmond, Virginia, climbed to 95 degrees and it was 94 in Charlotte, North Carolina, according to the NWS.
Related Topics
Trending reader picks.

1st look at rarely-seen rooms of Buckingham Palace
- Jul 9, 7:01 PM

Scientists find exoplanet smells of rotten eggs
- Jul 9, 7:30 PM

Americans coast-to-coast sweat out heat wave
- Jul 10, 6:28 PM

US-built pier to be put back in Gaza, then removed
- Jul 9, 3:08 PM

Expert tips to avoid dehydration
- Jul 10, 9:02 AM
ABC News Live
24/7 coverage of breaking news and live events
IMAGES
VIDEO
COMMENTS
Trends in neoadjuvant endocrine therapy use and impact on rates of breast conservation in hormone receptor-positive breast cancer: a National Cancer Data Base study. Ann Surg Oncol 2017;24:418-424 ...
Presentation of Case. Dr. Kevin S. Oh (Radiation Oncology): A 45-year-old woman was evaluated in the oncology clinic of this hospital because of metastatic triple-negative breast cancer. The ...
Background. Worldwide, male breast cancer is extremely rare, accounting for <1% of all breast tumors and <1% of all malignancies in men [1-3].Recently, the incidence of male breast cancer has increased from 1.0 per 100,000 men in the late 1970s to 1.2 per 100,000 men from 2000 to 2004 [4-7].The American Cancer Society reported a similar trend in the incidence of breast cancer in men from ...
n engl j med 390;21 nejm.org June 6, 2024 2013 Case Records of the Massachusetts General Hospital home with planned follow-up in the oncology clinic.
Carol Edwards, a 39 year-old premenopausal woman, had a screening mammogram which revealed an abnormality in the right breast. She had no palpable masses on breast exam. A mammographically localized surgical biopsy was done and revealed a small (0.9 cm) grade III infiltrating ductal carcinoma with some associated ductal carcinoma-in-situ (DCIS ...
The WISDOM study, run by the Athena Breast Health Network, uses these distributions to establish a threshold of the top 2.5% of risk for each age group to initiate counseling on prevention interventions and annual screening. ... We conducted a case-case analysis of women treated for invasive breast cancer at the University of California San ...
The incidence of breast cancer is growing rapidly worldwide (1.7 million new cases and 600,000 deaths per year). Moreover, about 10% of breast cancer cases occur in young women under the age of 45. The aim of the study was to report a rare case of BRCA 1-mutated breast cancer in a young patient with multiple affected relatives.
1 Introduction. Breast cancer remains the most common cancer diagnosed among women in the United States and is the second leading cause of cancer-related deaths, with approximately 41,000 patients projected to die from this disease in 2018 alone. The prognosis for patients with metastatic breast cancer varies based on many factors including estrogen receptor (ER), progesterone receptor (PR ...
Case: Inflammatory Breast Cancer Sub-navigation. Cases. Accessory Breast Tissue. Architectural Distortion. ... Inflammatory breast cancer accounts for approximately 1-3% of all breast cancers. An average age at diagnosis ranges between 55-58 years. ... CA Cancer J Clin. 2010 Nov-Dec;60(6):351-75.
Breast cancer (BC) is the prevailing malignancy among women, with HER2 overexpression observed in 20-30% of all BC, thereby serving as a prognostic indicator for unfavorable outcomes in affected individuals. There is a necessity to establish innovative treatment protocols to expand the therapeutic alternatives accessible for managing HER2-positive BC. In this study, we report a case of HER2 ...
A healthy female breast is made up of adipose tissue (fat cells) and lobes. The lobes contain many lobules. Lobules are responsible for milk production in lactating women. The lobes and lobules are connected via milk ducts (National Breast Cancer Foundation INC, 2019). All together, this system is responsible for transporting milk to the nipple.
The goal of this activity is for learners to be better able to select the most optimal anti-HER2 treatments for patients with HER2-positive breast cancer at every stage of care. Upon completion of this activity, participants will: Have increased knowledge regarding the. Clinical data associated with emerging anti-HER2 regimens for patients with ...
Breast Cancer [Case Study] If you have a disability and experience difficulty accessing this content, please email [email protected] or call 614-292-5000 for assistance. The content of this site is published by the site owner(s) and is not a statement of advice, opinion, or information pertaining to The Ohio State University.
Pathophysiology of Breast Cancer. Except for skin cancer, breast cancer is the most common cancer in American women. Most breast cancer occurs in women older than 50 years. The major risk factors for breast cancer are classified as reproductive, such as nulliparity and pregnancy-associated breast cancer; familial, such as inherited gene ...
Case Study Mrs. Whitney Breast CA. Client Profile Mrs. Whitney is a 45-year-old black American woman, married mother of two children, ages 10 and 12 years old. She noticed a lump in her left breast during her monthly breast self-exam two weeks ago. She made an appointment with her gynecologist who documents "a fixed round lump with irregular ...
The Playback API request failed for an unknown reason. EP: 1. Clinical Case Presentation: A 36-Year-Old Woman with Breast Cancer and Brain Metastases. EP: 2. Treatment Options in the Frontline Setting for Metastatic HER2+ Breast Cancer. EP: 3. Second-Line and Third-Line Treatment Options for Metastatic HER2+ Breast Cancer.
This patient's breast cancer is negative for ER and PR. Immunohistochemistry staining results for HER-2 are shown in Figure 3. HER-2 IHC is scored as 2+ (equivocal) for HER-2, demonstrating weak to moderate complete membrane staining in >10% of tumor cells. Due to this result, the sample is tested reflexively by FISH.
The effects of case management for breast cancer patients: a protocol for systematic review and meta-analysis. Medicine. 2022;101:9 (e28960). YC and LL contributed equally to this work. This project is supported by Sichuan Provincial Science and Technology Department Project of China (22KJPX0021) and Yibin Science and Technology Bureau Project ...
Case study breast cancer - Download as a PDF or view online for free. ... Blood Marker Tests • Examples of markers include: • CA 15.3: used to find breast and ovarian cancers • TRU-QUANT and CA 27.29: may mean that breast cancer is present • CA125: may signal ovarian cancer, ovarian cancer recurrence, and breast cancer recurrence ...
Abstract and Figures. In this case study, a women aged 40 was diagnosed with Metastatic breast cancer. Metastatic breast cancer is a complex multi-stage disease involving the expansion of ...
Case Study Breast CA - Free download as PDF File (.pdf), Text File (.txt) or read online for free. ... The case study objectives are to develop a patient-centered care plan, apply knowledge throughout treatment, identify risk factors, modify lifestyle needs, and understand the patient's condition. The patient health history outlines a 53-year ...
There are multiple breast cancer risk models out there. How are they different? Dr. Pfeiffer: One big difference is the [risk] factors the models consider. In addition, some take into account that a woman might die from causes other than breast cancer. NCI's risk assessment models for breast cancer, colorectal cancer, and melanoma do this.
BREAST CA Case Study - Free download as Word Doc (.doc / .docx), PDF File (.pdf), Text File (.txt) or read online for free. "Breast cancer" refers to a malignant tumor that has developed from cells in the breast. Breast cancer is always caused by a genetic abnormality. Only 5-10% of cancers are due to an abnormality inherited from parents.
Case Study 92 Breast Cancer. Describe the biopsy technique used to diagnose M.'s cancer. The type of biopsy used to diagnose M.'s cancer would be a breast biopsy. In a breast biopsy the extra tissue in the suspected area is removed and analyzed. After the tissue is analyzed under microscopic studies, a diagnosis of cancer can be given.
Abstract. Bilateral breast cancer (BBC) is rare and is associated with an unfavorable prognosis. Consequently it is crucial to improve diagnostic performance of breast cancer in the clinical setting. We report a case of BBC in a 66‐year‐old woman and describe the imaging findings, including mammography, hand‐held ultrasound, automated ...
Tracy Werthman and Nikoma Echt, both of West Seattle, and their kids cool off at Alki Beach as an excessive heat warning remains in effect a day after record-breaking temperatures hit the region ...
Large-Scale Prescribed Fire Incident Mobilization: A Case Study on the Stanislaus National ... was able to procure yurts from the Southern California Interagency Support Cache. However, unlike the yurts provided through VIPR contracts, these yurts did not come with generators, power cables, spider boxes, and HVAC systems, which created more ...